
 Click here for the new Anchor Rising & Ocean State Current page
Click here for the new Anchor Rising & Ocean State Current page

Socking It To the Insurance Co or To The Insured? Rhode Island Has the Highest Number of Health Insurance Mandates , by Monique Chartier
Healthcare
9:46 AM, 04/17/13
Health Benefits Exchange: What They Mean by Self-Sustaining, by Justin Katz
Healthcare
10:19 AM, 04/ 8/13
Premium Premiums? RI Employers Paying Higher Than National Average For Employee Health Coverage, by Monique Chartier
Healthcare
9:01 AM, 12/24/12
Things We Read Today (44), Wednesday, by Justin Katz
Pensions
6:19 PM, 12/19/12
Things We Read Today (42), Weekend, by Justin Katz
Civil Liberties
8:01 AM, 12/17/12
Gary Alexander's Long Commute and Rhode Island's Big Compensation, by Justin Katz
Public Service
12:00 PM, 12/14/12
The Philosophy of Noose Tightening, by Justin Katz
Economy
7:54 AM, 12/ 7/12
Things We Read Today (35), Tuesday, by Justin Katz
Healthcare
5:37 PM, 11/27/12
RI Governor Gives Nation a Preview of Obama’s Public Welfare Project, by Justin Katz
Under the Government's Wing
8:00 AM, 10/ 9/12
Things We Read Today (23), Wednesday, by Justin Katz
Healthcare
8:28 AM, 10/ 4/12
April 17, 2013

Socking It To the Insurance Co or To The Insured? Rhode Island Has the Highest Number of Health Insurance Mandates
To set the stage:
- This Wall Street Journal summary map indicates that Rhode Island has the seventh highest per capita health-care spending.
- In filings Monday, Blue Cross Blue Shield of RI requested an increase in health insurance premiums - an 18% increase for individuals (note that Blue Cross is the only company in the state that offers health insurance to individuals) and a 15% increase for small groups. It is not immediately clear how much of this is due to the implementation of ObamaCare.
- Speaking of ObamaCare, the cost of state health insurance exchanges, the tool that was supposed to lower health insurance costs, has been rising, adding to indirect costs of health care.
- A week ago, GoLocalProv reported that Rhode Island is
Among Worst States for Competitive Healthcare
Now we can perhaps identify a significant contributory factor for that last item and for the high (and rising) cost of health care in the state. Last week, the Council for Affordable Health Insurance (CAHI) released a report and ranking of "Health Insurance Mandates in the States, 2012." Once again, Rhode Island finds itself on the top of a dubious list - in this case, most number of mandated health insurance benefits.
Compelling the nasty insurance companies (what few there are in Rhode Island) to cover the maximum number of benefits sounds like a good idea in theory. The reality is that such mandates translate directly into costs, which get passed on to the customer/rate payer. From the CAHI report:
“One of the biggest cost drivers in our health care system is the steady proliferation of federal and state-based coverage mandates. When CAHI started tracking mandates in 1992, there were about 850 mandates across all 50 states,” explained CAHI Research and Policy Director, Victoria Craig Bunce. “Over the last twenty years the number of state mandated benefits has grown to 2,271. That’s an increase of 167 percent! Based on our annual analysis, mandated benefits currently increase the cost of basic health coverage from slightly less than 10 percent to more than 50 percent, depending on the state, specific legislative language, and type of health insurance policy.”
[Monique is Editor of the RI Taxpayer Times newsletter.]
April 8, 2013

Health Benefits Exchange: What They Mean by Self-Sustaining
Amidst the political noise of news on marriage, immigration, and guns, Phil Marcelo has an informative article in today's Providence Journal highlighting the fact that the State of Rhode Island is going to have to pay to maintain its ObamaCare health benefits exchange when federal dollars run out.
That's an issue that I raised last July, in a policy brief for the RI Center for Freedom & Prosperity.
December 24, 2012
Premium Premiums? RI Employers Paying Higher Than National Average For Employee Health Coverage
Business Wire reports.
When it comes to national average costs for health plans, Rhode Island employers are paying 13 percent more for employee single coverage and six percent more for employee family coverage, according to a study by USI Insurance Services’ (“USI”).
Lovely! Another item to add to our ... er, enticing business climate.
By the way, wasn't one of the purposes of the, it turns out, remarkably expensive health insurance exchanges mandated by ObamaCare supposed to be to lower health care costs by, among other things, bringing competition to each state? Yet a recent press release from Governor Chafee's office bragging on the state's health insurance exchange omits any mention of competition. Even more interesting, the author of the Business Wire article points to this somewhat baffling statement by the state's Office of Health Insurance Commissioner.
Slade said, “The Office of the Health Insurance Commissioner for Rhode Island has stated publicly that more competition won't help solve the cost problem which we find interesting given the fact that we have less competition here than almost any other market of comparable size and possibly the absolute worst average costs.”
A couple of questions pose themselves. First of all, why is Rhode Island spending many millions of tax dollars - our federal tax dollars now, our state tax dollars later - to create a health exchange when it apparently will not, after all, bring competition into the mix?
Secondly, why did the Office of the Insurance Commissioner say what they said? Do they not want competition? Are they diminishing the importance of that element because it is now clear that the health exchange will not confer it? Or are they acknowledging that it is, in fact, the excess regulations and requirements heaped upon the insurance industry in this state by the RI General Assembly that play a large role in the higher health insurance and health care costs in the state?
I'm starting to feel that we've been snookered by the hype that preceded the health insurance exchange. It'd be nice to get some honest answers about all of this.
December 19, 2012
Things We Read Today (44), Wednesday
Government's corrupt pension handling; the discount rate scam; fighting off the zoning inspector; government peeking doesn't count as privacy invasion.
December 17, 2012
Things We Read Today (42), Weekend
The lesson of current events and history; what the 2nd Amendment means; what that means for change; government control and healthcare insecurity; government control and economic stagnation; a couple positive notes.
December 14, 2012
Gary Alexander's Long Commute and Rhode Island's Big Compensation
Rhode Island resident and former human services chief Gary Alexander has been making news back home related to his current job as Secretary of Public Welfare in Pennsylvania.
About two weeks ago, Alexander's work came up on the Current and Anchor Rising regarding a chart suggesting that a single-mother in the PA public welfare system is better off not making more than $29,000 in gross income unless she can leap above $69,000, because her loss of public assistance payments drops so much.
This week, Alexander caught the attention of Rhode Island Public Radio reporter Ian Donnis after the Pennsylvania Independent published a story about his use of a state vehicle to travel to and from his family's home in Rhode Island.
December 7, 2012
The Philosophy of Noose Tightening
Providence Journal opinion columnist M.J. Anderson offers a fascinatingly candid look at the thought processes of those whose preference for expressing concern for people is through government programs, and at how it ultimately makes a cheap trinket of freedom.
The bulk of her column describes the terrible dynamic of ObamaCare that is leading employers to shift their emphasis toward part-time workers so as to avoid the choice that the federal government has given them: pay for expensive health plans or pay a penalty. ObamaCare sets a threshold of 50 employees working 30 hours or more per week before the mandate kicks in. As with minimum-wage laws, the rest is basic math and economic incentive.
Folks who share my philosophical view of the world look at this situation and see an argument against ObamaCare.
November 27, 2012
Things We Read Today (35), Tuesday
Healthcare and what you get for free; making a living trying to fix the dying (state); the dictator prescription; and unhealthily sexist (female) teachers.
October 9, 2012
RI Governor Gives Nation a Preview of Obama’s Public Welfare Project
People across the United States should consider Rhode Island as a canary in the ObamaCare coal mine, whistling the tune of the President's larger public welfare project.
When he spoke on the first night of the Democratic National Convention, RI's Lincoln Chafee introduced himself as "the nation's only independent governor." That's "independent" as in belonging to no political party. He went on to claim the mantel of "moderate" and to upend the dictionary with a new, inverted definition of "traditional conservative," applying that label to himself, as well.
Actual moderates and conservatives should be wary of Chafee's brand of independence. The most stunning reason is his state's status, in July, as one of only three to have lost employment since the end of the U.S. jobs free fall in February 2010. A more subtle, but profound, reason is the vision of health benefit exchanges toward which he is hurrying his state.
October 4, 2012
Things We Read Today (23), Wednesday
Controlling prices across a continent; a look back at erroneous polls; Matthews in the echo chamber; excuse #2 for Benghazi.
September 25, 2012
President Obama's Early Inklings of the Dependency Portal
In the battle of hidden video and archived recordings that is sure to characterize political campaigns during the digital age, audio emerged from a 1998 presentation by then-state-senator Barack Obama at Loyola University in Illinois. The statement that made headlines (at least on the center-right side of the media) was now-President Obama's belief in economic "redistribution" through the government.
Those who've been following the development, in the Ocean State, of what the Rhode Island Center for Freedom and Prosperity is calling a "dependency portal" may be more concerned about the context. Throughout the roughly twenty minutes prior to a question-and-answer period, Obama's talk exposes early indications of precisely the model of which the Center has been warning.
September 24, 2012
Things We Read Today (18), Monday
Many faces of big government: standardized tests; interest group buy-offs; government as marketing practice; and the United States of Panem.
September 23, 2012
Things We Read Today (17), Weekend
Returning RI to its natural state; RI as a playground for the rich; the gimmick of QE; the gimmick of digital records; killing coal/economy; when "Mostly False" means true.

Unintended Consequences: Electronic Medical Records Enable "Gundecking"
Whoda thunk? (via the New York Times)
When the federal government began providing billions of dollars in incentives to push hospitals and physicians to use electronic medical and billing records, the goal was not only to improve efficiency and patient safety, but also to reduce health care costs.It's all in the number-coding apparently. And the ease with which health care providers can tag procedures or checks being performed--for good or ill. In the maritime industry that's called "gundecking".But, in reality, the move to electronic health records may be contributing to billions of dollars in higher costs for Medicare, private insurers and patients by making it easier for hospitals and physicians to bill more for their services, whether or not they provide additional care....Over all, hospitals that received government incentives to adopt electronic records showed a 47 percent rise in Medicare payments at higher levels from 2006 to 2010, the latest year for which data are available, compared with a 32 percent rise in hospitals that have not received any government incentives, according to the analysis by The Times.....
Some experts blame a substantial share of the higher payments on the increasingly widespread use of electronic health record systems. Some of these programs can automatically generate detailed patient histories, or allow doctors to cut and paste the same examination findings for multiple patients — a practice called cloning — with the click of a button or the swipe of a finger on an iPad, making it appear that the physicians conducted more thorough exams than, perhaps, they did.
Critics say the abuses are widespread. “It’s like doping and bicycling,” said Dr. Donald W. Simborg, who was the chairman of federal panels examining the potential for fraud with electronic systems. “Everybody knows it’s going on.”
[S]ome critics say an unintended consequence is the ease with which doctors and hospitals can upcode — industry parlance for seeking a higher rate of reimbursement than is justified. They say there is too little federal oversight of electronic records.... As software vendors race to sell their systems to physician groups and hospitals, many are straightforward in extolling the benefits of those systems in helping doctors increase their revenue. In an online demonstration, one vendor, Praxis EMR, promises that it “plays the level-of-service game on your behalf and beats them at their own game using their own rules.”The system helps doctors remember what they did when they successfully billed for similar patients, and ensures that they do not forget to ask important questions or to perform necessary tests, said Dr. Richard Low, chief executive of Infor-Med Corporation, which developed Praxis. “The doctor can use a chart the way the pilot uses a checklist,” he said.
But others place much of the blame on the federal government for not providing more guidance. Dr. Simborg, for one, said he helped draft regulations in 2007 that would have prevented much of the abuse that now appears to be occurring. But because the government was eager to encourage doctors and hospitals to enter the electronic era, he said, those proposals have largely been ignored.
“What’s happening is just the problem we feared,” he said.
August 27, 2012
The Environment for RI's Health Benefit Exchange & Medicaid Expansion
The RI Center for Freedom & Prosperity has been collecting reasons not to pursue a "dependency portal" unified infrastructure, marketing all government services through the health benefits exchange currently in the design phase. But there are plenty of reasons to resist the exchange and the related expansion of Medicaid eligibility without regard to the cutting edge of the entitlement state.
Both the exchange — which will subsidize health insurance for families up to 400% of the poverty level (around $90,000 for a family of four) — and the Medicaid expansion are anticipated to greatly increase access to health insurance and use of medical services. Indeed, that's the point. The problem is that the Patient Protection and Affordable Care Act (PPACA; "ObamaCare") itself does nothing to expand the supply of doctors, and Rhode Island, specifically, has taken no steps to make up for the shortcoming.
In other words, beyond the direct costs to Rhode Islanders, through state government revenue, will be a cost in the health of the local health care market. The state already suffers from high costs and burdensome state mandates. That's why some charts and graphics by Avik Roy layer in a disconcerting additional consideration.
August 21, 2012
Meanwhile, ObamaCare Penalties for Excessive Hospital Re-admissions of Seniors Quietly Kick In
Some lively back and forth with regard to the impact of ObamaCare on Medicare.
Republicans have pointed out that ObamaCare cuts $700+ billion from Medicare.
Democrats and the Obama campaign have responded variously by denying this assertion and/or saying that this amount would be found by cracking down on waste, fraud and abuse and from eliminating subsidies to insurance companies. (Sidebar: Really? $70 billion dollars per year of Medicare funds goes to these items? What happens to the availability of care to seniors when Medicare withdraws these "subsidies" from insurance companies? And if Medicare waste, fraud and abuse is such a significant amount that it can be cited as a revenue source for another program, why do we have to wait for ObamaCare to fully implement in order to crack down on it?)
But as the discussion continues, ObamaCare is already impinging upon Medicare.
In Rhode Island, nine hospitals will be penalized a total of $1.6 million in Medicare funds, for Funding Year 2013, out of about a total of $600 million in Medicare funds, according to Edward J. Quinlan, president of the Hospital Association of Rhode Island.
Why are they being penalized?
Penalties for what the federal government deems high readmissions will be no more than 1 percent in the year beginning in October, 2 percent the following year, and 3 percent the year after that, under the Affordable Care Act.Some 2,211 hospitals in the nation will lose some degree of reimbursement ...
So to reiterate. ObamaCare has ordered that hospitals be penalized Medicare funds if hospitals re-admit seniors too quickly.
Then-Speaker Nancy Pelosi said in 2010:
But we have to pass the bill so that you can find out what is in it
In addition to the $700+ billion cut from Medicare mandated by ObamaCare, Speaker Pelosi, we're now "finding out" that ObamaCare is negatively impacting Medicare in another specific way - hospital stays for seniors. If ObamaCare continues to roll out, how many other similarly questionable items will turn out to be in it?
Differences in Sources Suggest RI Does in Fact Have Most Burdensome Mandates
Admittedly, I've been griping about PolitiFact from the sidelines almost since it entered the field. For many of the uses that the reporters put it toward, the notion of entirely objective facts is as absurd as the notion of entirely objective reporters. The simplistic (albeit marketable) Truth-o-Meter emphasizes the point; something's being arguable is not the same as its being partially false.
My vantage point was backstage during production of PolitiFact RI's investigation of RI Center for Freedom & Prosperity CEO Mike Stenhouse's statement about health care mandates in Rhode Island, and I can't say I've had my concerns about fairness eased.
According to the Center's Competitiveness Report Card, Rhode Island has the greatest number of mandates in the country. In an op-ed in the Providence Journal, Stenhouse characterized it as "the most burdensome level." And PolitiFact reporter Gene Emery went on the hunt.
August 15, 2012
Example of Ryan's Acumen on Health Care - "Hiding spending does not reduce spending."
Via Andrew Malcolm at Investors Business Daily. Vice-Presidential nominee Paul Ryan directly takes on President Obama and explains how his health care reform cost more--not save--money thanks to double-counting and other gimmicks.
August 14, 2012
Ryan on Medicare
As the Wall Street Journal writes:
There's no excuse in particular for letting the White House claim that Mr. Ryan would "end Medicare as we know it" because that is demonstrably false.James Pethokoukis, working from a suggestion by the American Enterprise Institute's Andrew Biggs, lists the 3 things that need to be stated over and over about the Ryan Medicare Reform plan:Late last year, Mr. Ryan joined Oregon Democratic Senator Ron Wyden in introducing a version of his reform that explicitly retains Medicare as we know it as a continuing option. The reform difference is that seniors would for the first time also have a choice of government-funded private insurance options. The Wyden-Ryan belief is that the choices resulting from private competition will be both cheaper and better.
This "premium-support" model has a long bipartisan pedigree and was endorsed by Democratic Senators John Breaux and Bob Kerrey as part of Bill Clinton's Medicare commission in 1999. Wyden-Ryan is roughly the version of reform that Mr. Romney endorsed earlier this year.
1. No one over the age of 55 would be affected in any way.Back in 2010 President Obama called the Ryan-Wyden plan a "serious" and "legitimate" proposal (though, as Ted Nesi points out, Wyden does not agree with the latest iteration of Ryan's plan). The President also pointed out the "political vulnerability" that all such proposals have, even decrying the tendency in Washington, D.C. for one party to scare seniors, etc. instead of dealing with the proposals put forth by the other. Honest, here's the video (at around the 4 minute mark).2. Traditional Medicare fee-for-service would remain available for all. “Premium support”—that is, government funding of private insurance plans chosen by individuals—is an option for those who choose it. No senior would be forced out of the traditional Medicare program against his will.
3. Overall funding for Medicare under the Ryan-Wyden plan is scheduled to grow at the same rate as under President Obama’s proposals. Is this “gutting Medicare” and “ending Medicare as we know it”? In reality, it’s the market giving seniors cheaper, higher quality choices they can take if they wish, with the traditional program remaining an option.
At around 5 minutes in the above video, the President asks: "At what point can we have a serious conversation about Medicare and it's long term liability? Or a serious conversation about Social Security or a serious conversation about budget and debt in which we're not trying to position ourselves politically?"
Oh, I don't know, how about now?
August 8, 2012
Bringing the Dependency Portal into Focus
The RI Center for Freedom & Prosperity has posted a hub page to explain and trace the development of Rhode Island's health benefits exchange into a full fledged "dependency portal," drawing people into government programs. As much as I strove to explain the concept on that page, two of the five points that one advocacy organization lists under "modernized eligibility procedures" express the disconcerting motivations behind the effort better than I was able:
- “No wrong door” policies through which, when an application is submitted to one agency, data from the application is forwarded to other agencies to see whether consumers qualify for additional assistance—in effect, using an application for one program as an “on ramp” to other programs ...
- Default enrollment strategies that provide eligible consumers with assistance unless they affirmatively “opt out.”
July 13, 2012
Unintended Consequences: ACA's Negative Impact on Workers
Deroyal Industries is a manufacturer of a wide variety of medical devices. They have over 2000 employees in 26 states and 5 countries. According to their President/COO, both the company and its employees will be negatively impacted by the ACA's new tax on medical devices (h/t).
July 12, 2012The medical device tax constitutes the largest cost increase DeRoyal has experienced in its 40-year history. We are working to mitigate this impact in a number of ways from both a revenue and cost perspective. Even in the face of this challenge we are doing everything within our power to preserve US jobs in this incredibly difficult economic environment.
Bill Pittman, President & COO
DeRoyal
(PDF)
July 11, 2012
Costantino, Ferguson, and Roberts Describe "Unified Infrastructure"
A brief that I wrote for the RI Center for Freedom & Prosperity describing the reasons that Rhode Island should opt out of the Medicaid expansion and health benefit exchanges of the Patient Protection and Affordable Care Act (PPACA) refers to "dependency portals." That is, the exchanges will be used to draw new enrollees into other welfare programs, like food stamps and cash payments.
Here is the audio (presented as a captioned YouTube video) in which RI Health & Human Services Secretary Steven Costantino, Health Benefits Exchange Director Christine Ferguson, and Lt. Governor Elizabeth Roberts describe their first-in-the-nation intention.
Federalism and the ACA: How States Can Control Health Care Destiny
David Harsanyi explains just how expensive the "Affordable Care Act" will be:
And even after all the taxes and mandates, the CBO [Congressional Budget Office] estimates that by 2021, around 26 million Americans still won’t have health insurance. What will it cost to provide universal coverage using the Obamacare model be? We don’t know. But a person should be highly skeptical about the numbers we’re hearing.There is a way around this for states, as Jeffrey Singer of the CATO Institute explains. According to Singer, states refusing to expand their Medicaid programs will "place a huge obstacle in the path of implementing" the ACA. This is because this will shift coverage for those individuals into the Health Care exchanges that are mandated by the ACA but states aren't obligated to create on their own. And they shouldn't.In a study released a few months ago, Chuck Blahous, a Medicare Board of Trustee member named by President Obama, reported that price tag for Obamacare was around $1.15 trillion. It doesn’t lower the deficit as promised but increases it by nearly $530 billion by 2021.
A few years ago, the Senate Joint Economic Committee released a study that looked at initial estimates of programs and their costs in dollars at that time. In 1967, the House Ways and Means Committee predicted that the new Medicare program would cost $12 billion in 1990. It was $110 billion. In 1987, Congress estimated that Medicaid’s hospital subsidies were estimated to cost less than $1 billion in 1992. It was $17 billion.
That’s just two of countless examples.
So even if Obamacare’s coercive individual mandate weren’t technically a tax, it is effectively one of the largest taxes we’ve seen in a long time. And, all signs say, it’s going to get a lot bigger. In the end, someone’s got to pay.
The state reaps no advantage from creating an exchange. This is because the state must carry out all federal directives in operating and implementing the exchange, and has no autonomy in the matter. In effect, all it does is make the state act as the proxy — the executive secretary, if you will — for the federal government in operating its exchange.Therefore, states that opt-out of Medicaid expansion should also elect to not create their own Health Care Exchange, thereby shifting the burden of Exchange creation back onto the federal government.
According to the Affordable Care Act, the federal government will set up a health insurance exchange in any state that chooses not to create its own exchange. It is through these exchanges that people will obtain their government-approved health insurance....according to explicit wording in the Affordable Care Act, if the states let the federal government create the exchanges, then residents of those states will not be able to receive federal subsidies to help them purchase the super-expensive, government-designed, government-mandated health insurance. Without those subsidies, few people would want to purchase these expensive policies.Additionally:
[If the] federal government creates the exchanges, small businesses are exempt from the onerous employer mandates. This rescues small businesses from the huge financial burden Obamacare places upon them. It will enable them to expand and add jobs without fear of financial insolvency from health insurance mandates.In short, if the states don’t create their own exchanges, Obamacare won’t work.
So the cloud of the Supreme Court’s Obamacare decision indeed comes with a silver lining. It leaves the states holding all the cards. The future of Obamacare is in their hands.
Justin has also explained how the Affordable Care Act will lead to less affordable health care for Rhode Islanders and has expanded on it with a policy brief (PDF) published by the Rhode Island Center for Freedom and Prosperity, which also recommends that Rhode Island should pass a Health Care Freedom Act:
Similar actions are being taken in other states. Unfortunately, given our current governor and the political makeup of our state, there is is a snowball's chance in July of Rhode Island opting out. In fact, we're rushing to be the first in.
1) Repeal the governor’s executive order creating PPACA Health Insurance Exchanges.
2) Apply for a State Innovation Waiver to free RI from certain provisions of PPACA, including exchanges.
3) Enact a Health Care Freedom Act that would:
a) Open up competition by allowing interstate sales to permit Rhode Islanders
to purchase health insurance plans from approved providers in other states.
b) Allow an “opt out” provision from the state’s currently burdensome level of
health insurance mandates and require insurers to openly display the original
mandates not included.
4) Pass an amendment to the state constitution to prohibit the federal government from ever requiring Rhode Island residents to buy health insurance.
5) Pass a resolution calling for amendment of the federal Constitution to invalidate PPACA.
July 10, 2012
Exchanges and Medicaid Expansion Move Health Care in the Wrong Direction
The Supreme Court's recent ruling that the Patient Protection and Affordable Care Act (PPACA) is constitutional resolved one narrow area of uncertainty surrounding the law. The upcoming U.S. election season as well as the various reactions of the states to implementation of new federal policy leave the future of health care at the national level unstable.
It would be prudent for Rhode Island to consider its options as a sovereign state, rather than merely charging forward with reforms as concocted in Washington, D.C. A policy brief that I've written for the RI Center for Freedom & Prosperity finds there to be seven critical flaws — risks to Rhode Islanders — that justify reconsidering the planned implementation of the new Medicaid expansion and state health benefits exchange.
July 2, 2012
No Word on What Kind of Tax ObamaCare Is, but a Deduction?
Last week, I gave some thought to exactly what sort of new tax Supreme Court Chief Justice John Roberts had created by reading the health insurance mandate of the Patient Protection and Affordable Care Act (PPACA) as a tax. My conclusion was that the only logical reading that satisfies the constitutional restraints is that it's a capitation tax (assessed per person) for which purchasers of health insurance and those with inadequate income receive a credit on their income tax returns.
Obviously, any attempt to categorize the tax are necessarily read into the law, because there are no provisions for taxation. Indeed, the Obama administration continues to refuse to call the mandate a tax (although not simultaneously acknowledging that it must therefore be unconstitutional).
That said, presumably the country will have to move forward with this new meaning of tax, so it behooves us to determine what exactly it is. In doing so, the old rule of thumb for science fiction stories comes to mind: The author can ask readers to suspend disbelief on a few major points (e.g., the reality of magic), but the imagined universe otherwise has to operate by pretty the same rules of physics as our real one and to be logically coherent.
National Review Senior Editor Ramesh Ponnuru's solution, offered on Bloomberg View, is a bit simpler than mine: He characterizes the mandate as a tax deduction. Although he stresses that the Justice Roberts's argument is not persuasive, whatever the case, Ponnuru's deduction example isn't really applicable for a few reasons.
June 29, 2012
Lt. Gov’s Press Conference: Personal Responsibility and Free Markets
At yesterday's press conference, featuring Lieutenant Governor Elizabeth Roberts, RI Secretary of Health and Human Services Stephen Costantino, and new health exchange Director Christine Ferguson, I asked about the uninsured Rhode Islanders expected to find coverage with the implementation of the Patient Protection and Affordable Care Act (PPACA).
How many of the 120,000 new recipients would really just be young adults who've heretofore determined that they don't really need coverage? My premise is that such people don't necessarily overlap extensively with the population that uses expensive emergency room services as a primary care vehicle.
The answers were interesting, especially for anybody who is striving to assess the likely next steps of health care policy development. Costantino seemed at least partially to affirm my premise: "You have some young people who are working for a small business that don't have health insurance; they haven't really utilized the system. But it's scary."
It's a Tax on Your Body
Unless I missed some language, the Supreme Court's ruling on ObamaCare shirks the responsibility of explicitly defining exactly what sort of tax Congress has imposed and how similar taxes might be structured in the future. Still, a thread can be followed.
Having just read through the tax-related sections of the ruling, and although the logic is as incoherent and slave to convenience as any I've ever read, it seems to me that a straightforward conclusion can be drawn.
First, on the incoherence: The health insurance mandate is apparently not a tax for determining the standing of the suit, but it is a tax to save the law. It's not a capitation tax — "a tax that everyone must pay simply for existing" — for the purpose of evading the constitutional requirement that such taxes be apportioned by state, but it's like a capitation tax for the purpose of evading precedent that prevents taxation from being used as stealth regulation. Bob and weave; whatever form it has to take to pass each obstacle.
However, in writing his opinion, Supreme Court Chief Justice John Roberts makes a big deal about the fact that people with no income tax burden do not have to pay the tax: "It does not apply to individuals who do not pay federal income taxes because their household income is less than the filing threshold in the Internal Revenue Code." Later, he likens it to a tax incentive.
The only way all of this makes coherent sense (which may be too high a standard for the highest court, granted) is if one takes the ruling a step farther to determine what sort of tax it is. I'd propose that the ObamaCare tax is effectively a capitation tax or a property tax on one's body.
Discussing Health Care on Rhode Island Public Radio
Within an hour of the Supreme Court's decision on the Patient Protection and Affordable Care Act (PPACA), I was privileged to be on Rhode Island Public Radio's Political Roundtable. For about ten minutes, Ian Donnis, Scott MacKay, Maureen Moakley, and I batted around health care, politics, and our state.
David Brooks Doing the David Brooks Thing
There are aspects of this David Brooks column in the New York Times with which I'd very much like to agree. (I'm much more inclined toward moderation than folks 'round here seem to perceive me to be, except naturally those farther to the right.) But a couple examples of... what? wishful thinking? the sloppiness that obsessive moderation begets?... demand highlighting.
Take, for prime example, Brooks's phrasing of a popular statement voiced around the center-right Internet throughout the day:
Roberts and six colleagues also restrained the power of the federal government to sanction the states. And, perhaps most important, he restrained future Congressional power.
The Supreme Court did no such thing. It drew a line for use of the Commerce Clause to expand federal power well beyond where it actually ought to be, and then it opened up a whole new vista of possibilities in the form of creeping taxation. What is the ObamaCare tax? Is it a "sin tax," as with cigarettes, to be levied against bad behavior?
Is it some new double-negative tax, levied on activities that Americans cannot not do? Or is it some sort of inverted sales or excise tax on that which is not purchased? (In which case, it would seem that the Constitution must allow us to evade the tax if we explicitly choose not to purchase insurance from companies that don't sell it in our own states.)
June 28, 2012
Supreme Court Rules Individual Mandate Survives as a Tax
Chief Justice Roberts wrote the opinion. Upholds Individual Mandate as a tax under Congress' taxing powers. Apparently a complicated opinion. Others are more equipped (and have the time) to analyze, but feel free to comment!
ADDENDUM (snarky version): Roberts joined with the courts liberals, so it was 5-4. Not quite the 5-4 decision anyone anticipated, to be sure. What are liberal supporters of the Health Care act going to say about Roberts now? Does this mean the Supreme Court is all-of-a-sudden legit again?
ADDENDUM (serious version): Some are arguing that by upholding the mandate by calling it a tax while expressly ruling that it's NOT legit under the Commerce Clause, CJ Roberts has managed to give liberals a political win while also pushing back against big government overreach, which is something conservatives like. Jay Cost:
First, the Roberts Court put real limits on what the government can and cannot do. For starters, it restricted the limits of the Commerce Clause, which does not give the government the power to create activity for the purpose of regulating it. This is a huge victory for those of us who believe that the Constitution is a document which offers a limited grant of power.Second, the Roberts Court also threw out a portion of the Medicaid expansion. States have the option of withdrawing from the program without risk of losing their funds. This is another major victory for conservatives who cherish our system of dual sovereignty. This was also a big policy win for conservatives; the Medicaid expansion was a major way the Democrats hid the true cost of the bill, by shifting costs to the states, but they no longer can do this.
Politically, Obama will probably get a short-term boost from this, as the media will not be able to read between the lines and will declare him the winner. But the victory will be short-lived. The Democrats were at pains not to call this a tax because it is inherently regressive: the wealthy overwhelmingly have health insurance so have no fear of the mandate. But now that it is legally a tax, Republicans can and will declare that Obama has slapped the single biggest tax on the middle class in history, after promising not to do that.
UPDATE: Key components of Roberts writing on the SCOTUS ruling (PDF) upholding individual mandate (after the jump):
March 21, 2012
Re: He Walked the Walk
Doctor-assisted suicide isn't an issue that I've spent much time with. From where I sit, right now, suffering from nothing more burdensome than a week-long sore throat brought on (I'd guess) by the change in the weather and post-nasal drip, I'd be extremely hesitant to tell somebody with excruciating pain that they must endure it.
However, commenting to Patrick's recent post on the issue, Jon raises the worthwhile point that "death with dignity" becomes quite a bit more insidious when healthcare moves into the hands of a government necessarily keeping an eye on top-down control of costs. Insurance companies can serve the same ends, by increasing the incentive to end life rather than to manage disease.
Even beyond that concern, though, there is the broader problem that these sorts of policies tend to expand once the culture accepts them. The barriers keeping the practice rare and targeted to extreme cases tend to erode, and cultural ideas about life tend to shift.
It's all well and good to make broad pronouncements about averting suffering and to assert that "a physician who does not believe in this action will not be forced to perform it" (which Patrick is surprisingly blithe in doing, given recent debates). But if our society does move in the direction of accepting the practice, it's critical that we do so with more clarity than appears common.
Even look at the statistics available in Oregon, from the page to which Patrick links. Since the practice was legalized in 1998, only 596 people have officially availed themselves of the opportunity, which is (thankfully) not a large number comparatively.
However, only 40 of them were "referred for psychiatric evaluation." The median length of the patient's relationship with the prescribing physician was 12 weeks (that's 84 days or roughly three months). That means that for every patient who'd been seeing the prescribing doctor for their entire lives (maxing out at 1,905 weeks), there was one who'd known him or her for less than 12. The median length of time between the first request for medication and death was 46 days, or almost seven weeks.
Now, of course, it's possible that family physicians might be squeamish about killing long-term patients, or that their moral objections led their patients to other doctors. But such are the numbers that ought to constitute the core of any real debate about the issue, especially given the fact that only 6.7% of them appear to have gone through even a pro forma psychiatric evaluation.
Of far more concern, however, is the fact that only 134 of the patients cited "inadequate pain control or concern about it." Be sure, advocates, that you have a clear definition of what you consider to be suffering. Most of the patients cited "losing autonomy" and "less able to engage in activities making life enjoyable." A couple hundred less cited "loss of dignity" and "losing control of bodily functions."
If this is a path that people want our society go down, we have to take profuse care to ensure that "death with dignity" doesn't morph into plain ol' suicide, and from there, to a cost saving measure toward which the healthcare infrastructure (however it finally develops) creates incentive.
March 16, 2012

He Walked the Walk
In my usual perusing various news sources for anything interesting, I fell upon this article about a doctor in Oregon. He was someone who campaigned for and helped to get a Death with Dignity law passed in his state. Then last week, he used that law for his own benefit, at the age of 83 after suffering through a disease similar to Parkinson's.
I've never really understood why we treat our pets with more compassion than we do our family and ourselves. Any time we have a pet that is near death, or in pain or suffering due to an incurable illness, we do what we feel is right and euthanize the animal. However, many don't feel like we deserve that right for ourselves. The opposition will argue that
the proposal would promote suicide among the mentally ill or even wrongdoing by doctors and unscrupulous relatives.That just seems shortsighted to me. It takes more than a family member or a wayward doctor to make these decisions. There's only one thing that any of us truly owns in this world that that is our own lives. However, do we really own it when the only options for taking one's own life are either gruesome or painful? If someone has an untreatable disease that simply leads to suffering and a painful end, why not let the person bypass that part?
Lastly, does something being illegal mean that something isn't going to happen? Of course not.
Goodwin pointed out that the acts he sought to legalize were going on quietly between doctors and terminally ill patients anyway. The proposed law, he said, restricted the right to rational people who were at the ends of their lives and repeatedly requested their physicians' help to end their suffering.Legalizing this will remove some burden and fear from physicians. Just like anything else, a physician who does not believe in this action will not be forced to perform it. Instead it merely allows those who do agree with it to help. If anybody deserves help, it should be those who are suffering.
March 5, 2012
Thought Much About Dying?
Have you thought much about your final days, final minutes or even thereafter? I, probably like most other people have already attended more wakes and funerals than I'd ever want to. But as the great philosopher Yogi Berra said, "You should always go to other peoples' funerals or else they won't go to yours." Then again, I'm pretty sure that I don't even want anything like that. Thousands of dollars on a casket? For what? A nice box and pillows for a bag of bones? Thousands of dollars on flowers and a funeral home and all the trappings. C'mon, what a waste. Let's put that money to much better use, spend it on the living.
There's a similar sentiment to end of life health care. I recently stumbled across an article in the Wall Street Journal about how physicians die differently. Ironically enough, it's not that doctors get better end of life care, they actually often opt for less.
Years ago, Charlie, a highly respected orthopedist and a mentor of mine, found a lump in his stomach. It was diagnosed as pancreatic cancer by one of the best surgeons in the country, who had developed a procedure that could triple a patient's five-year-survival odds—from 5% to 15%—albeit with a poor quality of life.I'm not going to say I would make the same choice as Charlie. That's an extremely difficult choice to make and maybe it depends on where you are in life. Maybe that extra couple months means getting to see a first grandchild. It could mean any number of things. However, how often do we see people hooked up to machines and tubes and all the latest and greatest inventions in the world of medicine to keep someone "alive"? Is this really how we picture our last days? Hooked up to breathing and feeding tubes in a hospital room? I'm guessing most people hope or expect to just drift off to sleep one night and peacefully continue on. Unfortunately, it rarely happens that way. Quite often, it's our own fault.Charlie, 68 years old, was uninterested. He went home the next day, closed his practice and never set foot in a hospital again. He focused on spending time with his family. Several months later, he died at home. He got no chemotherapy, radiation or surgical treatment. Medicare didn't spend much on him.
Have you spoken to your spouse or other family members about what you want to be done for you? Have you given someone else (or multiple people) the ability and right to make these decisions for you if you're unable? It's always best to make these decisions when you're clear-headed and not stressed. I have one such example.
I was very close with my own grandmother. She was getting into her 80s and had failing health. She had a number of issues going on, not the least of which was untreatable leukemia. Similar to Charlie described above. She worked her career as a nurse and has seen that quite often "the cure is worse than the cause" and decided she'd just ride it out. She also decided to keep that condition from our family for most of the rest of her life.
One day, she called and asked me to go to the doctor's office with her where she needed me to sign some paperwork. She wanted me to be second in charge (after my mother) in making end of life decisions for her. She finally explained her condition, along with her physician, and said she didn't want any more life saving procedures. She signed the "Do Not Resuscitate" orders. She even half-jokingly threatened to haunt me from the afterlife if I let her die after being hooked up to machines for weeks for months. I believed her. I accepted my responsibility, signed the paperwork and kept a copy.
Less than a week later, with my mother out of state, I got a phone call at 6:30 am from my grandmother that she wasn't feeling very well at all and was going to the hospital. She asked me to meet her there. This one sounded different, she sounded worse than normal. Just in case, I brought all the paperwork with me and I got there a few minutes after 7. As soon as I got to the ER and explained why I was there, the nurse said my grandmother was being prepped for surgery. I immediately got to her room where a surgeon was just wheeling her out to the operating room and explained to me that she had massive bleeding on her brain from the leukemia and needed emergency surgery now to relieve the pressure. With surgery, she might survive but without it she definitely would not.
I handed the paperwork to the surgeon, he read it, asked if I was sure, I said yes, and that was it. A few hours later, she was gone. About the only positive thing, or at least the only reassuring thing that happened all day was that her original physician, the one I'd met with less than a week before stopped in to see my grandmother and me. He offered his condolences and just looked at me and said, "You did absolutely the correct thing."
There was no extended suffering, there were no heroic measures, there was no stringing it out artificially. Her time had come and she made her choice, I was merely the spokesperson for her.
So take a read through the linked article, give it some thought, and help the people who will be put in the same spot. Let them know what decision you want to make, so they will not have to decide, in a stressful and emotional situation. Give them the reassurance that they too are making the right decision.
Addendum: If you'd like to read more about this need for decision making, Jessica David (@JDinRI) sent this additional article along: http://hbr.org/2012/01/tackling-social-problems/ar/1
February 13, 2012
Rahe: Catholic Church Reaping What it Helped Sow
With the ongoing controversy between the Obama Administration and religious institutions--particularly the Catholic Church--as to whether the health care plans offered by the institutions should cover items they deem inconsistent with their religious tenets (ie; contraception, etc.), Paul Rahe writes that the support given to various progressive causes by the institution of the Catholic Church, in particular, has come back to bite them. He provides some history:
In the 1930s, the majority of the bishops, priests, and nuns sold their souls to the devil, and they did so with the best of intentions. In their concern for the suffering of those out of work and destitute, they wholeheartedly embraced the New Deal. They gloried in the fact that Franklin Delano Roosevelt made Frances Perkins – a devout Anglo-Catholic laywoman who belonged to the Episcopalian Church but retreated on occasion to a Catholic convent – Secretary of Labor and the first member of her sex to be awarded a cabinet post. And they welcomed Social Security – which was her handiwork. They did not stop to ponder whether public provision in this regard would subvert the moral principle that children are responsible for the well-being of their parents. They did not stop to consider whether this measure would reduce the incentives for procreation and nourish the temptation to think of sexual intercourse as an indoor sport. They did not stop to think.He also offers anecdotal evidence:In the process, the leaders of the American Catholic Church fell prey to a conceit that had long before ensnared a great many mainstream Protestants in the United States – the notion that public provision is somehow akin to charity – and so they fostered state paternalism and undermined what they professed to teach: that charity is an individual responsibility and that it is appropriate that the laity join together under the leadership of the Church to alleviate the suffering of the poor. In its place, they helped establish the Machiavellian principle that underpins modern liberalism – the notion that it is our Christian duty to confiscate other people’s money and redistribute it.
At every turn in American politics since that time, you will find the hierarchy assisting the Democratic Party and promoting the growth of the administrative entitlements state. At no point have its members evidenced any concern for sustaining limited government and protecting the rights of individuals. It did not cross the minds of these prelates that the liberty of conscience which they had grown to cherish is part of a larger package – that the paternalistic state, which recognizes no legitimate limits on its power and scope, that they had embraced would someday turn on the Church and seek to dictate whom it chose to teach its doctrines and how, more generally, it would conduct its affairs.
I would submit that the bishops, nuns, and priests now screaming bloody murder have gotten what they asked for. The weapon that Barack Obama has directed at the Church was fashioned to a considerable degree by Catholic churchmen. They welcomed Obamacare. They encouraged Senators and Congressmen who professed to be Catholics to vote for it. {Emphasis added.}
I was reared a Catholic, wandered out of the Church, and stumbled back in more than thirteen years ago. I have been a regular attendee at mass since that time. I travel a great deal and frequently find myself in a diocese not my own. In these years, I have heard sermons articulating the case against abortion thrice – once in Louisiana at a mass said by the retired Archbishop there; once at the cathedral in Tulsa, Oklahoma; and two weeks ago in our parish in Hillsdale, Michigan. The truth is that the priests in the United States are far more likely to push the “social justice” agenda of the Church from the pulpit than to instruct the faithful in the evils of abortion.Rahe goes into much greater depth than these snippets indicate and it's worth a read (whether you tend to agree or disagree).And there is more. I have not once in those years heard the argument against contraception articulated from the pulpit, and I have not once heard the argument for chastity articulated. In the face of the sexual revolution, the bishops priests, and nuns of the American Church have by and large fallen silent. In effect, they have abandoned the moral teaching of the Roman Catholic Church in order to articulate a defense of the administrative entitlements state and its progressive expansion.
February 10, 2012
Memo to Bishops: Don't Fall For It
The Washington Post has collected a spectrum of religious reactions to the Obama administration's "compromise" — apparently announced as such without first consulting with the parties implicitly involved in the negotiations (a sure sign that Obama is more concerned about appearing to compromise than actually doing so). Religious leaders and others concerned about religious liberty — in particular those concerned about our ability to work through cultural avenues distinct from government to help shape society — should pause in their deliberations about the specifics of this overture.
Note what position the President's games put us in: We're not arguing about the morality of contraception (including abortifacients). We're not even arguing about the legitimacy of the government's declaration that everybody should have access to them free of cost (at least free of immediate cost to them). We're merely arguing about who else must pay — who has to chip in for the pills that address pregnancy as an illness to be treated and against which to be inoculated.
One hopes that the administration's initial overreach was enough to awaken the bishops and others to the reality that a deal with the Devil is always, always conditional on his ability to force you to the next-least-moral space on the playing field.
December 6, 2011
Government Sets a Thief to Catch... a Business
Yes, the story isn't as simple as a gut reaction allows, but broken down into a summary, this story feels like a cautionary tale of the leviathan state:
David Whitaker's cooperation with the Google investigation was called extraordinary several times during his sentencing [for Internet fraud crimes] in U.S. District Court in Providence. Assistant U.S. Attorney Andrew Reich said that because of the probe, millions of Americans have been protected from rogue online Canadian pharmacies advertising prescription drugs through Google's AdWords program. ...After his arrest, Whitaker disclosed to investigators that he had been selling prescription drugs online in Mexico with the help of Google's AdWords program, Reich said. Whitaker described how he developed relationships with Google employees who allowed him to place ads for drugs obtained from overseas without a prescription, Reich said.
Whitaker helped investigators construct phony websites that purported to sell the drugs, officials said. Then, an undercover investigator would tell Google employees who were creating the advertising for the products that they were manufactured overseas and did not require customers to have a valid prescription, officials said.
Ailing people seek legal drugs sold in Canada because U.S. government regulations (among other things) drive up the cost in their own country. Canadian pharmacies advertise on the World Wide Web, and American customers follow those links and purchase their products. So, the U.S. government enlists a criminal to help set up essentially a scam designed to relieve Google of $500 million. (Funny how, in the context of government spending, that hardly seems like a significant amount of money.)
Somehow, I can't help but think of some of our government's other activities that have been in the news lately, such as this one (although, at least in this case, the targets are criminal organizations selling drugs that are illegal with or without prescription):
Fast and Furious was a Bureau of Alcohol, Tobacco, Firearms and Explosives program, overseen by the Justice Department, which facilitated the sale of thousands of weapons, via straw purchasers, to Mexican drug cartels. Straw purchasers are people who can legally purchase guns in the United States but do so with the intention of illegally trafficking them into Mexico.At least 300 Mexicans were killed with Fast and Furious weapons, as was U.S. Border Patrol agent Brian Terry. Gosar said Holder bears responsibility for the operation. Holder is expected to face another round of questions about the scandal on Thursday when he appears before the full House oversight committee.
And that stops short of consideration of state involvement with the gambling industry...
December 1, 2011
The Hidden Power Grab
So, the Obama administration has given Rhode Island another $58 million to work on its government-run healthcare exchange, along with compliments for being so resourceful as to skip the legislative process in its implementation. At this point, the federal government shuffling around money that it doesn't have is hardly news, nor is the Obama administration's affection for imposing policies on the electorate. The real news, in my view, comes in the third-to-last paragraph of the Providence Journal story:
Additionally, it [the exchange] will decide how many plans will be included, and how they will be designed
Presumably, reporter Felice Freyer doesn't mean that the exchange will be an entity with artificial intelligence, so the decisions will actually be made by the really smart people (like Lincoln Chafee and Elizabeth Roberts) whom we elect to office, and their appointees. As I've noted before, the exchanges are just a sly way to impose government-run healthcare without elected officials' ever having to tell the American people explicitly that they're doing so. Create an exchange that enables regulation to the point of minute control, and then draw people toward its offerings.
One can hope that the world of the future will be such that the history books make note of the shadowy organization that used foreign money borrowed on future generations' backs to build a trap designed to give it minute control over the life decisions of a supposedly free people.
November 2, 2011
To Hell With "Government Experts" 2: Keep Covering Your Ass
Almost exactly two years ago, I wrote a post titled "To Hell With 'Government Experts', Keep Feeling Your Boobies" in which I explained my disagreement--admittedly in a gut-level sense--with new guidelines pushing breast cancer screenings for women out a decade further (from 40 years old to 50). I ended by warning, "And men, don't take this sitting down. Your ass (colonoscopy guidelines) could be next."
I was right: now the same agency, the U.S. Preventive Services Task Force, has issued guidelines stating we may be over-doing the PSA screening test.
The truth is, after reading the reasoning behind the decision, I can see the cost/benefit analysis that has gone into the decision (here is a decent point/counterpoint on it). Basically, many of those who have screened positive are either "false" positives or their cancer was so slow growing it wouldn't be (to put it bluntly) their ultimate cause of death. So many men go through the treatment to "cure" them of something that just may not actually kill them. Similar arguments were made regarding the breast cancer screenings. Of course, this is all based on averages, not actual lives. Sucks to be an outlier!
Guidelines serve a purpose, but it still boils down to a personal decision. However, as Glenn Reynolds noted, "when [you] politicize health care, the suspicion is that all health care decisions are political." Especially when it seems decisions are being made based on a cost/benefit analysis model that defines cost in dollars, not lives.
October 11, 2011
An Inapplicable Model
Honestly, something about Governor Chafee's fact-finding missions makes me very nervous. Consider this, from his latest trip, to Pittsburgh. It focuses on the University of Pittsburgh Medical Center (UPMC), which is attracting all sorts of federal money and expanding the prominence of the University's medical program:
Dr. Edward Wing, now dean of medicine and biological sciences at Brown's Alpert Medical School, worked 23 years at the University of Pittsburgh. He notes that the western Pennsylvania medical school — with massive collaboration, clinical-research dollars and consolidation — has since catapulted from the middle of the pack to among the nation's top-tier medical schools.UPMC is now a $9-billion global health enterprise that operates more than 20 hospitals and 400 outpatient sites; employs more than 2,800 physicians and 54,000 employees; ranks as western Pennsylvania’s largest employer and the state’s second-largest. ...
In the midst of the tour, Wing noted, "It's very hierarchical, so they can make decisions easy. It's much harder in Providence." ...
At UPMC, it's clear that money drives activity.
So, you've got a massive, hierarchical structure fueled with giant infusions of public money and absolutely central to the local economy. That sounds extremely risky, and while I don't know enough about Pennsylvania politics to know how they're handling it, out there, I simply wouldn't trust the power brokers of Rhode Island with such an entity.
And that's if the feat would be possible to reproduce. One need only look at a map to see one way in which Pittsburgh differs tremendously from Providence: There's no urban competition in proximity. We've got Boston and New York City within easy striking distance.
The governor should turn his sights away from top-down behemoths and look toward making Rhode Island notable, in the crowded Northeast, for being an easy and inexpensive place to start and grow business. Our economic development people look to UPMC and see the flow of money that they could use to get entrepreneurs and innovators over the hump of high expenses and difficulty, in RI, when they should be looking to flatten it, instead.
September 22, 2011
"Exchange" as in Bait and Switch
When I initially heard of the concept of state-government healthcare exchanges, my first thought was that only three insurers are willing to do business in Rhode Island — how extensive could such an exchange be? The hook by which Governor Chafee is presuming to step in and legislate via executive order to create Rhode Island's exchange raises more questions about what, exactly, they're planning to develop:
The state faces a Sept. 30 deadline to apply for tens of millions in federal money to develop the exchange, but needed to first establish the authority to create, govern and finance the exchange.
The model cited for the exchange is Travelocity and other comparison-shopping sites, but with three insurers to review, how could it possibly take "tens of millions" in (borrowed) federal dollars to put such a thing together? The state ought to be able to get somebody to pull together the necessary documents and deploy a slightly tweaked out-of-the-box search engine for under $100,000.
Apart from finding ways to spend taxpayer money that the state and federal governments do not have, Lt. Gov. Elizabeth Roberts gives some indication of what the expanded scope of the exchange might be:
... Roberts said the exchange will provide more active assistance to people choosing health insurance. It may also set standards for the types of health insurance products offered.Indeed, the executive order also explicitly calls for "payment reforms and innovative benefit designs" that promote quality and efficiency.
"One of the goals of this executive order is to create the infrastructure with some early goals," Roberts said. "A lot of those bigger issues are very appropriately going to be discussed by the board going forward."
As I've speculated before, the "exchange" is more of a bait-and-switch. As Roberts describes it, the site will either be a welfare-style means of drawing people toward taxpayer-subsidized programs, or it will grant a small range of technocrats the ability to shape everybody's healthcare programs in very detailed ways, or both. And a look at the board already in place to guide the thing is not encouraging:
In addition to [former U.S. Attorney Margaret] Curran, the chairwoman, the board's public members will include Vice Chairman Donald Nokes, president and co-founder of the small business NetCenergy; Michael C. Gerhardt, a former health insurance executive; James Grace, president and CEO, InsureMyTrip.com; Linda Katz, policy director and co-founder, The Poverty Institute; Peter Lee, president and CEO, John Hope Settlement House; Dr. Pamela McKnight (not currently practicing); Tim Melia, UFCW New England Council; and Minerva Quiroz, case manager, AIDS Project RI.The government members are: Steven M. Costantino, secretary of Health and Human services; Christopher F. Koller, health insurance commissioner; Richard A Licht, director of administration; and Dr. Michael D. Fine, director of health.
In addition to the government bureaucrats, we've got a former lawyer, a former health insurance executive, a former doctor, two executives from businesses that offer related technology services, three paid activists, and the obligatory union representative. Not present is a single person who looks apt to approach this sly government power-grab from the perspective of Rhode Islanders' civil rights (in the government-limiting sense) or of protecting the free market or taxpayers' wallets. There isn't even anybody whose background suggests an especial concern with the ethical questions that inevitably arise in matters of medicine.
A further frightening thing is that the only organized voice that the reporter finds in opposition is Barth Bracy, of the Rhode Island Right to Life Committee. About the only other opposition that I've seen has come from Mike Stenhouse, CEO of the newly formed Rhode Island Center for Freedom and Prosperity, in an op-ed arguing that the state should be wary of jumping into ObamaCare because many questions remain — not the least being whether the law will even remain in effect. For the most part, that's a statement of process, not of principle, although he does step beyond the practical argument a bit:
Government does poorly vs. the free market. The very idea of a government-controlled exchange is antithetical to our nation's historical free-market principles, which is the only proven way to consistently deliver a good service at the lowest possible rate. A true free-market is an exchange in itself!
Unfortunately, politicians (especially in Rhode Island) have long thought the handling of healthcare to be too important to leave to people who actually know what they're doing. Their exchanges will not be tools to guide consumers to the products that most closely align with their needs and resources, but to tell taxpayers how much they have to spend on healthcare, for what, and for whom.
September 7, 2011
Healthcare Exchange More than Commonly Thought
As I explained in a video blog a couple of years ago, Tiverton resident, one-payer healthcare advocate, and just-about-overt socialist Nick Tsiongas is an instructive figure to watch in Rhode Island politics, and the op-ed that ran in yesterday's Providence Journal is a fine example.
I'm thinking that many of us have underestimated the intended reach of the state-level healthcare exchanges that will be implemented as part of ObamaCare:
Any reform with a chance of success would require that we move as much of the money as possible into one place and coordinate its use with a state health plan. The power of the plan and the purse would let us use carrots and effective sticks to change this crazy system.Such an opportunity exists: It’s the exchange, a marketplace set up by the state under the Affordable Care Act where people and businesses could buy health insurance. We have the chance to build an exchange where all Rhode Islanders can buy public or private insurance.
If your view of the healthcare exchange has been as a sort of benign, non-binding Web site on which to compare possible plans in a straightforward manner, you (like me) forgot that everything that government does is not about serving the public, but about government power. In Tsiongas's telling, the exchange is an opportunity to filter all of our healthcare dollars through a single point, at which the government can impose requirements that force users of health services to conform with best practices as defined by Nick Tsiongas and friends.
By opening the exchange to all our residents and linking it to an explicit state health plan, we can finally empower ourselves to get off the cost treadmill, maintain quality and start treating this ailing system.
He doesn't go into how, exactly, the exchange will be "linked" to "an explicit state health plan." On one end (no doubt his ideal), all companies allowed to sell healthcare plans would have to do so through the exchange, and the exchange would require them all to conform with government-defined benefits, creating a de facto single plan over which bureaucrats, ideologues, and special interests have government access.
On the mild end, a state plan would compete with other plans which may or may not have to be on the exchange or meet additional requirements than they currently face. If that's the case, then it's hard to see how a state plan could be so attractive as to draw people away from other options unless it exacerbates cost problems by subsidizing member benefits through additional revenue confiscated from taxpayers.
Either way, the exchanges cannot be written off as a mild distraction for unnecessary government functionaries if the likes of Tsiongas have such strong intentions for them.
September 1, 2011
Not Getting to Keep the Coverage That You Like
It's too bad nobody was able to see this as a probably consequence of ObamaCare:
Nearly one of every 10 midsized or big employers expects to stop offering health coverage to workers after insurance exchanges begin operating in 2014 as part of President Barack Obama's health care overhaul, according to a survey by a major benefits consultant.Towers Watson also found in its July survey that another one in five companies are unsure about what they will do after 2014. Another big benefits consultant, Mercer, found in a June survey of large and smaller employers that 8 percent are either "likely" or "very likely" to end health benefits after the exchanges start.
If this outcome weren't so unexpected, one might be tempted to wonder whether President Obama's assurances that anybody who likes his or her health coverage could keep it was deliberately deceptive.
Seems to me that I haven't been hearing near enough from elected officials about repealing the healthcare legislation, lately.
August 10, 2011
Moving the Goal Posts on Healthcare
See, I don't recall this being the sales point with which President Obama and his allies pushed ObamaCare:
New projections show that health care spending will grow faster than the nation's GDP over the next decade. But the increase will be only slightly more than would be the case without the new national health law.At least that's what the White House and other health law supporters drew from a new analysis of actuarial data released by the U.S. Centers for Medicare and Medicaid Services. The analysis, published in Health Affairs last week, reported that health spending through 2020 would rise only one-tenth of one percent more under the health law than it would have otherwise — despite some 30 million more people getting health coverage.
Sure, a bunch of young, healthy people will now have insurance that they wouldn't otherwise have purchased without incurring Earth-shaking costs, but ObamaCare wasn't sold on the great deal that it would provide in covering additional recipients. It was going to slow the inflation of health care costs. Indeed, it was going to be a sort of deficit reduction program for the government. That's clearly not expected, now, and wasn't expected by many of us who opposed the legislation in the first place:
Over the next 10 years, federal actuaries expect the pace to pick up. By 2020, the national bill will be $4.6 trillion — one in every five dollars spent in the U.S. economy. The government's share also will rise. Washington will pay 30 percent of the tab, and state and local governments will pay almost 20 percent. Average annual spending growth over the decade will be 5.8 percent, according to the analysis.
Our broke and flailing government is currently covering about 27% of $2.7 trillion in healthcare spending, or $729 billion. In 2020, that federal expenditure will be $1.38 trillion, with state and local governments paying another $92 billion. (The article doesn't say what the lower-tier governments currently pay.)
Repeal this monstrosity.
June 10, 2011
Massachusetts and Connecticut More Generous with Medicaid than RI
Apparently RI legislators haven't gotten updated or correct numbers when it comes to the income limits for offering RIte Care (Medicaid* in RI).
The information, presented at a public hearing on Monday, portrayed Rhode Island as more generous in its RIte Care benefits than either of its neighboring states, Connecticut and Massachusetts, citing information from the Rhode Island Public Expenditure Council, “How Rhode Island Compares.” Rhode Island was said to allow parents to enroll at 175 percent of the poverty level, compared with 150 percent for Connecticut and 133 percent for Massachusetts.This was important because the House is looking at making the eligibility requirements for receiving RIte Care tougher by dropping it to 133% of the poverty level. The apparent error was brought up by Mark Reynolds of the Neighborhood Health Plan of Rhode Island.
The problem, according to Reynolds, is that the figures being used were not accurate. In Massachusetts, eligibility extends to 300 percent of the federal poverty level, and the 133 percent figure is when cost-sharing premiums kick in for the participants. In Connecticut, eligibility extends to 185 percent. (See chart.)Here's a chart that helps explain the differences. I can't track down the RIPEC report, but comparing states' eligibility isn't always apples to apples because they differ in when benefits kick in. This seems to be the case with comparing RI to Massachusetts. As for Connecticut, I wonder if RIPEC's numbers were "accurate at the time" but CT has since changed? Regardless, the important take away is that "both Massachusetts and Connecticut cover parents at higher incomes than Rhode Island does today." I'm good with that.“From what we are hearing, there is a misperception by some in the Legislature that eligibility requirements for RIte Care are more generous than those of our bordering states,” said Reynolds. In fact, both Massachusetts and Connecticut cover parents at higher incomes than Rhode Island does today.”
*Thanks to brassband for the correction.
June 7, 2011
"If You Like Your Insurance, You Can Keep It."
Remember when the President of the United States repeated that promise over and over to the American people? Well quite a few of us less-lofty folks predicted this contrary outcome:
Once provisions of the Affordable Care Act start to kick in during 2014, at least three of every 10 employers will probably stop offering health coverage, a survey released Monday shows.
But that's not all:
The survey of 1,300 employers says those who are keenly aware of the health-reform measure probably are more likely to consider an alternative to employer-sponsored plans, with 50% to 60% in this group expected to make a change. It also found that for some, it makes more sense to switch.
In some cases, the lost benefit might transition to some other form of compensation (although many of us have also predicted that ObamaCare will not stop, and may accelerate, cost inflation and quality deflation in the medical industry). In the push for government control of healthcare, though, spanning its peculiar procedural maneuvers and bold flight in the face of taxpayer concerns, likely outcomes were downplayed, not thoroughly vetted.
May 23, 2011
Pension Pinch is Bad...so is Healthcare
WPRI's indefatigable investigative team has turned up the fact that RI cities and towns owe a combined $3.6 billion in healthcare benefits (Sen. Dennis Algiere wrote about this a few days ago). From the WPRI report:
The state's municipalities have promised to provide nearly $3.6 billion worth of medical coverage to their current and future retirees over the next three decades, but government financial reports show they've put aside almost nothing to pay the bill – just $27.5 million, or less than 1 percent of the future cost.WPRI has provided a map for you to check out your city or town's liability. You won't find any info for Hopkinton, Exeter and Richmond: they never promised health care coverage (golf clap). There are predictable and common sense solutions outlined in the piece. Be sure that all will be resisted.To put it in perspective, the $3.6 billion unfunded liability for city and town retiree health care is significantly larger than their pension plans' shortfall of roughly $2.2 billion.
As with pensions, communities do not need to come up with the money for these so-called "other post-employment benefits," or OPEB, all at once. But most have barely begun to grapple with the cost.
"You've heard the general treasurer recently say pension reform for state employees and municipal employees isn't a problem – it's the problem," said Dan Beardsley, executive director of the Rhode Island League of Cities and Towns. "Well, I would say OPEB obligations and dealing with those obligations is either equal to or just a notch down from the needed pension reform."
May 21, 2011
Waivering Health Care Reform
About his then residence that had undergone extensive renovations, Dave Barry once observed,
When prospective buyers ask: ''What kind of construction is this house?" I answer: "Spackle."
Similarly, health care reform now seems to be comprised largely of waivers. 204 more companies were granted waivers in the last ten days, 20% of them going to companies located in the district of former (ahh!) House Speaker Nancy Pelosi. The total number of purportedly temporary (but how easy will it be to grant one year extensions ... year after year after year) waivers issued now tops 1,700.
Just as notable as those issued to companies in CA-8 is the waiver that recently went to everyone's (???) favorite senior advocacy organization. Ed Morrissey at HotAir explains the significance, not to say irony.
No one seems to know what criteria HHS uses to grant or deny waivers to insurers from provisions in ObamaCare. The White House won’t release the names of those insurers and employers refused waivers or discuss denials at all. But maybe, just maybe, we could all agree that organizations that publicly pushed ObamaCare to approval should be ineligible to escape its consequences?
Indeed, why would the AARP be anxious to duck out of a law for which they themselves advocated?
ADDENDUM
Anthony correctly reminds us that entire STATES - Maine, New Hampshire and, most recently, Nevada - have obtained waivers from ObamaCare.
Forty seven more to go!
May 20, 2011
Coffee News to Wake Up To
Early morning seemed the appropriate time to mention this news report:
Drinking coffee, regular or decaffeinated, may reduce the risk of prostate cancer, according to a study by Harvard University researchers.The study found that men who consumed six or more cups of coffee a day had a 60 percent lower risk of developing deadly metastatic prostate cancer and a 20 percent reduced risk of developing any form of the disease. One to three cups cut the risk of lethal prostate cancer by 30 percent. The findings, published today in the Journal of the National Cancer Institute, suggest non-caffeine elements in coffee may provide the benefit.
Yeah, the researchers stress that there are harmful effects to coffee, as well, and encourage readers not to conclude that they should increase their intake of the beverage. Still, I'll take it as reason to pep up a little before having my regular daily doses.
April 27, 2011
Democrats in Massachusetts Take Health Care Out of Collective Bargaining
Reality has hit Massachusetts' Democratic politicians, from the Governor on down: they realize the state can no longer afford to negotiate fixed medical co-pays in government employee contracts that span multiple years while the actual costs quickly increase well past the negotiated level.
House lawmakers voted overwhelmingly last night to strip police officers, teachers, and other municipal employees of most of their rights to bargain over health care, saying the change would save millions of dollars for financially strapped cities and towns.Democratic leaders claim this allows them to put more money directly towards services and retaining or hiring personnel.The 111-to-42 vote followed tougher measures to broadly eliminate collective bargaining rights for public employees in Ohio, Wisconsin, and other states. But unlike those efforts, the push in Massachusetts was led by Democrats who have traditionally stood with labor to oppose any reduction in workers’ rights.
“What we've recognized is that unfortunately, because of the cost of health insurance, that a very large percentage of the monies we commit are unfortunately going to fund municipal health insurance,” said House Ways and Means Chair Brian Dempsey (D-Haverhill). “Now, that’s not anyone’s fault. We’re not blaming anyone for the rise in health insurance. But, it's a fact. It’s a fact. The cost of health insurance is going up, and the money we commit every year, it’s unfortunately not going to textbooks. It’s not going to classroom size. Unfortunately, it’s going to a large degree to fund municipal health insurance.”Notice that this was done at the state level. In Rhode Island, individual cities and towns have proposed--or may try--similar reforms. Doing it at the state level would save a lot of time. Everyone is in the same boat, after all.“I applaud the members of the House for taking the vote that will save more than $100 million for cities and towns,” [Massachusetts House Speaker Robert] DeLeo said in a statement. “By spending less on the healthcare costs of municipal employees, our cities and towns will be able to retain jobs and allot [sic] more funding to necessary services like education and public safety.”
March 9, 2011
Health Care: Yes, we have no bananas
It's up to over 1,000 entities that have acquired a waiver from adhering to President Obama's national health care law. One is the entire State of Maine, whose motto, Dirigo or "I lead," could be prophetic as other states look to do the same.
Meanwhile, the unintended, but predicted, consequences (h/t) of this hurried health care reform are coming to fruition.
Patients are demanding doctors' orders for over-the-counter products because of a provision in the health-care overhaul that slipped past nearly everyone's radar. It says people who want a tax break to buy such items with what's known as flexible-spending accounts need to get a prescription first.Read the whole thing for more, just on that issue. Aside from that, there are other things:The result is that Americans are visiting their doctors before making a trip to the drugstore, hoping their physician will help them out by writing the prescription. The new requirements create not only an added burden for doctors, but also new complications for retailers and pharmacies.
"It drives up the cost of health care as opposed to reducing it," says Dr. Chung, who rejected much of a 10-item request from a mother of four that included pain relievers and children's cold medicine....Some doctors, irked by the paperwork and worried about lawsuits, are balking at writing the new prescriptions. Pharmacists and retailers say the changes mean they have to apply a personalized label on some 15,000 different everyday products for customers paying with certain debit cards.
Health-policy experts predicted that new insurance pools for high-risk patients would attract so many expensive enrollees that funding would be quickly exhausted. In fact, enrollment is running at just 6% of expectations, partly because of high premiums.It's amazing that this could have happened, isn't it?A provision preventing insurers from denying coverage to children with pre-existing health conditions prompted insurers in dozens of states to stop selling child-only policies altogether.
And a piece of the law designed to centralize patient care by encouraging health-care providers to collaborate is running into antitrust concerns from regulators.
February 28, 2011
Observed from Within the Complications
The complaints against high-deductible health insurance coupled with health savings accounts presented in Richard Salit's article, yesterday, seem more like groans against change than anything:
... some health experts say that you can't expect people who are ill to be cost-conscious consumers — even healthy people have difficulty price-shopping for medical services. That's why Christopher Koller, the state's health insurance commissioner, says the plans are no "silver bullet" for curbing the nation's health-care costs. ...Higher-deductible plans can be challenging to understand. They include a new vocabulary of terms and quite a few acronyms to decipher. They also require people to get involved in managing their health-care expenses in a way they never have before.
The Coastal Medical group has witnessed first-hand how some patients get confused by the plans.
Sure, high-deductible plans are more confusing than top-of-the-line offerings that allow consumers to go anywhere at any time, but those are increasingly rare. In general, health insurance has hardly been a simple matter. Referrals, primary care, copays, coshares... most people, I'd hazard to suggest, already tend to go where they're advised to go and pay whatever bill is sent their way once the insurer has trimmed it down.
The only added complication, with high-deductible plans, is that the bills don't get trimmed until the plan member has paid a certain amount. When coupled with health savings accounts, that money just comes from them, first. Frankly, the notion that people are too ignorant to comprehend this added step is suspiciously patrician.
Koller does raise the reasonable concern that bills that patients find unpayable end up stuck on hospitals' and doctors' books. Similarly, employer Donald Nokes, who recently switched his company to a higher-deductible plan, observes that employees who had health issues during the year weren't as happy with the change as those who did not. Of course, they're likely happier than they would have been if the company had not been able to afford any benefit at all.
What unites Koller's and Nokes's points is that they are indications that the price-conscious reform of high-deductible plans and health savings accounts is still beginning. As such an approach becomes more common, more people will have years of healthy buildup in their savings accounts to absorb the pain of tougher years. When that's the case, fewer health care providers will find their invoices unpaid.
Above everything, though, what gets lost in the article is the comparison of doing nothing. Moreover, any reform that attempts to avoid the necessity of patients' involvement in their own care will fail to control costs, unless it puts decisions in the hands of supposed experts with the power to deny care.
We have no choice, that is, but to choose the path of education and individual investment.
February 16, 2011
Health Care "Reform" = IRS Expansion
U.S. News tells us that the IRS is ramping up because of the new health care reform plan (we're all so surprised!):
The Internal Revenue Service says it will need an battalion of 1,054 new auditors and staffers and new facilities at a cost to taxpayers of more than $359 million in fiscal 2012 just to watch over the initial implementation of President Obama's healthcare reforms.'Ware the Tanning Taxers!!!
Among the new corps will be 81 workers assigned to make sure tanning salons pay a new 10 percent excise tax. Their cost: $11.5 million....[They] will be tasked just to handle the tax reporting of 25,000 tanning salons. They face a new 10 percent excise tax on indoor tanning services. Another 76 will be assigned to make sure businesses engaged in making and import[ing] drugs pay their new fee which is expected to deliver $2.8 billion to the Treasury in 2012 and 2013. The new healthcare corps will also require new facilities and computers.Phew, glad this is making things all so much easier. Just kidding (obviously)....But don't forget, according to the ProJo, this complication is all because of conservatives playing with the tax code.
February 3, 2011
The Obamacare Waiver List Grows
Melissa Clouthier called attention to this from Ethel Fenig at the American Thinker:
In August, 2009, as he was extolling the virtues of his proposed Obamacare, President Barack Obama (D) famously promised "If you like your health care plan, you can keep your health care plan." And if you're a union member you certainly can; if you're not, well...Hey, why not? They've got good plans. John Sexton explains why they're "waivering" (ba-dump bump):The Health and Human Services site Helping Americans Keep the Coverage They Have and Promoting Transparency (sic) conveniently lists the 773 waivers approved to date. Scroll through the list; notice that most of the waivers, more than 650 went to unions exempting well over 2 million employees.
This ever-expanding list of waivers is the direct result of ObamaCare raising the annual benefit caps on certain health plans. Obviously, a plan with higher annual limits is potentially more costly than one without them. The money to cover the difference in premiums has to come from somewhere. Without the waivers, it will come from the employer who are forced by law to upgrade to the more expensive plan. In other words, the...organizations who have received waivers are not seeking refuge from an unintended consequence, but from the costs associated with one of ObamaCare’s features.Obviously, it's not just unions that received waivers as there are many, many small businesses that have them, too. As Sexton also asks, "...what [will] these businesses...do once the waiver program comes to an end?"
February 2, 2011
Seems Folks Argued This All Along...
This point was made so early in debate over the federal healthcare overhaul — before the Democrats rammed it into law despite every negative signal from the American people — that it's difficult to believe that anybody still believes the opposite. Still, it's worth noting its restatement:
Two of the central promises of President Barack Obama's health care overhaul law are unlikely to be fulfilled, Medicare's independent economic expert told Congress on Wednesday.The landmark legislation probably won't hold costs down, and it won't let everybody keep their current health insurance if they like it, Chief Actuary Richard Foster told the House Budget Committee. His office is responsible for independent long-range cost estimates.
Legislators cannot simply ignore the law of supply and demand, no matter how much the resulting policies may please the special interests to which they cater or how much more invasive authority over citizens the legislation grants them.
February 1, 2011
Marriage as Healthcare Policy
Pankaj Ahire, of Charlestown, uses extremely condemnatory language, laying the potential death of his same-sex partner at the foot of RI Roman Catholic Bishop Thomas Tobin:
The lack of marriage equality implies that my excellent health and dental insurance does not cover my partner. Unfortunately, my partner has had health issues, and could not go to a doctor. To see him suffer when I could have provided for him is agonizing to say the least.But more importantly if tomorrow something happens to my partner, you can bet that I will take him straight to emergency room. Who foots the bill now? The State of Rhode Island. In this economic climate, shouldn't taxpayers try to get coverage for as many people as possible? Marriage equality is a way to do that.
Ahire provides an excellent example of the error in progressive thinking that has wrought so much damage throughout the United States and Western society at least since the mid-1800s. Radically altering cultural institutions in order to serve immediate economic and personal desires and needs — no matter how just and urgent they may be — ignores the pillars that have evolved over centuries and that such institutions developed to support.
Marriage is fundamentally about joining of the two halves of human biology, man and woman, most significantly in the bodies of the children that only a man and a woman can create. The ability to extend employment benefits to a loved one is not its key quality, neither is tax policy, neither is a government stamp of equality, and behaving as if any of these ancillary aspects should be focal points undermines an institution that is in dire need of fortification, in our time.
Mr. Ahire would be more rational to direct his ire at those who've held up healthcare reform. He'd be more intelligent to advocate for reforms that lower the cost thereof and increase freedom and choice when it comes to insurance plans and means of acquiring medical services.
January 19, 2011
Health Care Wrangling
The U.S. House of Representatives will most likely try to repeal the Obama Health care program this week, though that's where the effort will stop because of the political realities (Democrats control the Senate) while on another front, we are now up to 26 states that are suing the Federal Government over the imposition of the Obama program.
Advocates explained to the ProJo why repeal isn't a good idea, basing their argument on the benefits accrued by filtering your tax dollars up through the beltway bureaucracy and back down to the state level so that several programs can be implemented by local bureaucrats to help manage the plethora of benefits forthcoming from the aforementioned feds. Promise!
Meanwhile, the impact of the health care reform so far has resulted in a winnowing of "choice." Some examples, as explained by Sally Pipes: 1) the construction of at least 45 physician-owned hospitals has been halted because they didn't open in time to qualify for Medicare certification; 2) doctors are planning on dropping patient care or limiting the amount of patients they treat who are Medicare/Medicaid because they can't afford to treat them; 3) Rules requiring small plans to spend 80% of premiums on medical claims will push many out of existence (those efficiencies are tough to reach in smaller plans--economies of scale, etc.). So smaller plans that may be able to compete against the giants in certain sectors will be pushed out.
Then Pipes explains the impact of the new over-the-counter drug restrictions, which--I can tell you--has been much discussed at my workplace and home:
Other measures kicking in are petty -- but punitive. For example, people can no longer use tax-free Health Savings Accounts on basic over-the-counter drugs. Instead, they must pay for a doctor's appointment -- and then get a prescription for a pricier pharmacist-dispensed drug.Pipes exaggerates a bit--for my plan, a doctor's note explaining that an OTC drug is called for is adequate justification to be able to use an HSA to pay for it--but that still requires a doctor visit. Just more hassle, more red-tape and more bureaucracy all to make things...better?Consider the case of Claritin, an allergy medication that recently was approved for OTC use. A report from the National Center for Policy Analysis found that longtime users of the drug saw their daily costs fall 80 percent, from about $2.50 to just 50 cents. ObamaCare reverses this trend by encouraging people to opt for higher-priced prescription drugs when a cheaper OTC medication would work just as well.
January 8, 2011
The Predicament of Dementia
Father Tadeusz Pacholczyk notes an unfortunate, but natural, reaction to dementia. Relating the story of a woman who could only connect with her afflicted mother by singing hymns, with the lesson being that "there's always someone in there," Pacholczyk goes on to lament our tendency to behave as if that's not the case:
Sometimes we may view the situation more from our own vantage point, rather than the patient's. In a report on care for the elderly, physicians Bernard Lo and Laurie Dornbrand put it this way: "Family members and health professionals sometimes project their own feelings onto the patient. Life situations that would be intolerable to young healthy people may be [made] acceptable to older debilitated patients."[Steven] Sabat notes how this raises the prospect of reducing the patient to a kind of object:
The dementia sufferer is not treated as a person; that is, as one who is an autonomous center of life. Instead, he or she is treated in some respects as a lump of dead matter, to be measured, pushed around, manipulated, drained, filled, dumped, etc.
Two thoughts: First, it's possible to see a debilitating mental illness of late-life as a means of easing the process of death's separation. To the loved one, the circumstances of the patient appear intolerable — perhaps more so than death itself — but if treated properly, the sufferer may not have to see the circumstance as one of suffering. In that way, the gradual loss of a connection to reality makes the final separation bearable.
Second, the particular affliction of dementia relates intriguingly to a metaphysical interpretation that I've come to see as broadly explanatory. Basically, we are all instantiations of the idea of us in every circumstance in which it would be logical for us to appear, given the constraints of physics and history; that is, if it were logically possible for you to be a millionaire movie star at this moment in time, an instance of you exists in that very role.
Our individual awareness of continuous time (another way of saying "our souls") moves from one instance to the next with each passing moment, but according to the rules of reality. Your soul can't, in other words, instantly leap into the version of you that's a movie star, but you could take the steps — educational, social, economic — that lead you closer. This isn't just a linear progression in a unique, circumscribed reality; it's a transition of the very state of your being.
The experience of mental disorders, therefore, would be movement from one step to another with no logical coherence. To those of us living in a more ordered sequence of reality, that incoherence seems unreal.
So, it would be more correct, by this model, to say that the demented person is "over there," rather than "in there" (lateral, rather than buried) although it remains no less possible to draw them back, perhaps so strongly and sustainedly as to effect what appears to be a miracle overcoming of biological logic.
January 3, 2011
Almost Like Another Ponzi Scheme
This doesn't appear to be a sustainable system:
Consider an average-wage, two-earner couple together earning $89,000 a year. Upon retiring in 2011, they would have paid $114,000 in Medicare payroll taxes during their careers.But they can expect to receive medical services - from prescriptions to hospital care - worth $355,000, or about three times what they put in.
As each generation shrinks in size from the previous, the number of payers decreases, and as medical science and individual longevity advance, the pay outs increase. That's why folks my age don't really expect to see a penny of such "entitlements."
January 2, 2011
So Rep Lally Favors an Increase in Health Insurance Premiums for Rhode Island?
On Thursday, the Providence Journal printed an OpEd by Dr. Joseph Cambio of Urologic Specialists of New England and RI House Deputy Majority Whip Donald J. Lally (D, Narragansett & South Kingstown). We'll stipulate for a moment the problem that they name because it sounds all too plausible.
... Rhode Island health insurers reimburse the state’s physicians at a very low rate. This is a particular problem with such medical specialties as urology. Urology is only one of many medical fields, as well as dentistry, from which we are losing our best and brightest to other states. We also have aging field of doctors. As older physicians in our state retire there are fewer and fewer newer doctors to take their place. The reason is quite simple: Why would a new physician with over $150,000.00 in debt from medical school loans set up a practice in the state if he or she could make significantly more money by going to Massachusetts, Connecticut or somewhere else?It is becoming increasingly difficult to recruit new physicians to Rhode Island. Urologic Specialists of New England had one promising young doctor recently turn down its offer when he saw that he would make significantly more for the same practice in Massachusetts.
So let's agree, in the absence of new and contradictory information, that pay for doctors practicing in Rhode Island needs to be increased. Now the question is, where does that additional money come from? Who pays for the increase?
Apologies for answering a question with a question. But maybe I'm missing something.
Within the insurance framework, is there any source for higher compensation - i.e., an increase in spending - other than rate payers?
December 13, 2010
Federal Judge: Obamacare "Individual Mandate" = Unconstitutional
A Federal Judge in Virginia has ruled that the individual mandate portion of President Obama's health care reform law is unconstitutional. From a note on page 36 of the decision:
If allowed to stand as a tax, the Minimum Essential Coverage Provision would be the only tax in U.S. history to be levied directly on individuals for their failure to affirmatively engage in activity mandated by the government not specifically delineated in the Constitution.The judge also expects his decision to be appealed to the U.S. Supreme Court. The White House has acknowledged that the individual mandate is "not severable" from the rest of the law. In short, without the individual mandate, the health care law as it is constituted can't work.
December 11, 2010
An Insidious Mindset
So, the Providence Journal editorial board likes ObamaCare. What are you gonna do? A recent unsigned editorial, though, points toward a disturbing underlying premise:
Let us start with one of the provisions most beefed about on the campaign trail but also most necessary — the requirement that everyone buy coverage. Forcing people to obtain insurance is essential for two reasons: One is that it ensures a larger insurance pool to cover the expenses of sick people. Does this mean that the healthy must subsidize the ill? Yes, but that’s how insurance works.
This, in a phrase, is socialized medicine, and there's no difference between this sort of involuntary insurance and compulsory redistribution of resources. Indeed, what redistributive scheme would not be possible to present in terms of "insurance"?
Relatedly, note this double misconception:
Perhaps the most important place to trim waste is in the unhealthy economic incentives that nudge doctors to prescribe more treatments and office visits than are necessary. This is also the hardest to fix, because it means narrowing or shutting down some income streams in a health-care industry that has virtually bought many members of Congress.The Medicare program and private insurers are the ultimate payers and therefore perfectly placed to move health care away from the wasteful fee-for-service model and toward a results-oriented one.
First of all, Medicare bureaucrats and insurance providers are not the "ultimate payers." They are middle-men between the people you pay for healthcare and people who deliver it. The ultimate payers are policy holders and taxpayers. They are perfectly positioned to trim waste from the system by deciding whether they're willing to pay for it.
That suggestion leads to the second of all: It is hardly obvious that the players in the healthcare industry who neither receive the care nor deliver it have any incentive to lower costs in a way that maintains services. Their incentive is to extract more money from the payers and procure lower prices from the providers. Take more money from the payers, and they're going to seek more services to make the higher price worthwhile; give less money to the providers, and they're going to seek ways to tack more services on to their bills.
December 2, 2010
A Foreseeable Consequence for Health Insurance Consumers
Remember when those of us who opposed ObamaCare were insisting that the law would increase costs and result in fewer options and others, including members of the Service Employees International Union were getting downright violent in support of the law? We were right, and they were working to their own detriment:
Late last month, the Service Employees International Union informed dues-paying members of its behemoth 1199 affiliate in New York that it was dropping its health care coverage for children. That's right. A radical leftist union, not an evil Republican corporation, is abandoning the young ‘uns to cut costs.More than 30,000 low-wage families will be affected, according to The Wall Street Journal. Who's to blame? SEIU 1199 benefits manager Mitra Behroozi singled out oppressive new state and federal regulations, including the much-ballyhooed Obamacare rule forcing insurers to cover dependents well into their 20s.
Megan McArdle layers on some context, but this response to a perfectly foreseeable consequence of legislation that the union itself was prominent in promoting does have relate interestingly to the exemptions and waivers that we keep hearing about.
November 27, 2010
What Healthcare Poll Results Really Show
The Providence Journal's headline: "Public split on health-care law." The source, McClatchy Newspapers, states the implication more boldly: "New poll undercuts GOP claims of a midterm mandate."
A majority of Americans want the Congress to keep the new health care law or actually expand it, despite Republican claims that they have a mandate from the people to kill it, according to a new McClatchy-Marist poll.The post-election survey showed that 51 percent of registered voters want to keep the law or change it to do more, while 44 percent want to change it to do less or repeal it altogether. ...
On the side favoring it, 16 percent of registered voters want to let it stand as is.
Another 35 percent want to change it to do more.
On their face, though, the available answers to the question of "what Congress should do with the 2010 Health Care Law" are confusing. The first evidence that this is a factor comes later in the article:
Independents, who swung to the Republicans in the Nov. 2 elections, are evenly divided on how to handle the health care law, with 36 percent for repealing it and 12 percent for restraining it — a total of 48 percent negative — while 34 percent want to expand it and 14 percent want to leave it as is — also totaling 48 percent.
McClatchy's summary of these results isn't anywhere near plausible. According to the analysis, folks who responded to Obama and the Democrats by switching to Republicans are more likely than the average to "favor" the healthcare law, as defined as "wanting to change it to do more." Looking at the raw data (PDF), more Tea Party supporters want to "change it so it does more" than "change it so it does less." The question is clearly ambiguous. What if I want healthcare laws to allow more high-deductible plans with health savings accounts? Or to enable individual purchase of health insurance across state lines? Or to reform tort law? On the scoreboard, those policies are on the opposite end of the spectrum from ObamaCare, yet some poll respondents almost certainly were thinking of such things when they said they want the law to "do more."
To bolster its analysis, McClatchy considered responses to individual components of the law. Respondents liked the facts that it "stops insurance companies from denying coverage because of pre-existing conditions" (59% to 36%), "allows children up to age 26 to stay on their parents' health insurance policies" (68% to 29%), and "closes the so-called donut hole in Medicare prescription drug coverage by providing assistance to pay for costs" (57% to 32%). But respondents flip their opinions on the signature aspect of the law that defines ObamaCare. Only 29% think "Americans should be required to buy health insurance," while 65% believe "it is unconstitutional to require it." (Note that the poll is sloppy even at this level of detail: Why must the choices be support for the insurance mandate or unconstitutionality? Surely it's possible to think it's constitutional but still oppose it.)
Clearly a case can be made that:
- A more choice-driven health insurance regime would enable Americans to choose policies that suit them (e.g., covering adult children).
- Less-expensive high-deductible and catastrophic coverage plans with health savings accounts would be more broadly affordable and, therefore, translate into fewer Americans caught with "pre-existing" conditions, because they wouldn't be without insurance for periods of time or lose it when they switch employers.
- All of the benefits that Americans wish to derive from healthcare law can (perhaps must) be sought only after all of the obscure and detrimental aspects of ObamaCare have been stricken wholesale from the legal code.
October 19, 2010

Intro: Federal Judge Rules that the Attorney Generals' Suit Against the Federal Healthcare Law can Continue. What Do the Candidates for RI AG Think About This?
Last Thursday, Judge Roger Vinson of the Federal District Court of Northern Florida ruled that the lawsuit challenging the new Federal healthcare law filed by 20 state Attorney Generals should be allowed to continue. His reasoning is very straightforward. The Federal Government’s power to act is limited by the Constitution...
My review of the statute is not to question or second guess the wisdom, motives, or methods of Congress. I am only charged with deciding if the Act is Constitutional. If it is, the legislation must be upheld --- even if it is a bad law...Conversely, if it is unconstitutional, the legislation must be struck down --- even if it is a good law....and since a Federal imposition of a purchase mandate on individuals is an unprecedented extension of Federal power, the question of whether that extension is Constitutional merits consideration...
At this stage in the litigation, this is not even a close call...The power that the individual mandate seeks to harness is simply without prior precedent.Prior to Judge Vinson’s ruling, all of the candidates for Rhode Island Attorney General had previously taken positions on whether a challenge to the healthcare law had any legal merit. I asked each candidate what impact a Federal Judge's decision that “it’s not even close” had on their positions. Responses received so far will be posted on the upcoming half-hours...
October 11, 2010
Healthcare "Huh" for Today
The article's a couple of weeks old, but it's still worth noting a bit of writing that I don't think Projo journalist Felice Freyer or her editors would have allowed into print if they weren't fundamentally in favor of government healthcare:
The increases will pay for the coverage of dependents through age 26 and preventive services that now must be provided without any cost to the consumer.
Yup. The extra money you'll be paying for insurance is intended to make sure that you don't have to pay for certain services. Makes sense...
Of course, there may be a correlation-is-not-causation effect, here. Perhaps an habitual tendency to believe that something is free as long as its cost is filtered through a few steps of disguise results in a preference for government solutions.
September 25, 2010
Congressional Timidity on ObamaCare - Or - We Certainly Won't Remind You What We Did
Further to Justin's post, ABC's The Note is hard pressed to find any congressperson expending precious campaign dollars to broadcast their "Yea" vote for ObamaCare.
Six months after President Obama signed a sweeping health care measure into law, how many Democrats nation-wide are running TV ads touting their votes for the law?Answer: Zero
Caveat: We have trolled through ads ourselves and checked with Republicans and Democrats who would know. So its possible there is some innocuous ad out there. But it would be the exception that proves the rule.
A survey two weeks ago by Jennifer Haberkorn at Politico came to the same conclusion.
Many congresspeople voted for Obamacare. They must have thought it was a good thing. So why the scarcity of tv ads bragging about that vote? Why the reluctance to run on their own voting record on this matter?
September 24, 2010
Reminders of What They Did
The Washington Examiner offers a useful reminder of some of the actions of ObamaCare:
Six months ago, President Obama, Senate Majority Leader Harry Reid and House Speaker Nancy Pelosi rammed Obamacare down the throats of an unwilling American public. Half a year removed from the unprecedented legislative chicanery and backroom dealing that characterized the bill's passage, we know much more about the bill than we did then.
Costs will go up; abortions will be funded; consumers will lose the coverage that they like; doctors will be harmed, economically; jobs will be lost; the government will grow and become more invasive. The slight correction may be necessary that a lot of us "knew" these things about the bill inasmuch as we expected them to be included.
September 17, 2010
Government Drives Us Crazy
My first thought, upon reading about Butler Hospital's attempts to gain government approval for a 26-bed addition for psychiatric patients was, "Must everything be a controversy?" Unfortunately, the more government involves itself in every corner of American society, the more the answer becomes, "yes."
Psychiatric hospitals around the country have also been expanding, and about a dozen new psychiatric hospitals have been built in the past few years, said Mark Covall, president and CEO, of the National Association of Psychiatric Health Systems, in Washington, D.C.This is in reaction to a decline in psychiatric beds during the previous decade, the closing of state mental hospitals, and today’s surging demand as insurance coverage improves and the stigma of mental illness eases, Covall said.
The improvement of insurance coverage can be substantially explained, one supposes, by the government parity mandates spearheaded by our own Rep. Patrick Kennedy. And when people feel like they are either getting something for free or paying for it regardless of usage, they'll tend to use it more, eliminating price mechanisms as a fulcrum for supply and demand. What people are willing to pay for becomes moot to the extent that government requires that they (or others) provide financing.
Naturally, it therefore falls to government to regulate usage — whether through quotas, rationing, or the allocation of funds for supply. Thus, when a provider, like Butler Hospital, perceives a shift in demand and seeks to adjust accordingly, competitors, like Rhode Island and Miriam hospitals, and organizations that handle the money, like Blue Cross & Blue Shield, have the opportunity to stop it from doing so through public hearings. The determination, ultimately, is made by unelected bureaucrats, in this case, in the state Health Department, tasked with oversight of the entire system.
Such judges will perforce be drawn from within the industry and, however much they proclaim a narrow focus on the public interest, will be most approached, wheedled, and manipulated by large, powerful entities. Which entity wins, ultimately, is only incidentally related to the well-being of one-voice-one-vote citizens who live and die by the ability to acquire that which they need.
September 14, 2010
Maybe I'm Too Cynical, But...
Did you happen to catch this article by Felice Freyer?
Do you want a governor who will embrace the law and make the most of it? Independent Lincoln D. Chafee, Democrat Frank T. Caprio and Moderate Party candidate Kenneth J. Block all accept the law — with varying degrees of enthusiasm — and all pledge to carry it out fully.Do you want a governor who will resist the law, perhaps join other states in challenging it in court, and take a minimalist approach to its requirements? Either of the Republican candidates would probably satisfy you on that score. John F. Robitaille and Victor G. Moffitt both say they believe the law is unconstitutional.
Do you want a governor who will enter office with a deep understanding of the health-care system and the nuances of the federal overhaul? You're out of luck.
Two points follow from the above. First, developing a nuanced understanding of ObamaCare hasn't been necessary, because opinions are generally formed, and the issue has been defined by the side that believes the whole "reform" ought to be scrapped on both pragmatic and principled grounds.
Second, ObamaCare defined the current Congress and administration — and set the tone for this election season — in terms of the fact that voters who wanted elected officials who would develop an understanding of "the nuances of the federal overhaul" before making it the law of the land were out of luck.
August 13, 2010
You Scam, They Scam
I've been holding on to this link because a couple of questions continue to nag at me:
Authorities said busts carried out this week in Miami, New York City, Detroit, Houston and Baton Rouge, La., were the largest Medicare fraud takedown in history -- part of a massive overhaul in the way federal officials are preventing and prosecuting the crimes.In all, 94 people -- including several doctors and nurses -- were charged Friday in scams totaling $251 million. Federal authorities, while touting the operation, cautioned the cases represent only a fraction of the estimated $60 billion to $90 billion in Medicare fraud absorbed by taxpayers each year.
First, did it really require "a massive overhaul" in order to define, discover, and prosecute outright fraud? And if new regulation of some sort was needed, couldn't that have been passed quickly and easily through Congress when the problem was first discovered? Which leads to:
Second, couldn't the savings and recovered money (if any) go toward making Medicare self-sustaining, rather than helping to balance out a costly new entitlement program?
August 10, 2010
The ObamaCare Scam
The healthcare legislation should never have become law, and as time goes on, we continue to discover what a shoddy bit of law-making it was:
Talk about a paperwork nightmare: Tucked into the massive new health care law is a demand that nearly 40 million U.S. businesses file tax forms for every vendor that sells them more than $600 in goods. ...The goal of the provision was to prevent vendors from underreporting their income to the Internal Revenue Service. The government must think those vendors are omitting a lot because the filing requirement is estimated to bring in $19 billion over the next decade. ...
Republicans want to repeal the filing requirement and pay for it by changing other parts of the new health care law, a strategy that Democratic leaders won't support. Democrats want to repeal the filing requirement and pay for it by raising taxes on international corporations and limiting taxpayers' ability to use special trusts to avoid gifts taxes. Republicans won't support that.
Because of the method of the legislation's enactment, nobody caught this problem before it passed, and those who were aware of it were either too ignorant to foresee (or object to) the consequences or thought it would offer a nifty trick for repealing the problem and increasing taxes after the legislation had squeaked through to passage. Frankly, the whole bill is a scam and an atrocity and should be repealed in full.
Barring that, the Republicans are exactly right: repairs to the law should be made within the law.
August 1, 2010
Different Escalators to and from Sanity
Did you happen to catch this in the New York Times, last week?
Even as the new coalition government [of Great Britain] said it would make enormous cuts in the public sector, it initially promised to leave health care alone. But in one of its most surprising moves so far, it has done the opposite, proposing what would be the most radical reorganization of the National Health Service, as the system is called, since its inception in 1948.Practical details of the plan are still sketchy. But its aim is clear: to shift control of England's $160 billion annual health budget from a centralized bureaucracy to doctors at the local level. Under the plan, $100 billion to $125 billion a year would be meted out to general practitioners, who would use the money to buy services from hospitals and other health care providers.
The plan would also shrink the bureaucratic apparatus, in keeping with the government’s goal to effect $30 billion in “efficiency savings” in the health budget by 2014 and to reduce administrative costs by 45 percent. Tens of thousands of jobs would be lost because layers of bureaucracy would be abolished.
Yes, the move is to doctors, but more importantly, it's toward patients. In other words, the much lauded National Health Service is decentralizing, even as the ruling class of the United States attempts to push our system in the other direction.
Note, also, the underlying justification for government bureaucracy: the employment of government bureaucrats! One wonders what is given up in the private sector in order for paper pushers to survive on plush government compensation.
July 17, 2010
Rationing Life
I'd forgotten it during the national debate about universal healthcare, but in processing old columns for my personal site, I came across this, from May 2005:
Intrinsic human worth may not dominate the scales during other lifecycle stages for long, either. One indication of the slide is the British judiciary's hearing arguments concerning a problem that arises from government-funded healthcare: deciding whether the patient or the doctor/public has the final say on when to cease care.As the lawyer representing the General Medical Council stated, "a doctor should never be required to provide a particular form of treatment to a patient which he does not consider clinically appropriate." Instead, in a "joint decision-making" process, the doctor should provide a menu of "appropriate" courses of action from which the patient may choose. The lawyer for the National Health Service noted that the doctor should compile the list of options "having regard to the efficient allocation of resources." It may not be appropriate, in other words, for treatment to include a hospital bed and the expensive attention and technology associated with it.
When the government encourages expectations of "cradle to grave" care, the focus of major decisions shifts from humans' dealing with the contingencies of life to society's managing human beings. An ailing patient can weigh every consideration related to his or her own life and choose, or not, self-sacrifice for things that he or she values — whether personal dignity or the preservation of savings for a family's well-being. When the authority ultimately rests with the public, however, this opportunity translates into a judgment of comparative value between citizens. There is a bottom line to balance, and it helps to exclude patients who cannot move sustenance to their digestive systems, for example.
We're now on the path.
July 16, 2010
UPDATE: A Short-Lived Order Protecting Short-Lived Human Beings
Remember that executive order that supposedly gave pro-life Democrats cover to vote for Obamacare? Oh well:
[House Republican Leader John] Boehner [of Ohio] and other Republicans point to reports that the Health and Human Services Department is giving Pennsylvania $160 million to set up a new high-risk insurance pool that will cover any abortion that is legal in the state.
According to Boehner, the response of the Obama administration to inquiries has been not to respond. People may pretend otherwise, but I don't think anybody actually doubted this outcome. Hopefully, the current election cycle will prove that burying the truth in subtext will not avert consequences. Also hopefully, as I suggested this morning, a shift of power won't merely change the direction of the corruption.
On the matter of funding abortion, though, I remain concerned that recent jurisprudence out of Massachusetts, concerning same-sex marriages, there, may lead federal courts to invalidate the federal government's ability to place such strings and restrictions on the use of our money.
ADDENDUM:
After this matter began to draw attention, the Department of Health and Human Services released the following statement:
As is the case with FEHB plans currently, and with the Affordable Care Act and the President's related Executive Order more generally, in Pennsylvania and in all other states abortions will not be covered in the Pre-existing Condition Insurance Plan (PCIP) except in the cases of rape or incest, or where the life of the woman would be endangered.Our policy is the same for both state and federally-run PCIP programs. We will reiterate this policy in guidance to those running the Pre-existing Condition Insurance Plan at both the state and federal levels. The contracts to operate the Pre-existing Condition Insurance Plan include a requirement to follow all federal laws and guidance.
Note, however, that this post had to do with a high risk insurance pool, not a PCIP. Perhaps it's an unnecessary distinction, but I'll believe it when I see the subsequent release. Note, also, that pro-abortion groups appear to believe that this statement changes things.
July 6, 2010
Healthcare's Unchanged Incentives
Offering some representative anecdotes from her experience as a doctor, Alieta Eck explains the problem with the Obamacare approach to healthcare reform:
Are these patients or their physicians committing fraud? No. They are simply acting legally to enhance their own well-being, following the incentives set up by the unwieldy system. People with "coverage" do not care what costs they incur, and those who provide services benefit by providing more. As with the oil rig in the Gulf, there is a lot of pressure behind the leak. Adding more pressure — as with the Democrats' idea of saving money by covering everybody — is not the answer. It can only make things worse.
Everybody assumes that bringing healthy people into the insurance fold will help to balance increased usage among the sick, but the incentive, for them, will be the same as for everybody: Use whatever services are conceivably needed. Even if "broadening the pool" does delay the inevitable, Eck sees this as our future...
Once the nation is bankrupt, hospitals have closed, and physicians have found alternate ways to earn a living, real medical needs will not be met. The best medical care in the world will simply cease to exist. Then all Americans, young and old, will feel the pain.
... and offers an alternative approach with which Anchor Rising readers will be readily familiar:
There is a better answer, pointed out by Rep. Ron Paul, M.D. (R-TX):"We need a system in America where patients pay cash for basic services, and carry insurance only for serious illnesses and accidents. 'Health maintenance' is the responsibility of each of us individually. We cannot continue to collectivize the costs of healthcare and expect things to get better."
Insurance needs to be insurance, and consumers must be required to incorporate cost into their healthcare decisions.
July 2, 2010
Cures as the Positive Hook for Healthcare Policy
James Pinkerton offers a strategic angle for Republicans on healthcare:
Health-care spending is a problem, but it is important to remember that spending is a secondary issue. The primary issue is health itself — how to achieve it, how to maintain it, and how to regain it in the case of sickness or injury. Health-care finance is hotly contested political ground, yet Washington has had precious little to say on the subject of health in recent years.That is perplexing — and a huge missed opportunity. After all, people don't go to the doctor because they have insurance plans or health-savings accounts. They go to the doctor to get well and to stay well. Americans' eyes may glaze over at the wonky debates that are catnip to Washingtonians, but, beyond the Beltway, they can't seem to get enough information about their bones, bladders, and blood pressure. ...
Those on the right who have been fighting Obamacare have been loud and articulate in their criticism of its bureaucratic aspects, but they have had precious little to say about curing and preventing diseases. The opportunity now exists for Republicans to reassociate themselves with the creation of health. Let the Democrats own the redistribution of health-care dollars and the management of scarcity; Republicans have a chance to own the much more powerful issue of solving health problems.
Extrapolating a little bit to derive policy from Pinkerton's suggestion, free-market based reforms — real choice when it comes to the context in which health insurance is purchased, a functional system that pushes high-deductible plans back toward being actual insurance rather than an unnecessary layer for routine care, and tort reform — would jump start the healthcare industry and probably free up money for public investment in research.
It's an approach worth candidates' consideration — not to be forgotten, of course, once they claim offices.
June 23, 2010
What Healthcare Is Like
R.R. Reno makes a fair point that our pre-Obamacare healthcare system ultimately created "an ad hoc mechanism for extracting payments from the insured to finance a haphazard effort to provide at least emergency and critical care for the uninsured as well as decent care for the underinsured."
Seeing this as socialization, Reno argues that something like the individual mandate is preferable, to explicitly provide general care (cheaper than emergency) to the uninsured and those with preexisting conditions. I'm not so sure, first of all, that forcing the involvement of young adults and others who opt not to insure themselves — effectively looking to one segment of the "uninsured" to pay for another — will make for an even swap.
More to the point, though, I don't think avoiding the excesses is possible when government gets involved. We're sure to find, for example, that those young adults will be permitted onto their parents' plans at ever older ages. We're also sure to see mandatory coverage expanding, redistributing wealth from the healthy to the ill (and those who treat and advocate for the ill). Given Reno's reliance on "political realities" for his argument, that he doesn't anticipate this response and address it in greater detail suggests that some of his premises require reconsideration, such as:
Think about getting hepatitis or breast cancer. The risk of suffering from these misfortunes is similar to the risk of being mugged or shot. It's a life-and-death matter, and if human government has any justification for its power over citizens, then surely it rests in its unique capacity to pool resources to protect life. As Albert Camus recognized, one moral source for solidarity can be found in our common struggle against the dehumanizing power of suffering and untimely death.
In circumstances of interpersonal violence, government is arbitrating between people. That's not the same as arbitrating between a person and a virus or cancer. That government can exert force to stop individuals from doing the same in an acute act of assault does not mean that it's appropriate for government to step in as a life manager.
June 13, 2010
A Leaked Document Followed by a Reluctant Confirmation: Under ObamaCare, 50% or More of Americans Will Not Be Able to Keep Their Health Care Plan
Friday's Investor's Business Daily.
Internal administration documents reveal that up to 51% of employers may have to relinquish their current health care coverage because of ObamaCare.Small firms will be even likelier to lose existing plans.
The "midrange estimate is that 66% of small employer plans and 45% of large employer plans will relinquish their grandfathered status by the end of 2013," according to the document.
In the worst-case scenario, 69% of employers -- 80% of smaller firms -- would lose that status, exposing them to far more provisions under the new health law.
This contradicts the repeated reassurances made by President Obama as he was attempting to sell health care "reform":
If you like your health care plan, you can keep your health care plan.
There is one seemingly small characteristic of this document which is chilling in its long-term implication to American health care should ObamaCare remain unchanged before its implementation.
The 83-page document, a joint project of the departments of Health and Human Services, Labor and the IRS
Confirmation that the federal government is well on its way to edging market forces altogether out of the system and replacing them with the tax gun. Commenter David P correctly points to the next inevitable step, which is for government to dictate "the terms under which it provides service".
In Massachusetts, we are getting a preview of how this will unfold as government price controls combined with government mandates now begin to squeeze and then whittle down the number of health care providers willing to stay and dance to the tune of MassCare.
June 12, 2010
MassCare: Ominous Developments in the Precursor to ObamaCare
So in early April, Governor Deval Patrick's Division of Insurance rejected most of the rate increases for individual and small business plans which Mass insurers requested, marking the first time the state had flexed its authority in this way.
But, though most of us have a love/hate view of them, insurers are just the man in the middle. Note that Patrick's action in freezing premiums, which meets with the approval of the Obama admin, did nothing to address the underlying reason for cost increases. What it did do is pile ever more losses on the industry which, as it was, had entered 2010 in the red.
Sure enough, six weeks later, in mid May,
The four major Massachusetts health insurers yesterday posted first-quarter losses totaling more than $150 million, with three of them blaming the bulk of the losses on the Patrick administration’s decision to cap rate increases for individuals and small businesses.The carriers attributed $116 million of their $152 million in losses to the April 1 ruling by the state Division of Insurance to deny most proposed premium increases for the so-called small-group market.
The next step for the carriers, naturally, is to attempt to pass the losses along to providers.
Massachusetts health insurers say they want to freeze or slash payments to some hospitals and large physician groups this year, setting up the toughest contract negotiations in memory and creating the potential for disruptions in where patients get their care. ...Unlike in past years, insurers believe they have widespread backing from politicians, regulators, and employers to aggressively push back against large price increases, even if it means some unhappy providers drop out of insurers’ networks, forcing patients to find new doctors and hospitals.
Whoops. Sounds like Bay Staters may be on their way to losing their right to choose (... a doctor, anyway).
Now the latest development (h/t Michael Graham). The Patrick administration has moved to place three carriers into administrative oversight.
State officials said they sent letters to three health insurers earlier this year asking them to accept more intense oversight and supply additional data because of concerns about their financial health.One of the insurance companies has agreed to administrative oversight, while regulators are negotiating details with the other two, the officials said. Administrative oversight is a first step regulators take when they determine there is a need to monitor the financial condition of insurance carriers more closely. It does not mean the companies are insolvent.
Officials said the heightened concern is related to the fragile economy, which caused several major insurers to lose money in 2009.
Really, a fragile economy? Or something else, like a government has taken a strangle-hold on your business? Michael Graham:
Was it really the "fragile economy" that's causing Massachusetts insurance companies to go broke, as the Patrick administration claims? Or is it the lousy Romney-Care plan they’re working under, and the fact that more and more people are getting services they're not paying for? Those costs are being shifted onto taxpayers and the insurance companies.
In Massachusetts, we are getting a real life preview of what will happen when, in four years, under Congress' orders, MassCare becomes a national pandemic. It's not pleasant. Can we please observe, learn and react accordingly, even if it means a "drastic" course change (back to the status quo)?
June 2, 2010
The Underlying Assumption of the Leftist Taxers
In a review of some of the tax consequences of Obamacare, Grafton Willey conveys this bit of policy that one suspects underlies many of the assumptions of those who advance policies in the mold of nationalized healthcare:
Imposing a 3.8 percent "unearned-income Medicare contributions" tax on higher-income taxpayers. The 3.8 percent unearned-income Medicare contributions tax is imposed on the lesser of net investment income or the excess of modified adjusted gross income (AGI) over the threshold amount ($200,000 for single individuals or heads of households; $250,000 for married couples filing a joint return and surviving spouses; and $125,000 for married couples filing separate returns).Neither the $200,000 nor $250,000 amounts are indexed for inflation. Modified AGI is adjusted gross income increased by the amount excluded from income as foreign earned income less deductions attributable to such income.
Net investment income includes interest, dividends, royalties, rents, gain from disposing of property from a passive activity and income earned from a trade or business that is a passive activity. In determining net investment income, investment income is reduced by deductions properly allowed to that income.
Net investment income does not include distributions from qualified retirement plans, including pensions and certain retirement accounts. For example, income from individual retirement accounts (IRAs), 401(a) money purchase plans, 403(b) and 457(b) plans would be exempt.
Some of the hardest work that I've ever done was the back-room labor involved in selling fish from a truck, and there were times, while hauling crates in the snow or cleaning putrid wooden boxes in the beating sun, that I marveled that it should be so difficult to earn $7 per hour and wondered what one could possibly do to "earn" the salaries of the wealthy. (For clarity: I look back on those days very fondly and came around to appreciating them even while they were in process.)
I don't offer that anecdote as a means of transforming economic ignorance into a populist cry. To the contrary: the notion of "earned income" is hopelessly subjective and, therefore, merely a dash of political rhetoric to justify confiscatory taxation. Consider the amount of money that President Obama has earned as an author. Personally, I love writing and undertake it as a compulsion and balm. But in the course of lugging a table saw up the narrow steps to the third floor of a Newport mansion, I might be inclined to challenge the assertion that Mr. Obama "earned" that money in the sense implied by the Medicare tax.
May 29, 2010
A Direct Line from Health, Through Information, to Political Manipulation
The problem with giving government authority over everything is that, well, it gives government authority over everything. For a shocking example, consider Mark Steyn's description of a minor controversy in Great Britain.
It seems that, in the course of the recent election cycle, the then-ruling Labour party sent out postcards warning that, if victorious, the Conservatives would reduce access to breast cancer treatment. What's shocking is that Labour appears to have culled the list of all citizens to include only those who have" been either diagnosed with, treated for, survived or, in at least one case, died of breast cancer." Writes Steyn:
So a quantum leap in targeted marketing has just been made: The governing party of a free society was able to identify women with breast cancer in swing constituencies and send them a postcard warning that if you vote for the opposition they’ll cut off your chemo and kill you.
I suppose that's not much different than local school committees sending parents warnings that their children will have to return to paper-less one room school houses if they don't receive the budgets that they desire. The difference is that it's unavoidable for school departments to know which households have children in the school system, but at least in the United States, it isn't yet the case that political parties have ownership of everybody's personal health histories.
The easy availability of information has its pluses and minuses. The real danger lies in giving a centralized authority the power to use that information for its own purposes.
May 25, 2010
ObamaCare Less and Less Popular
Imagine how unpopular it will be when its costs really start to kick in:
Support for repeal of the new national health care plan has jumped to its highest level ever. A new Rasmussen Reports national telephone survey finds that 63% of U.S. voters now favor repeal of the plan passed by congressional Democrats and signed into law by President Obama in March.Prior to today, weekly polling had shown support for repeal ranging from 54% to 58%.
And by "costs," I don't mean just the direct cost to the federal government, which (for those who've forgotten) is not the sum total of the United States. For one example, Americans are pretty good at intuiting this sort of outcome:
A study by the National Center for Policy Analysis shows that tax credits in the new healthcare law could negatively impact small-business hiring decisions.The new law provides a 50 percent tax credit to companies offering health coverage that have fewer than 10 workers who, on average, earn $25,000 a year. The tax credit is reduced as more employees are added to the payroll.
The NCPA study finds the reduction in tax relief to be a cost concern for companies looking to hire additional workers, but operate on slim profit margin yet still provide employee health coverage.
Incumbents — making government less efficient and American life more difficult, year after year.
May 19, 2010
Complexity is Knowing that Government Control Must be Better, No Matter What that Pesky Constitution May Say
One of the more maundering sections in the Projo's recent Tea Party editorial began by looking at the view expressed at many Tea Party events that modern government needs to continue to be consistent with the principles of the founding of America...
They also make frequent reference to getting back to what the nation's Founders wanted, though it is not at all clear how the Founders would have governed a country that has grown from about 3 million people living in a mostly agrarian nation in 1790 to about 310 million in the highly urban/suburban, technological and multicultural one now. We do know that the Founders supported the right to amend the Constitution as things changed.The connection that the editorial seeks to establish, between simplicity and Constitutionality, is not at all clear. Given that defining and enforcing limits on the power of government has never been a simple problem for any society, it would have been helpful if the editorial board had discussed the specific Constitutional sections they believe to be too simplistic for a "highly urban/suburban, technological and multicultural" nation.But complexity is anxiety-provoking, while simple slogans are comforting.
Indeed, much modern history has been shaped by human struggles with and against the consequences of contrasting formulations of government. The renowned philosopher and sociologist Raymond Aron described the key contrast in the past two-and-half-centuries as being defined by the difference in the ideas of...
...representative governments restrained by the balance of power, and so called democratic governments invoking the will of the people but rejecting all limits to their authority.Then again, given the Projo editorial board's steady stream of editorials over the past year declaring the need for more government power over healthcare regardless of the details -- and perhaps the Constitutionality -- of the the plans that were being proposed, they may feel that the issue has been settled, with the latter view of government described by Aron having won out.
However, those who would feel comfortable with a system where the most important factor limiting a government's power is that government's ability to decide for itself when its actions serve true public interests really shouldn't be congratulating themselves on their ability to deal with complexity.
May 14, 2010
Why the Federal Health Insurance Mandate Cannot Be Made Constitutional By Calling it Tax
Article I, sections 8 and 9 of the United States Constitution originally defined the taxing authority of the Federal Government...
(s8) The Congress shall have Power To lay and collect Taxes, Duties, Imposts and Excises, to pay the Debts and provide for the common Defence and general Welfare of the United States; but all Duties, Imposts and Excises shall be uniform throughout the United States...(s9) No Capitation, or other direct, Tax shall be laid, unless in Proportion to the Census or Enumeration herein before directed to be taken.This creates two classes of taxes 1) "direct" taxes, which must be apportioned according to the census and 2) "indirect" taxes, e.g. taxes on commercial activity, transactions, etc. The Sixteenth Amendment to the Constitution extended the Federal taxing power to allow unapportioned taxes on income...
The Congress shall have power to lay and collect taxes on incomes, from whatever source derived, without apportionment among the several States, and without regard to any census or enumeration.Income has been defined broadly by the United States Supreme Court, in the case of Commissioner v. Glenshaw Glass, as "instances of undeniable accessions to wealth, clearly realized, and over which the taxpayers have complete dominion".
Not purchasing insurance is not income under the Court's definition of income because the non-purchase of insurance is not "an undeniable accession to wealth" and therefore cannot be taxed under the Sixteenth Amendment's grant of authority. Nor can the non-purchase of something meet the criteria of being subject to a directly apportioned or indirect tax, meaning that nothing in the Constitution allows the Federal government to tax an individual's non-purchase of health insurance.
But the dubious constitutionality of the Federal health insurance mandate doesn't end with this significant problem.
Congress and the President could have, in a clearly Constitutional manner, used its taxation power to influence the purchase of health insurance by creating a tax-deduction associated with the purchase of health insurance. This idea was, in fact, proposed by officials like President George W. Bush and United States Senator Ron Wyden. However, Congress chose not to go this route.
Given the current Federal tax code, such a deduction would extend an advantage already enjoyed by corporate purchasers of health insurance to individual purchasers of the same products. But in choosing not to create an individual deduction, and opting for a tax on non-behavior instead, Congress chose a mechanism of dubious Constitutionality specifically for the purpose of preserving an advantage that some purchasers of health insurance, i.e. the corporate ones, have over others.
One of the most fundamental purposes of a Constitution is to prevent a government from taking arbitrary actions that would favor some over others. When Congress stretches beyond its clearly enumerated powers, with the specific intent of preserving government created-advantages for some over others, it doubly violates the Constitution's reason for being.
May 10, 2010
Gov Calls on AG to Join Other States Challenging Healthcare Reform
I'd like to second this, along with Justin's reservations about "Obamacare". (The gov's office issued this press release a couple of hours ago.)
Governor Donald L. Carcieri today urged Attorney General Patrick Lynch to join 14 other states that have filed a complaint in the federal district court challenging the constitutionality of the federal healthcare legislation citing the new law as “a violation of the equal protection and commerce clauses and the 10th amendment, among other constitutional provisions.” In a letter to the Attorney General, Governor Carcieri writes, “Among the provisions of the recently enacted federal health care legislation is one which forces the citizens of Rhode Island to purchase health insurance and the state itself to form and participate in insurance exchanges; failure to comply can result in substantial fines.”The Governor called upon the Attorney General to “exercise its discretion to protect our citizens from this unnecessary and probably unconstitutional intrusion of the federal government into the lives of Rhode Islanders whose freedoms to make their own choices about health care should be preserved and protected.”
Governor Carcieri cites the 10th amendment of the United States Constitution, which clearly defines that there are limits to federal powers and places where only the State and its citizens have authority to act.
A critic of the process by which the health care legislation was passed, Governor Carcieri reinforced his concerns that the law will “raise the costs of health care to Rhode Islanders, lower the quality of care, and shift another unfunded mandate on a state already overburdened with budget deficits.”
Insurance Doesn't Mean Health
Duncan Currie explains why it is speculation to assert that increasing health insurance coverage will mean improving health and decreasing avoidable deaths (subscription required). For the most part, it's a problem of separating data points. This part, however, moves beyond the immediate question and gives some reason to worry about the effects of ObamaCare, moving forward:
Here's another reason we should not expect the landmark bill to yield major health gains: A hefty chunk of the newly insured under Obamacare — anywhere from 15 million to 18 million people, according to projections — will rely primarily on Medicaid for their insurance. Unfortunately, the fact that Medicaid reimburses participating providers at low rates has made it increasingly difficult for recipients to find doctors. In a 2008 survey, only 40.2 percent of physicians told the Center for Studying Health System Change that they were accepting all new Medicaid patients, and more than a quarter (28.2 percent) said they weren't taking any. It can be even harder for Medicaid patients to locate dentists.And yet this is the program that will soon be flooded with a massive wave of new enrollees. Dr. Edward Miller, dean and CEO of Johns Hopkins Medicine, has written that "without an understanding by policy makers of what a large Medicaid expansion actually means, and without delivery-system reform and adequate risk-adjusted reimbursement," Obamacare "will have catastrophic effects on those of us who provide society's health-care safety-net."
One foreseeable government "fix" will be a requirement that doctors not consider the type of coverage that potential patients have, forcing them to take all comers for whom they have room in their schedules (probably with regulations of how many patients doctors must accept). If that comes to pass, established doctors may just stop taking new patients at all, they might charge privately insured patients even more, or they might just quit the field.
May 4, 2010
The Healthcare Bill Due to Come Due
A recent essay in National Review by Avik Roy takes up the topic of healthcare inflation resulting from ObamaCare (emphasis in original):
Consider the numbers: Based on the gimmick-free assessment of former Congressional Budget Office director Douglas Holtz-Eakin, from 2010 to 2019 the act will increase the debt by $562 billion — almost $5,000 per household. Not great news, to be sure. But a PriceWaterhouseCoopers analysis projected that, over the same ten-year period, Obamacare will increase the cost of health insurance by approximately $20,000 per family.This cost will be borne primarily by the young, who will be forced to subsidize the care of the middle-aged; by freelancers and small-business owners, who will not benefit from the exemptions afforded to large, self-insured employers; and by middle-class families, who will most feel the squeeze of higher insurance costs yet will also be expected to finance the health care of others.
The effects of this legislation on the debt are worrisome indeed. But, barring a Weimar-style collapse of the U.S. economy, they will be less visible to the typical family than health-care inflation will be. Rapidly rising insurance premiums will blow a hole directly in the monthly paychecks of tens of millions of middle-class households.
Mandates, consumer incentive to avoid "insurance" until it's actually needed, redistribution of costs from people in public programs to people with private insurance, and protection of monopolistic players are some of the ways in which the Democrats' big-government variation of "reform" will only exacerbate our healthcare system's current problems.
When polls ask about support for reform, respondents mean (or ought to mean) government action in pretty much the opposite direction from that which the Democrats have taken. That's why even in Rhode Island a majority supports repeal of ObamaCare.
April 24, 2010
Still Spinning Healthcare Down, Although Up
This won't be the first such report:
... the [Health and Human Services Department] analysis [of the healthcare legislation] also found that the law falls short of the president's twin goal of controlling runaway costs, raising projected spending by about 1 percent over 10 years. That increase could get bigger, since Medicare cuts in the law may be unrealistic and unsustainable, the report warned.It's a worrisome assessment for Democrats.
In particular, concerns about Medicare could become a major political liability in the midterm elections. The report projected that Medicare cuts could drive about 15 percent of hospitals and other institutional providers into the red, "possibly jeopardizing access" to care for seniors.
Recall that what little actual support there was for this legislation, and what broad support there was for "need reform" questions, had to do with getting costs under control. Now the spin is that the legislation will only add 1% to costs. Of course, that's still taking into account cuts and changes that aren't politically plausible or financially workable.
Not for no reason does the legislation delay the bulk of its provisions until after a couple of election cycles. Life in the United States is about to become substantially worse, at least for those who have the misfortune of becoming sick or needing a job or not being rich or well connected.
April 23, 2010
Bishop Tobin Won't Let Catholicism Just Be a Brand
As much as it's disappointing to see division among Catholic organizations, unity can't be the core principle of any group that actually believes in anything. That is to say that I think Bishop Thomas Tobin got this one right:
Following a statement issued by the U.S. Conference of Catholic Bishops expressing regret that health care reform came with the possibility of expanded abortion funding, Bishop Thomas J. Tobin sent a letter March 29 to Sister Carol Keehan, the president and CEO of the Catholic Health Organization, requesting that St. Joseph Health Care of Rhode Island be dropped from the organization's membership and expressing his disappointment that the CHA, under her leadership, publicly endorsed the legislation that was signed into law.Breaking with the position of the U.S. Bishops who support health care reform without federal funding for abortion, Sister Carol Keehan, a Daughter of Charity, said that "while not perfect, the reform law significantly expands coverage, especially to low-income and vulnerable populations, and is a tremendous step toward protecting human dignity and promoting the common good."
Just as Catholicism isn't only an ethnicity, it isn't only an organizational brand.
April 16, 2010
The Way to Government Ownership
Since I mentioned, earlier this morning, the government's "overtaking of healthcare," it's relevant to point out an explanation offered in a recent National Review, in the magazine's short-take "The Week" section (subscription required):
American college-loan policy offers an illustration of how the government can absorb an activity incrementally, claiming to cherish the benefits the private sector provides until the bait has worked and it's time for the switch. Government support for student loans began in the form of subsidies for private loans, much as the Democrats' health-care bill would succor the insurance industry by subsidizing its product while forcing people to buy it. In the 1990s, Democrats added a "public option" — making government the direct provider of some student loans — with the Clinton administration claiming that "students and schools are served by healthy competition" between the private sector and the government. This is the same rhetoric Obama used when he tried to sell us a public option for health care. And now we see how quickly Democrats dispense with the rhetoric of competition when a government takeover seems viable: The new student-loan bill would make the public option the only option, thus completing the absorption of the activity. In a similar way, the current health-care legislation isn’t the endgame.
Government ownership of student loans gives politicians strong influence over your career. Healthcare will do the same to your body.
April 13, 2010
The Nanny State Will Tax Your Skin
Fellow blogger and Providence Firefighter/EMT Michael Morse and his wife sent an op-ed to the Providence Journal objecting to an Obamacare tax on tanning salons:
A small group will be the first to pay for national health-care reform, the first to put their hard-earned dollars into the system. Starting July 1, they will pay 10 percent more for a service that helps them feel better and look better and promotes healthy living.You can’t tax sunshine, right? Think again. The indoor-tanning industry, mostly small-business owners, the majority of them women, has been singled out to provide funds for a program that claims to be equitable for all.
As they note, other skin-related professions avoided proposed taxes because of the size of their lobbies and the urge to protect people from themselves that has begun to creep from smoking to tanning (let alone eating fast food). For their part, the Morses dispute the ill effects of artificial tanning on health.
Personally, I think that's besides the point. It isn't the role of government to impose a healthy lifestyle on individuals, especially with matters of such long-term repercussions as exposure to light. We'd best get used to it, though. With the government intimately involved in our healthcare system — even more than was already the case — your every behavior is now a matter of interstate commerce.
April 8, 2010
Can You Hear the Sly Taxation?
Bills have been introduced by Sen. William A. Walaska (D-Dist. 30, Warwick) to increase medical insurance coverage for hearing aids and to require insurance coverage for surgery and services associated with hearing aid implants.
Without a doubt, hearing loss increases the difficulty of one's life. So does poor eye sight and any number of other ailments and disabilities. There are two problems with this continuing trend of legislating mandatory insurance coverage for related aids, medication, and surgeries:
- It essentially turns insurance premiums into a tax to fund redistributed wealth, without allowing voters a direct influence on those increasing the cost/tax. In other words, the government is making the insurance companies levy a tax and block the political heat.
- Determining how much addressing each health difficulty is worth works best on a case-by-case basis, and when somebody else is forced to pay for the remedy, nobody in the chain from provider to patient has significant incentive to make actual, often difficult decisions, thus driving up costs all around.
But, as I said, there's a firewall against political heat built into this practice, so the politicians will keep doing it until we all decide to reassert basic principles of good governance.
April 7, 2010
Perhaps Healthcare Will Be a Catalyst, at Least for a Permanent Alarm
Theodore Gatchel raises the operative question with regard to the reaction to the content and process of the new healthcare legislation:
On the positive side, the process the Democrats have used to pass this legislation appears to have caused more Americans than ever to read the Constitution.The more they read it, the more they question not just the legitimacy of this particular process, but also how the immense power of today's federal government can be reconciled with any common-sense reading of the Constitution.
As Gatchel suggests, part of the answer will depend on the direction that the Democrats head from here. If they wipe the dirt off their hands and govern quietly from the center at least through the next election, public ire might subside. If they continue with their radical agenda, whether on immigration, energy, unions, or what have you, they'll reinforce public opposition.
On the other hand, even in our little blue, heavily propagandized state, we've seen people newly involved in a way that suggests a long-term commitment — and a long memory. Even if the politicians manage to lull a critical mass of Americans back into apathetic slumber, there is now a huge nationwide infrastructure for sounding alarms.
April 6, 2010
The Healthcare System Sinking In
It's probably not really worth mentioning, but Joe Baker's column in yesterday's Newport Daily News is an astonishing bit of cheer leading for the policies of the Obama administration. Most of it has to do with the economy and how wonderfully the stimulus program worked. Perhaps it's enough to note that he claims the recovery on which he's so bullish is "in the rebound a lot quicker than was being forecast when we were in the pits of despair last year."
My recollection is that, in the pits of despair, economists were predicting a clear recovery before 2010. If we find ourselves emerging from the darkness only a couple quarters later, that'll be wonderful, but I'd advise against managing your finances as if flush times are just around the corner.
What's really astonishing about Baker's essay comes when he decides that singing about rainbows in the economy isn't adequately partisan:
Republicans who went to the wall in an attempt to kill the health care reform measure were hoping for a rising backlash from its passage. But that hasn’t materialized, and as the reality of the program sinks in and nobody sees the dire consequences predicted by its opponents, methinks a lot of the remaining anger will float away.
Does this guy get his news purely from Obama press releases? Put aside the fact that he ignores the delay on most of the bill's provisions. One gathers that Baker missed the financial statements of major companies expecting billions of dollars lost to their bottom lines because of the legislation. Moreover, on the same day that Newport County's major daily paper handed its readers Baker's bubblegum, the state's major daily paper was informing its own of the following, on its front page:
While some experts are predicting better times for hospitals from the national health-care overhaul, an analysis conducted for the Hospital Association of Rhode Island predicts that the state's 11 acute-care hospitals stand to lose $465.7 million over the next 10 years.The study found that any gains from more patients coming through the doors with insurance will be more than offset by cuts in payments the hospitals receive from the federal government, according to Edward J. Quinlan, the association’s president.
An accompanying article suggests that the government has a history, in this area:
Quinlan traces the hospitals' troubles back to the passage of the federal Balanced Budget Act of 1997, which led to steep cuts in Medicare payments. The association estimates that over 13 years, the cuts have resulted in a loss of $700 million. Medicare payments used to provide hospitals 14 percent more than the cost of care, providing a necessary buffer to help pay for general hospital expenses. Now the payments are about 89 percent of the cost of care.
Just wait until employers start dumping their workers into publicly subsidized programs. And just wait until this guy's ilk get the reins firmly in their hands:
Health-care reform may bring some relief. But Nick Tsongias, an executive board member of HealthRIght, which supports comprehensive health-care reform, says there's an even deeper problem to address."I think the business model that the hospitals are operating under is now obsolete," he says. ...
... increased competition isn't necessarily beneficial, says Tsongias. In fact, he says, it can be harmful. For example, Landmark Medical Center started a coronary-care unit, but had to close it down because it contributed to financial losses so severe the hospital had to seek protection from the courts, he says.
"It certainly poorly serves the public if the way we determine how many hospitals we have, and what the appropriate array of services are ... is through survival of the fittest," Tsongias says.
Competition leads to efficiency. Indeed, Tsiongas's complaint is that it drives down prices to the point that only the most effective providers can continue to profit from a particular good or service, and what ultimately makes them effective is that consumers wish to spend their money with them. I'm not an expert in hospital finance, but I'd wager that the reason hospitals have chased a narrow collection of identical services is that a mixture of government regulations and insurance company policies have created inadvisable incentives through mandates and the speed and percentage of payments.
The better approach to lowering costs and broadening care would be to allow consumers to pay more directly for the services that they want and need. Further embedding the "insurance" model — really a "healthcare services plan" model — and giving government regulators a more direct responsibility for and authority over the healthcare system will only yield additional strains on providers and higher costs. Which will only yield fewer providers and even higher costs.
I'd much rather live in Mr. Baker's world, in which one can trust that the cool smart guy running the show in Washington would manage of our every worry. We could all relax and be taken care of. Unfortunately, in the world that I've observed, that's just not realistic.
March 30, 2010
Media Message: Healthcare Simply Rosy
As Marc mentioned this morning, large companies have been assessing the direct cost of the Democrats' healthcare plan to them (i.e., their employees and customers) in the billions of dollars, and Congress has responded by "fuming." Those who read the from the mainstream media and left of there wouldn't have heard much about it, though.
I haven't combed the Providence Journal but about the closest thing to an admission that the healthcare plan might have such negative effects that I've noticed in the Providence Journal has been a column by John Kostrzewa saying that "nobody has a clear answer" the the question of whether small businesses will see their own costs rise. My general assessment, to which Kostrzewa alludes, is that the plan will wind up saving small businesses money inasmuch as they'll simply pay the government fee for unloading their employees into healthcare exchanges and any federal plans that pop up.
There could have been a healthcare reform in which that sort of switch would have been positive, but it would have been based on an increase of choices and decrease in mandates. Such an approach would lead employees to opt to fund their own healthcare and thereafter pressure their employers to give them some of the savings in increased pay. At the same time, consumer-controlled demand would have brought prices down.
As it is, healthcare costs will continue to rise, and small businesses will see canceling healthcare benefits as a necessary savings measure, so the push to split the savings with employees will not be as strong (at least for those employees who need the most help improving their hands in the power game)
Big Business v. Big Government on Healthcare
Big Business learns that Big Government giveth and taketh away:
On Capitol Hill and in the White House on Monday, Democrats were fuming over a series of announcements that started Friday from Fortune 500 firms saying their bottom lines will take huge negative hits because of changes in tax law mandated by Obamacare. That hit in turn means lower profit projections. Caterpillar estimates, for example, that Obamacare will cost it $100 million; John Deere faces expenses of $150 million; 3M, $90 million; AK Steel, $31 million; Valero, $20 million. And then there's AT&T, which is marking its balance sheet down by a whopping $1 billion. All in all, the Wall Street Journal estimated a $14 billion haircut for these corporations.Under post-Enron accounting rules, the corporations were required to revise their projections to account for the effect of Obamacare on their bottom lines. The effect is negative because Democrats, in their zeal to raise revenues and improve Obamacare's claimed effect on the federal deficit outlook, took away a tax break these companies needed in order to supply prescription drugs to their retirees. The tax subsidy, itself a government accounting ruse crafted in 2003 by the Republican Bush administration to dissuade corporations from dumping their retiree drug benefit programs on the then-new Medicare Part D, becomes taxable under Obamacare. Corporations are now being reminded of the harsh truth: What Big Government giveth, Big Government taketh away, too.
March 27, 2010
The Constitutionality Proof Is Worse than the Pudding
Ed Fitzpatrick's column, yesterday, suggests that the healthcare law, including the individual mandate, is constitutional, but one needn't be as far right as Anchor Rising to be very concerned about the reason:
The Supreme Court has held that Congress "can tax for any legitimate reason, and certainly providing health care for all Americans is a legitimate reason," Goldstein said. "It was imposed based on Congress' reasonable conclusion that when some people don't have health insurance, it hurts them and shifts a lot of costs onto the rest of us. The tax is little different than taxes Congress imposes on companies that pollute, which are similarly based on the conclusion that pollution hurts everyone and could be deterred through a tax."Also, the high court has upheld Congress' power to regulate "economic activity that substantially affects interstate commerce," Goldstein said. "And there is no question health care and health insurance affects interstate commerce."
So, not taking care of your own health is like large factories' polluting the air and your health-related habits also affect interstate commerce, making them a legitimate target for regulation and taxation. I took up this topic in a Rhode Island Catholic column a few months ago. The question arises: under such reasoning, what doesn't Congress have the authority to regulate?
Statists already would have answered "nothing," but shouldn't we find it frightening to stare down this dark slope? Now, not only is the authority asserted, but the federal government has a massive new entitlement to bolster and defend by making the American behave in particular ways.
March 25, 2010
After the Legislation, the Deluge
This might be the most frightening thing related to the healthcare legislation that I've read thus far:
Dr. Nick Tsiongas, who sounded jubilant when reached by phone Monday, actually agrees with Purcell that the bill is weak on cost control. But Tsiongas, who founded the local reform group HealthRIght, believes the federal legislation will allow Rhode Island to tackle that issue. The federal subsidies are necessary to cover the uninsured, he said. "It establishes a platform on which state reforms can now begin to take hold," he said.
Take hold like a hand around a throat. You may recall Dr. Tsiongas from one of my vlogs:
At Rep. Patrick Kennedy's townhall-esque AARP meeting, Tsiongas explained his desire to pool all of the money currently in the Rhode Island healthcare system — public and private — so that he and his fellow experts could allocate it in a way that they consider to be rational, determining such things as how much of each medical technology is available in the state. His jubilation at the "platform" that enables him to reach such goals is evidence enough that Congressional Democrats and President Obama have done a very bad thing, indeed.
Spotting the Spin in the Fact Check
Perhaps you've noticed the newspaper fad, in recent months, of printing "fact checks" that purport to offer readers a balanced and objective assessment of the spin surrounding various issues. I stopped bothering with them after the first couple, when it occurred to me that the articles are mainly useful for bloggers still interested in spotting media bias. In a recent example concerning the healthcare legislation, Ricardo Alonso-Zaldivar strives to explain how both sides are spinning the issue. The problem is that his fact checking of the opposition doesn't really present actual myths or the facts that debunk them.
The first "myth," for example is that "Obama has put the nation on a slippery slope toward socialism." The "fact" is that the nation has been on that slope for a while and still has farther to go until it reaches bottom. I don't know of anybody, on the right, who disagrees, so it appears that Alonso-Zaldivar has debunked a strawman.
When he gets to the question of abortion, it's not at all clear that the reporter has done any research about the actual arguments being made:
You will be forced to pay for other people's abortions.Only if you join a health insurance plan that covers abortion. In that case, the costs of paying for abortions would be spread over all the enrollees in the plan—no differently from how other medical procedures are handled, except a policyholder would have to write a separate check for it.
Timothy Jost, a law professor at Washington and Lee University, said people who don't want to pay for abortion could simply pick a plan that doesn't offer it.
There would definitely be a demand for such plans, and not just from people with moral objections. Single men and older women would have no reason to pay an extra premium for abortion coverage.
The point isn't that the government will force us to join healthcare programs that offer abortion. The point is that the government will be subsidizing, with our money, the premiums of people who do.
However one feels about abortion or healthcare or socialism, it remains necessary to adjust for the medium through which one acquires news. Spin is chronic and addictive.
Except on Anchor Rising, of course, where all of our facts and conclusions are entirely objective.
March 23, 2010
Rhode Island's Lesson for America
It's been an education in the future of healthcare in the United States to watch Rhode Island's three insurers seek rate increases from the state as the Democrats have forced their legislation through Congress. On Thursday, the state health insurance commissioner, Christopher Koller "slashed" proposed premium increases and:
... that's not the only effect: Koller also reallocated how insurers should spend their premium dollars.He ordered Blue Cross & Blue Shield of Rhode Island and UnitedHealthcare of New England to spend less than they had proposed on hospital care — a decision that could pressure insurers to negotiate lower payments to hospitals, at a time when hospitals are losing money.
The usual suspects are demagoguing about ruthless insurance companies and their endless rate increases, and Mr. Koller is bringing up "troubling trends," such as the unexplained fact that the average age of people receiving health coverage through work is going up, adding to premiums. Nobody is questioning the wisdom of allowing an unelected bureaucrat to manage every insurer in the state:
Koller does not merely rule on the total premium, but examines the factors that the insurers say underlie their need for more money — the costs of hospital care, medications, primary care, administration and profits. His only changes were: reducing inpatient and outpatient hospital costs at both Blue Cross and United, increasing United's primary-care costs, and slightly cutting the administration and profits at Blue Cross. ..."We need to make the status quo as uncomfortable for insurers and providers as it is for employers, the people who are paying the bill," he said.
Is a healthcare system built upon mutual discomfort really the most effective approach? Artificially suppressing prices doesn't affect the factors driving those prices up, and however much provider and insurer greed may play a role, the limited number of choices, the disguising of costs within broad premiums and through government subsidies, and the requirements and restrictions that the state government places on the market are exponentially greater factors.
If we wish to bring down costs, we're going to have to increase the degree to which consumers must consider the price of each service. Unfortunately, our government — convinced of its own need for more power — is moving in the other direction. With the intention of taking decisions out of the hands of insurers, government operatives are pulling them into their own.
At least if consumers were unhappy with the deals offered by Blue Cross, they could switch to United (and now Tufts). What are our options supposed to be if we're not happy with the decisions of Mr. Koller? And why would additional companies choose to operate within a state (or nation) in which such a functionary ultimately runs their operations?
March 22, 2010
Patrick Lynch Not Interested in Challenging the Federal Government's Power to Impose a Purchase Mandate on Individuals
According to Steve Peoples of the Projo's 7-to-7 newsblog, Rhode Island Attorney General Patrick Lynch (to no one's surprise, really) is not interested in joining a potential lawsuit by the states challenging the Federal government's power to require that individuals purchase something...
"I don't like a lot of the decisions that the legislature makes every day. Do I go up and sue them? And do you have the basis to do so, more to the point?" Lynch said in a late-morning interview, characterizing the looming lawsuits in a dozen states as "political posturing....But at the outset, moments after the vote, when they're crying and putting up [lawsuit threats] on Facebook in Texas first, there's a procedure that we go through as attorneys general when something is more substantive, and this seems to be a partisan driven mechanism," said Lynch, a Democratic candidate for governor."To me it's a moment that should be celebrated," he said of Sunday's health-care vote.
At Some Point After Healthcare Reform Kicks In
Not understanding this. Long waits and worsening care. Costs increasing - strange, why didn't price controls take care of that? Looks like we're gonna need to do some more revenue enhancing.
Doctors dropping out. (Huh. Wonder if that's related to the price controls.)
Most doctors have stopped taking Medicare patients? Well, a "universal coverage" addendum ought to take care of that. If doctors don't accept Medicare patients, they won't get any reimbursements from us! That'll fix 'em.
Whoops, fraud and abuse up double digits. That's right, we never did get around to re-deploying those IRS agents.
Unemployment rate creeping up. That's got nothing to do with healthcare reform, though ...
Gee, looks like nobody has access to good healthcare now. ... Well, other than Congress and the very rich, of course. (Color me embarrassed on THAT point!)
Good thing Speaker Kucinich (and how funny is that! but it was the only way to keep his support) has convened a study commission. We'll get to the bottom of this, no matter how many junkets and how long it takes!
Okay, what's on the calendar? This afternoon - hearing to telescope med school and eliminate residency periods. Gotta get more docs pumped out. And tonight - oh, excellent, the trial lawyers' fundraiser. They've been a rock through all of this. Let's see. "Just keep saying no to tort reform!" H'mm ... "Together, we can hold off the scourge of tort reform!" Better! Must remember to hold up clenched fist ...
Your Democrat Congressman
We Awake in a Different Country
For almost a year, the people of the United States have taken every opportunity to tell their "representatives" not to absorb our healthcare system into the government. Tea Parties, town halls, elections (even unto taking a Massachusetts Senate seat out of Democrat hands), and poll after poll after poll. They didn't care. They've lied. They've gamed every internal analytical system, such that the Congressional Budget Office had to find falsely a deficit reduction. They've taken key votes on hidden days, even Christmas Eve. They've overtly bribed members. They've manipulated the legislative process. And now, like it or not, America, they've forced the costly, detrimental lemon down our throats:
A bloc of pro-life Democrats turned out to be the linchpin to passage of the Senate's massive health insurance overhaul Sunday night, as President Obama cemented a 219-212 victory with a pledge to issue an executive order "clarifying" abortion language in the Senate bill.The House also voted 220-211 to support a "reconciliation" bill aimed to "fix" provisions in the Senate bill that many House Democrats opposed but viewed as better than nothing.
The one monomaniacal call that must now replace every objection that the American people have raised over the past year is: Repeal.
ADDENDUM:
Here's the vote list. Consult it before you ever vote for an incumbent of this Congress for so much as town garbage sorter.
March 21, 2010
Will Patrick Lynch be Getting a Phone Call Tonight...
...and do we have a new issue in both the Rhode Island Attorney General's and the Governor's races, based on this facebook post from the Attorney General of Texas (h/t NRO)...
Texas attorney general Greg Abbott Facebooks: "I am organizing a conference call tonight for AGs across the country. We will discuss our litigation strategy about the healthcare bill. I will update you on Facebook after the conference call."
Breaking: The Stupak Sell-Out
The Stupak pro-lifers have accepted an executive order for their votes:
Stupak announced support for the bill as the White House issued its statement about the executive order.The president "will be issuing an executive order after the passage of the health insurance reform law that will reaffirm its consistency with longstanding restrictions on the use of federal funds for abortion," reads a statement from White House Communications Director Dan Pfeiffer.
As they're arguing in the Corner, an executive order simply doesn't do the trick. Kathryn Lopez: "I think we're witnessing Bart Stupak write the obit for the concept of the 'pro-life Democrat.'"
As a local matter, he may be writing the obituary for Jim Langevin's seat in Congress. If this is what pro-life Democrats get for their votes, they ought to throw the next primary to Betsy Dennigan and then vote Republican or independent as a lesson.
Re: Sunday Healthcare Whip Report
Stupak is now officially a "yes". National Review Online has identified 3 pro-life Congressmen that may not go along with the executive order solution. Two of them, Dan Lipinski and Jerry Costello both of Illinois, are on the Firedoglake Stupak-list. A third, Gene Taylor was already counted as a "no".
Earl Pomeroy has declared he is a "yes".
If we put the 7 remaining from the Stupak bloc as "yes" votes, plus Pomeroy, the Democrats now have 216, no matter how the remaining undecideds break (trusting the FDL information and the NRO report to be accurate).
UPDATE (5:08 PM)
...although the New York Times lists only 5 official "yes" votes, Stupak, Driehaus, Dahlkemper, Rahall and Mollohan.
Sunday Healthcare Whip Report
Firedoglake is reporting that Marcy Kaptur of Ohio, who had been in listed in their Stupak bloc (don't know that we can really call them pro-lifers as a group anymore) will vote "yes" regardless of any changes in abortion language. Bart Stupak's statement that he has 6 members in his bloc suggests least one or more of the others in the FDL "Stupak" category might go "yes", regardless of changes or non-changes that happen today. Reportedly, Stupak is negotiating with the White House on banning public funding for abortion via executive order, meaning the EO strategy could win his vote and the votes of his bloc.
FDL is also mentioning that Rick Boucher of Virginia, who they had as a "no" but other sources had as undecided, is a potential undecided. And no one is sure what Loretta Sanchez of California is going to do. All that taken into consideration, I'l interpret the FDL reports as saying 206 Yes, 207 No, 9 generic unknowns, 9 potential members of the Stupak bloc (but at least one who is probably already a "yes").
Fox News hasn't moved their tally from 216-215; I'm not sure where they had Kaptur before. The New York Times is enjoying Sunday Brunch.
UPDATE (12:32 PM)
Something is up with the Stupak discussions with the White House. A press conference that was supposed to have been held at noon has been cancelled. Nothing definitive has been reported yet.
Also, there appears to be one New England vote still undecided. Firedoglake has Michael Michaud of Maine as an undecided potential Yes-No flip, though the New York Times has him as a "yes". The Bangor Daily News reported yesterday...
With a historic vote on reforming the nation's health care system looming on the horizon, Rep. Michael Michaud isn't tipping his hand. In a prepared statement on Friday, Michaud said he is still reviewing the contents of the reconciliation package unveiled Thursday by fellow Democrats in the U.S. House...As of Friday afternoon, Michaud was the only member of Maine’s congressional delegation still on the fence about the legislationDepending on what is happening with the Stupak bloc, one question may become how well having to campaign as "the man who decided to bring socialism to America" will go over in Maine.
UPDATE II (12:49 PM)
Firedoglake is reporting that MSNBC is reporting that the Stupak bloc has accepted the Executive Order, and will vote for the bill.
By FDL's count, one more commitment is still necessary to get the democrats to 216 (assuming they now will get all 9 of the Reps listed under the Stupak bloc). Could we see any confusion about Loretta Sanchez clear up very soon? I suspect she could weather the title of "the bringer of socialism to America" title better than Mike Michaud could.
UPDATE III (1:08 PM)
Here's the banner from MSNBC...
BREAKING NEWS: Sources tell NBC News that Rep. Stupak to vote yes on health care billNo link provided, no word from Rep. Stupak himself yet.
UPDATE IV (1:17 PM)
Robert Costa of National Review Online is confirming Stupak as a "yes".
UPDATE V (1:30 PM)
Fox News is reporting that Brian Baird of Washington has announced he will vote for the bill, and they've moved their tally to 217-214.
Baird was on the Firedoglake list of unknowns, which means if all 9 of their Stupak bloc members come over, their tally is 216 votes in favor of passage. Baird, by the way is retiring from Congress.
UPDATE VI (1:42 PM)
Hold on a sec: a conservative group-blog (NRO) is linking to a twitter feed from a producer at an all-news network (CNN) which says...
Urgent -- Rep. Stupak to CNN producer Lesa Jansen: "I'm still a no...There is no deal yet. Its a work in progress."However, the feeling among the commentariat is that something will be worked out.
UPDATE VI-B (1:54 PM)
Roll Call says...
Despite reports to the contrary, House Democratic leaders insisted Sunday that they do not yet have the support of anti-abortion-rights Rep. Bart Stupak (D-Mich.), who has been leading a bloc of key holdouts on the bill.MSNBC reported earlier that Stupak — and others opposing the final health bill over the abortion language — would vote in favor. But according to Brendan Daly, spokesman for Speaker Nancy Pelosi (D-Calif.), “MSNBC is wrong.”
“We hope so, but it hasn’t happened yet,” he added.
UPDATE VII (2:01 PM)
The New York Times is reporting that John Tanner of Tennessee, who was undecided, will remain a "no". Firedoglake is reporting that Lincoln Davis of Tennessee will also vote "no", and that Bill Foster of Illinois will vote "yes".
That puts the total at 208-209, 5 generic undecideds (4 of whom voted yes on the previous bill), 9 members of the Stupak bloc possibly waiting on the outcome of the executive order deliberations.
A Little More Context for the Vote
As the national Democrat Party does back flips to pass its healthcare monstrosity, there's are important bits of context of which we shouldn't lose sight. The first is that: "Job loss has been a big factor in the loss of insurance coverage, but not the only one," and job loss has been the sickly child in the room that Congress has ignored in its fixation on further nationalizing healthcare. Here's the second:
"Nobody is saying that providing coverage for those Rhode Islanders who are fully or partially uninsured won't cost anything," [Owen] Heleen, of the Rhode Island Foundation, said. "We all know it's going to cost something. That's much of the fight going on in Washington."Said Koller, the health insurance commissioner, "You need significant federal money if you want to reduce the number of uninsured — unless you want to reduce the benefits for everyone else, and that's a nonstarter."
"It's not something we can solve ourselves," [Deb Faulkner of the Rhode Island-based Faulkner Consulting Group] agreed. "We can do our own Rhode Island thing, but we need their money."
But somehow, coming up with that money at the federal level is going to reduce the national deficit. Got it?
March 20, 2010
Healthcare Whip Report
As of 8:15 pm, Fox News says there are 217 votes in the House of Representatives in favor of passage of the Democratic healthcare reform bill (216 are necessary for passage). National Review Online is reporting that a Maryland Congressman has said that he's "not sure" that the Democratic leadership needs the the Bart Stupak pro-life bloc in order to pass its bill.
On the other hand, the liberal website Firedoglake has posted its own tally of "unknowns". According to the numbers there, the Democrats have to pick up all 10 of the Congressmen listed as unknown (Rep. Jim Matheson has already gone "no") plus at least 2 of 10 from the Stupak bloc, in order for the healthcare bill to pass. A few hours ago, they had Zack Space of Ohio listed in their Potential Yes-No flips (he is now a "no"), so there seems to be something to their breakdown.
National Review Online, as of 8:15, says the current tally is 208-214 with 9 undecideds. That's close to the Firedoglake result, if you count the 10 Stupak bloc members as "no" votes.
If the Dems do have more than they need, Zack Space would be good choice to release, as Firedoglake notes that his district was +7 Republican in the Presidential election.
I have no idea what information is fully reliable, and what's being put out (by the politicos, not the news sources) for tactical purposes.
UPDATE I (8:33 PM):
Since I posted the original item, Fox news is now reporting 218 votes in favor of passage.
UPDATE I-B (10:07 PM):
Fox is back to 217-214 in favor. The New York Times also has a tracker up and is reporting the current state of affairs as 207-206 with 18 undecided.
UPDATE III (11:59 PM):
Glenn Nye of Virginia, a potential No-to-Yes Flip on the Firedoglake list has told his local paper he is a "no". If I'm counting this right, the Firedoglake tally is 204 Yes, 208 No, 9 generic unknowns, and 10 undecided members in the Stupak pro-life bloc. Passage now requires 3 members of the pro-life bloc to support the bill, if all 9 of the other unknowns decide "yes".
FDL is also indicating that a current "yes" has switched to "no", but the Congressperson hasn't said it herself yet.
UPDATE III-B (12:12 AM):
And Fox is now at 216-215. The New York Times has apparently gone to bed for the evening. Clearly, they've never heard Huey Lewis' The Heart of Rock and Roll.
UPDATE IV (1:15 AM):
Solomon Ortiz of Texas has issued a statement saying he will vote "yes", taking himself off of Firedoglake's potential Yes-To-No list. Let's call it 205 Yes, 208 No, 8 generic unknowns, 10 members of the pro-life group.
UPDATE V (1:32 AM):
One more, and I'm done for the evening. Bart Stupak in Roll Call says that he has six votes in his pro-life group...
Stupak, who once spoke for a dozen Democrats who were prepared to vote against the bill unless his strict abortion restrictions on insurance coverage were adopted, told reporters Saturday that his group was down to six, and he did not know if that would be enough to block the bill.Working off of the Firedoglake list, I think the implication is that the Democratic leadership can pass the bill by finding some compromise (an executive order?) softer than the full Stupak amendment that would satisfy four of the members of the pro-life bloc, plus get support from 5 out of 8 of the generic undecideds.
March 19, 2010
The Democratic Healthcare Penalty on Lower-Income Employees
Here at Anchor Rising, we slog through the dreck, so you don't have to! The paragraph below is some less-than-transparent text from the House reconciliation bill on healthcare "reform" (i.e. the dreck)…
[SEC. 1003(b)] APPLICABLE PAYMENT AMOUNT -- Section 4980H of such Code, as so added and amended, is amended-- (1) in the flush text following subsection (c)(1)(B), by striking ‘‘400 percent of the applicable payment amount’’ and inserting ‘‘an amount equal to 1⁄12 of $3,000’’;To unravel the meaning of such epic prose, we'll start from the beginning. The title of "Applicable Payment Amount" suggests questions of 1) applicable to whom and 2) payment for what. For answers, we have go to the details of section 4980H(c) of the original bill (which starts on page 350). The title of 4980H(c) right away gives us the whom…(2) in subsection (d)(1), by striking ‘‘$750’and inserting ‘‘$2,000’’…
LARGE EMPLOYERS OFFERING COVERAGE WITH EMPLOYEES WHO QUALIFY FOR PREMIUM TAX CREDITS OR COST-SHARING REDUCTIONS.The section specifically addresses employers offering coverage, not the ones who don't. No ambiguity there.
Moving down to subsection (c)(1)(B), we find a set of circumstances that trigger a tax-penalty…
‘‘(B) [If] 1 or more full-time employees of the applicable large employer has been certified to the employer under section 1411 of the Patient Protection and Affordable Care Act as having enrolled for such month in a qualified health plan with respect to which an applicable premium tax credit or cost-sharing reduction is allowed or paid with respect to the employee, then there is hereby imposed on the employer an assessable payment equal to the product of the number of full-time employees of the applicable large employer described in subparagraph (B) for such month and an amount equal to 1⁄12 of $3,000.Read that section carefully citizens of America; what it says is that when an employer who offers health coverage to his or her employees hires someone who qualifies for a Federal subsidy, that employer will be charged a penalty. The amount of the penalty, according to the reconciliation bill, is $3,000 per year. That money doesn't do anything to directly to help cover the employee, it is a tax that goes directly to the government.
In other words, it now costs a "large employer" $3,000 more a year in Federal taxes to hire someone who qualifies for a Federal subsidy than to hire someone who doesn't. This is, of course, what Democrats call rational economic policy.
If nothing else, this makes it understandable as to why House Democrats don't want to have their votes recorded on the substance of the Senate healthcare legislation. But as the fixes in the reconciliation legislation make clear, this is a provision House Democrats want to keep, not one they want to get rid of!
March 12, 2010
Despite Health Care Mess, There are Points of Agreement
Erstwhile Democratic presidential pollsters Pat Caddell (Carter) and Doug Schoen (Clinton) have penned a piece about the political prospects facing their party amidst the health-care drama. Yet, what caught my attention was their concise summary of the things upon which most everyone agrees:
There are enough Republican and Democratic proposals -- such as purchasing insurance across state lines, malpractice reform, incrementally increasing coverage, initiatives to hold down costs, covering preexisting conditions and ensuring portability -- that can win bipartisan support. It is not a question of starting over but of taking the best of both parties and presenting that as representative of what we need to do to achieve meaningful reform. Such a proposal could even become a template for the central agenda items for the American people: jobs and economic development.It's too bad that the Democrats in charge are hell-bent on reconciling this unpopular omnibus health care plan into existence. If they'd take a step back, they'd see that a popular, bi-partisan approach is there for them. But that would mean admitting (a small) defeat.
March 11, 2010
Wanting (and Needing) a Different Kind of Reform
Perhaps it shouldn't be surprising, given the presumption of their label, but "progressives" have a tendency to assume that anybody who wants change wants their kind of change — as if there can only be one solution for reaching a given goal. Just about all conservatives, for example, really do desire world peace, but that doesn't mean they should be counted among those desiring unilateral retreat and disarmament. Most believe that regimes that initiate or foster violence and war must be removed in order for peace to be lasting.
Just so with healthcare. A conundrum that John Kostrzewa cites is not actually a conundrum:
...69 percent of the 200 members of the Greater Providence Chamber of Commerce who completed the survey in February said health insurance was their biggest concern. That's up from 63 percent in a similar survey a year ago. ...But [these results] all run counter to national polls that show a clear majority of people is opposed to President Obama's proposal to overhaul the health-care system by covering more people and eventually cutting costs.
Kostrzewa never quite articulates the factor that resolves the question: It isn't just that individuals and businesses are generally suspicious of Washington and dislike political squabbling (Americans are more savvy than that); it's also that we don't believe that the approach to "reform" that defines Obamacare will improve costs or quality. And that's a problem on up the tiers of government. The state of Rhode Island could go a long way toward alleviating the healthcare concerns of its citizens were it to lighten regulations and let market forces work.
March 9, 2010
Healthcare as Inspiration for Fealty
Further to Monique's post about signs of the wisdom of the Democrats' desired healthcare regime, I thought I'd beat the drum again with Mark Steyn's Saturday column:
... Look at it from the Dems' point of view. You pass Obamacare. You lose the 2010 election, which gives the GOP co-ownership of an awkward couple of years. And you come back in 2012 to find your health-care apparatus is still in place, a fetid behemoth of toxic pustules oozing all over the basement, and, simply through the natural processes of government, already bigger and more expensive and more bureaucratic than it was when you passed it two years earlier. That's a huge prize, and well worth a mid-term timeout.
And well worth some golden-ticket promises to senators and congressmen who may lose their seats over their votes.
Red Flags that the Pending Healthcare Reform May not be a Good Idea
(... in addition to the Constitutional issue - i.e., the legality of compelling everyone to purchase health insurance.)
Much of the disagreement about whether the Democrats' health care reform should proceed centers around its long term consequences. Supporters of the pending reform don't see any problems long range if the bill passes. Opponents point to the inevitable consequences of compelling insurance companies to provide essentially open-ended coverage while demanding that they not raise premiums too high.
Okay, set that aside for a separate discussion. Here are some more immediate warning signs.
1. Congress has exempted itself from it. If better/more expensive health insurance policies are Cadillac plans, Congress has a Rolls Royce. And it stays right in their driveways even if they themselves pass health care reform "for" everyone else. If the proposed reform is such a good idea, why?
2. We start paying for it right away but the benefits don't begin for four years. (Side issue, which it clearly is for proponents: what happens to all of those sick, uninsured people in the meantime?) How viable is a proposed program if the required revenue needs a four year running start?
3. $500 billion cut from Medicare. Proponents have stopped even pretending that this will come from a crack down on waste, fraud and abuse. Setting aside the disgrace and misdirected priority of depriving seniors of this care, isn't a proposed program patently non-viable if another program has to be gutted to fund it?
4. Let's see if we understand the scenario. No insurance company can refuse anyone coverage. The penalty for an individual not obtaining coverage is $800. So wouldn't it be a lot cheaper for the healthy person (many millions of them) to not buy coverage, pay the penalty rather than the premiums year after year and then simply enroll as soon as a health issue crops up? Actually, we don't have to wonder. This is exactly the approach New York took.
New York's "reforms" meant that people could literally wait until they had an accident or illness before buying a policy -- changes that more than doubled insurance costs in the state, according to the Empire State Center for New York State Policy.Premiums shot up so far and fast that healthy customers dropped insurance altogether -- with the number of people buying individual policies plummeting from 750,000 in 1994 to 36,000 now.
It's tough to come to grips with the longer term implications of the proposed reform to health care when we are asked to disregard such serious pitfalls up front.
March 4, 2010
Obama's Health Plan: Rhetoric vs. Reality
The Foundry helpfully breaks down President Obama's latest bid for health care reform:
President Barack Obama gave yet another speech this afternoon urging Congress to pass his health care reform plan.As the President's rhetoric partially indicated, there are legitimate areas of common ground between the President and conservatives. They just aren't in this plan.The President again claimed his plan lowers health care costs. It doesn’t.
The President again claimed his plan would not give government bureaucrats or insurance company bureaucrats more control over health care. It does.
The President again claimed that “if you like your plan, you can keep your plan. If you like your doctor, you can keep your doctor.” That simply is not true.
The President again said his plan gives the American people the same health care as Members of Congress. It doesn’t.
The President again claimed his plan is paid for. It is not.
February 26, 2010
Fundamental Differences Displayed
Heritage's Ed Haislmaier sums up the fundamental issue on display at yesterday's healthcare snoozefest:
The overriding reality behind this summit is that both the public and the politicians come to the table divided not over the details but rather over the basic approach to health reform. In his comments, Sen. Lamar Alexander (R-TN) highlighted three of those major divisions — comprehensive legislation versus incremental legislation, starting over versus pressing ahead with the bills passed in House and Senate in December, and a decentralized approach versus a centralized federal solution. Today’s debate showed few indications of a willingness by the President or the Congressional leadership to alter their basic approach. Though the summit served to highlight the fact that both parties are in favor of reform, differing only in their opinions on how to achieve it, the direction of the health care debate is unlikely to deviate from the course it has taken for the past year as a result of today’s discussion.As the Wall Street Journal reported, the Obama Administration does have a lower cost "Plan B" that would seem more likely to receive bi-partisan support:
The pared-down bill would cost about a quarter of the 10-year, $950 billion plan Obama put on the table on Monday, sources told Fox News.So, the Democrats are still going to use reconciliation to pass an omnibus reform package (and the ProJo editors celebrate!) and face the consequences, if any, in November.The Wall Street Journal first reported Thursday that Obama's staff had prepared the blueprint for a smaller-scale plan. Sources said the backup would extend coverage to about 15 million people, or half the number the larger plan would cover.
It would expand Medicaid and the Children's Health Insurance Program, while allowing people to stay on their parents' health plans until age 26.
But the idea of what one congressional Democrat called "skinny" health care reform may encounter stiff resistance in the House.
"Inaction and incrementalism are simply unacceptable," House Speaker Nancy Pelosi said in remarks released before Thursday's summit. House Democrats are almost sure to reject calls for a scaled-back bill.
"We are going forward with a big bill," a top Democrat told Fox News.
Doctors Point the Way to Reform
It should surprise nobody that I see this as evidence that healthcare reform must move in the free-market direction, not the government takeover and dictation direction:
"Something has been discouraging physicians from working the long hours they used to work," [Douglas Staiger, an economics professor at Dartmouth College] said.
The cause? Bureaucracy and limits to their pay.
Payment issues may have played more of a role. The overall decrease in hours coincided with a 25 percent decline in pay for doctors' services, adjusted for inflation. And when the researchers looked closely at U.S. cities with the lowest and highest doctor fees, they found doctors working shorter hours in the low-fee cities and longer hours in the high-fee cities. ..."There's so much oversight for what we do, so many people we have to answer to and so little of it improves care, it's just driving us all crazy," [Dr. Robert Perlmuter, a Chicago internist,] said.
Officious government meddlers may not believe it, but the rest of us adults can conduct our lives just fine without their assistance. One is hearing murmurs here and there of local officials' wondering whether Rhode Island can move forward with some sort of healthcare reform regardless of what the federal government does. Somehow, though, they've seem disinclined to acknowledge that the General Assembly could eliminate the burdensome mandates right now and immediately improve healthcare quality and costs in the state of Rhode Island.
February 19, 2010
Government Can't Just Dictate Reality
I certainly don't want any of my family's regular expenses going up. Indeed, if I were able to dictate terms to companies who provide me services, I'd lower my rates. But that's not how the world works. Of course, one doesn't get the impression that government officials comprehend such mundane observations of reality.
Rhode Island's Health Insurance Advisory Council, for example, in considering insurers' requests to increase their rates, acknowledges that "most of the proposed increases result from growing hospital and pharmaceutical costs." But the body can only think to posture and demand more squeezing from the companies. Several candidates for public office who put in an appearance at the hearing had nothing additional to offer:
State General Treasurer Frank Caprio, a candidate for governor, offered the council "an update from kitchen tables across the state." He said bills are piling and people are forced to cut back. "I respectfully ask you to say, 'Enough is enough' to these insurers," Caprio said.Lt. Gov. Elizabeth H. Roberts, a candidate for reelection, acknowledged that medical inflation was the underlying problem, but urged Koller to push insurers to develop proposals for dealing with it. "We need to put the challenge on the table," she said.
State Sen. Leonidas P. "Lou" Raptakis, D-Coventry, a candidate for secretary of state, suggested linking health-insurance premiums to the consumer price index.
Why is nobody proposing the clear solution to the problem of increasing in-state health insurance? Look, our mechanism for dictating terms to those who provide us services is to find another provider willing to agree to them. A market of just three insurers is clearly not enough, so we need to bring others in. To do that — and to enable them to keep down costs — we've got to lighten up our mandates and regulations.
Unfortunately, we're learning that the one thing that Rhode Island's ostensible leaders will not consider is decreases to their own authority. That's why we have to apply a political version of the Central Falls high school "turnaround model": Vote them all out of office and reelect no more than the one percent or so who might have something resembling a clue.
January 26, 2010
Hurry to Pass Big Stuff Now and We'll Fix it Later (Promise!)
As I've pointed out, one of the arguments made by the Healthcarism advocates was that we must pass something, anything and "the warts can be removed later." Apparently, that attitude exists amongst global climate changistas, too (h/t):
Some researchers have argued that it is unfair to attack the IPCC too strongly, pointing out that some errors are inevitable in a report as long and technical as the IPCC's round-up of climate science. "Part of the problem could simply be that expectations are too high," said one researcher. "We have been seen as a scientific gold standard and that's hard to live up to."Let's look at what I emphasized:Professor Christopher Field,director of the Department of Global Ecology at the Carnegie Institution in California, who is the new co-chairman of the IPCC working group overseeing the climate impacts report, said the 2007 report had been broadly accurate at the time it was written.
He said: “The 2007 study should be seen as “a snapshot of what was known then. Science is progressive. If something turns out to be wrong we can fix it next time around.” However he confirmed he would be introducing rigorous new review procedures for future reports to ensure errors were kept to a minimum. {emphasis added}
1) "...errors are inevitable in a report as long and technical as the IPCC's round-up of climate science.": Yes, it is a compounding kinda thing: the bigger the report, program, idea, the more likely there will be mistakes, oversights, fraud, waste, abuse....
2) "...the 2007 report had been broadly accurate at the time it was written.": Global Warming? That's soooo 2007. Good thing there was enough resistance to that "consensus" about the inevitability of global catastrophe. If we'd all marched along blindly, can you imagine the sort of already obsolete government regulations and restrictions we'd have had? (Hope I'm not speaking too soon...)
3) "The 2007 study should be seen as “a snapshot of what was known then. Science is progressive. If something turns out to be wrong we can fix it next time around.": There it is. Based on "what we knew then" we were harangued about the need for the massive imposition of "environmental" safeguards that will impact the global economy negatively. And we're assured that things will be fixed next time around--just like health care.
How confident are you that a massive governmental program will be flexible enough to integrate such "change" on the fly? Or that the political will is there to do it. (Social Security, anyone)? No, every time I hear promises about fixing problems down the line, I recall that infamous line from Animal House about trust. My guess, in the wake of the Scott Brown win, is that most Americans are a little wary of Big Government for much the same reason.
January 24, 2010
Protestations to ProJo Pronouncements
1) The ProJo editors on global warming:
Still, that a few scientists are accused of manipulating a bit of data from some climate research does not do away with the preponderance of evidence. The latest controversy revolves around the validity of the collection and use of data behind a U.N. Intergovernmental Panel on Climate Change 2007 report that Himalayan glaciers will shrink dramatically, or even disappear, in a few decades. However, the scientific consensus that Himalayan glaciers will dramatically recede is unlikely to be overturned anytime soon."[A] bit of data", huh? That interpretation explains why the ProJo has ignored Climategate. The attempt to hide data, manipulate data, leave out non-conforming readings from Siberia, etc.? Aw, no big deal. I suppose they're right about that "scientifice consensus" concerning Himalayan glaciers....
The scientist behind the bogus claim in a Nobel Prize-winning UN report that Himalayan glaciers will have melted by 2035 last night admitted it was included purely to put political pressure on world leaders.Oh.Dr Murari Lal also said he was well aware the statement, in the 2007 report by the Intergovernmental Panel on Climate Change (IPCC), did not rest on peer-reviewed scientific research.
2) Froma Harrop is ticked about Massachusetts electing a senator to stop national health care reform, especially since Masachusetts has already enacted state health care reform. (Echoes of the temper tantrum the ProJo editors published a few days ago--guess we know who penned that one!). Harrop thinks the national plan superior to the Mass. one, particularly in that it does a better job containing costs. But Massachusetts is going to fix it, which gets us to Harrop's favorite rejoinder to critics of national health care: "Politically, the Massachusetts program could serve as a national model. Pass universal coverage now, fix it later." Here's an idea: let's revert to the the "laboratory of the states" idea. The reason for the reputed success of national health care programs in other countries rests largely on their relatively smaller populations and cultural homogeneity. Neither of these are comparable in the U.S. So let states handle it, if they choose, like Massachusetts did.
3) Some minor quibbles with Ed Fitzpatrick's piece on what went wrong with Coakley, mostly with his parrotting of two memes that don't have much substance, but apparently make Democrats and liberals feel a little better. First:
Republicans might convince themselves that Brown’s victory heralds a new level of affection for the GOP. But voters aren’t expressing love. They’re expressing anger.No kidding. I really haven't seen many Republicans convinced that they're suddenly the darlings of the polity. Hardly. File under, "I know you are, but what am I...." Second:
But after a year of economic turmoil and seemingly endless debate, many people remain unconvinced that a complex health-care overhaul should top government’s priority list. (If I had to guess, the top three priorities are simple: jobs, jobs, jobs). And now Brown, who as a Boston College law student posed nude for a Cosmopolitan magazine centerfold, has stripped Democrats of any easy way to move forward with the existing bill.It's become an obvious tactic, let's call it Scott Brown Commentary Rule #1: reference his nude modeling "career" no matter what. The attempt is clearly to imply an unseriousness about Brown. Well, sorry, too late. Oh, and one more thing: like all proper thinking columnists, Fitzpatrick is worried that we're headed towards "partisan gridlock.' And that's a bad thing?
January 22, 2010
Move from Management to Insurance to End Payment Disparities
Rhode Island's health insurance commissioner, Christopher Koller, has released a report showing huge disparities in what health insurers pay local hospitals for the very same procedures. The reason is that members of the Care New England hospital group offer services not elsewhere available, so insurers have no choice but to include them, and the hospitals leverage those services for better payments throughout their organizations.
Note the way reporter Felice Freyer insinuates regulation as the strategy for resolution:
Koller’s report shines a flashlight beam into the murky world of hospital finance. Hospitals negotiate privately with insurers to establish how much they will be paid for each service. These talks are largely unregulated, and always private, so that no hospital knows exactly what its neighbor is being paid. All are forbidden by contract to reveal their rates.
Diving into the regulatory pool would only drive up rates. Whether government mandates forced insurers to pay above the rate that the market dictates, within its regulatory strictures, or one or more of the state's three insurers bow out, the cost will ultimately be borne by consumers.
The better approach would be to move away from a system that uses insurance as a healthcare management plan. If patients paid more directly for the services that they receive, the market would set prices based on those services, not on the leverage of hospital groups. That a hospital is the only one with a newborn intensive care unit matters less to an individual who needs heart surgery than it does to a large insurance company that must negotiate a full menu of services.
January 20, 2010
Carter: Kennedy "Killed the [Healthcare] Bill" in 1979
Thanks to a caller to the Matt Allen Show, I was tipped off to something I'd never heard before. In an event at his Presidential Library (broadcast by C-SPAN on September 15, 2009), former President Carter explained that, back in 1979, he had bi-partisan support for a health care reform package that was completely financed and approved by various committees. Well, except for one powerful committee chair who was opposed: Senator Ted Kennedy. That Carter's revelation came just a few weeks after Senator Kennedy's death may explain the dearth of media coverage.
Here is a link to the video (The question and answer begins at around 41:45 of the video and the explanation that Kennedy "killed the bill" is at around 43:30). Here is the relevant snippet as explained by President Carter:
[My health care proposal] would have passed except for---at that time we had the full approval of all of the committee chairman of the House and Senate; Republicans endorsed it with me in a press conference---except for the key Senator and that was Senator Kennedy, who at that moment had decided to run against me for President and didn't want to see us have success. So he killed the bill.Thirty years ago, Senator Kennedy was willing to unilaterally--not even as one of 40 filibusterers, but all by himself--stop health care reform solely for his own political benefit. Legacy indeed.
UPDATED: Here's a brief, contemporary story from the Harvard Crimson about the plan. CNN covered the speech last September, but reported the above as follows:
Carter blamed "political problems" for his inability to overhaul the nation's health care system in 1979 so that all 15 million Americans then without health insurance would have gotten coverage. That number has tripled in the intervening years.One is left to infer that the problems must have been partisan based (ie; the GOP must have stopped him), just like they are now. And they wonder why they have the reputation they have. Finally, according to the Wikipedia entry on Jimmy Carter, similar accusations by Carter against Kennedy can be found in Carter's book Keeping Faith (pp. 86–87).
January 19, 2010
ProJo's Last Shot at Brown - Scare Tactics
On election day in Massachusetts, the desperate ProJo editors have resorted to listing a bunch of "what ifs?" should Scott Brown be elected and Obamacare not pass. Notwithstanding that a counter-argument can be made that passing this particular monstrosity called health care "reform" would make all of the items they identify even worse, the panicked essay reveals that the fatal flaw in their reasoning still exists. They clung so stubbornly to a mythical, ideal single-payer system--like Medicare for all!--that they've been blind to other (yes, free market) reforms that would accomplish many of their desired goals, if differently. So they're left to exclaim that we need to pass something, anything ("the warts can be removed later") before it's too late.
January 14, 2010
The Haves and Don't Have Tos of Healthcare
Mark Patinkin begins a brief examination of "why there's all this fuss about revamping the [healthcare] system" with a faulty premise:
I'm guessing there have been two distinct audiences for the health-care debate.Those who have an affordable plan and those who don't.
If you don't, you doubtless paid a lot more attention.
Patinkin's essay stands as evidence that there are at least three audiences, and since the third implies an antipode, there must be four:
- Those who have an affordable plan and believe something like the Democrats' plan will not affect them.
- Those who have an affordable plan and believe something like the Democrats' plan will threaten them.
- Those who don't have an affordable plan and believe something like the Democrats' plan will ensure one.
- Those who don't have an affordable plan and don't believe something like the Democrats' plan will ensure one.
So dramatically different is my understanding of the landscape than Patinkin's that he assumes the "don't haves" to be the most interested in the debate, while I've perceived the debate mainly to be between the factions of the "haves." Note that the Tea Party phenomenon was heavily populated by working and middle class folks, and that much of the advocacy for the Democrats' policies has come from Patinkin's peers in the media, academia, and government, all likely having excellent benefits.
A telling bit of the perspective difference between the "have" groups comes when Patinkin investigates the options that "have nots" can pursue. Just after explaining to his readers how a deductible and copay would work on a $2,000 MRI, he writes:
I was told you might be able to get that $660 monthly fee down to $487 if you proved you were very healthy. But you'd still have the deductible, leaving folks to debate every procedure.
Here's my question in response, as somebody who has decent (although too expensive) coverage and fears that the Democrats are on track to price me out of it: What is wrong with folks debating every $2,000+ procedure? Simply put, there will never, ever be an effective mechanism for controlling healthcare costs unless every potential patient weighs the value of every test, drug, and procedure. Pretending otherwise is going to cause a whole lot of suffering among a whole lot of people.
Labor Gets its Special Health Care Deal
At the end of this post I alluded to the special deal that unions--after much b***ing and moaning-- have extracted from Team Obama Health Care Force. In short, the tax on so-called "cadillac plans" won't be applied to collectively bargained health plans. Heritage's James Sherk observes:
What a deal. Unions want the health care spending, but they do not want to pay for it. Obama gave them just that. It also makes for a great recruiting pitch: join a union, get a tax cut.No doubt. But wait, there's more!
That is just one of the many handouts unions get in the health care bill. It sets aside $5 billion to subsidize the costs of employer health benefits for early retirees. Few nonunion employers, of course, pay pension and health benefits for workers to retire at 55.Nothing like looking out for the little guy, eh? But back to the exemption: Daniel Foster looks at the tea leaves:Or consider the small business exemption from the employer mandate for businesses with less than 50 employees. All businesses, that is, except construction companies. The costly employer mandate applies to any construction firm with more than four workers. Why would Congress kick small construction contractors when they are down? Because the construction unions asked Congress to. They did not want their small competitors to get out from under the bill’s costs and gain a competitive advantage. What if those costs put small contractors out of business? That is just too bad.
Look for Obama and Congressional Democrats to the expand the union carve-out to cover a swath of the "middle-class" (the universal solvent of American politics), so they can camouflage this massive giveaway to a pet constituency.The shell game continues.One House Democrat is already saying a "consensus" could be built around such a scheme by further increasing the Medicare payroll tax and applying it to capital gains to make up for lost revenue.
This would amount to nothing less than a bill of attainder against on all constituencies that are not especially useful to the president and his party.
January 13, 2010
ProJo Ideology Identified: Healthcarism
With the ProJo editorial board's endorsement of Martha Coakley for Senate, it's become more apparent than ever that the ProJo editorial board has become a single-issue shill for health care reform at all costs.
Most important to us is that she is the candidate most likely to carry on the work of the late Sen. Edward Kennedy in health-care reform.This really isn't a surprise. In October, after the death of the late Senator Kennedy, the editorial board gnashed their teeth over the "contortions" that Massachusetts Democrats went through to enable Governor Duval Patrick to select a seat-warmer, but legitimized it to themselves:
Mr. Kirk’s immediate duty will be to ensure that the Democrats keep 60 votes in the Senate so they can push through major legislation, especially on health care. That is why Massachusetts’s Democratic leadership went through contortions to change the law to get their man in there. We’d be happy to see health reform pass with his help, of course.Yeah, it kinda stunk, you see, but the ends justify the means. Just so.
Over the past few months, we've witnessed them twist and turn with every permutation of the various, nebulous health care reform bills that weaved through Congress. First, while they didn't necessarily like the Baucus bill (preferring a single-payer system), they urged Democrats to be ready to go it alone because "[t]he stakes are too high to let political wrangling stop Congress from addressing the many flaws of our chaotic health-care 'system.'” In October, they did accurately portray the opponents of this nebulous version of health care reform at one time:
One is the principled conservative, or at least libertarian, view that the less government role in health care the better. Another is just old-fashioned bribery, in which some legislators take care of health-insurance and pharmaceutical companies, which pay vast campaign contributions and thrive from the current arrangements. And another is the worry among Republicans that the Democrats might get long-term credit for health-care reform, as with Social Security and Medicare –– two other very popular “socialistic” plots opposed by much of the GOP when they were started....Yet, setting aside the disingenuous implication that the opponents breakdown equally into these three groups, the ProJo's subsequent editorials have focused on the two worst factions--the hypocritical Republicans who previously supported the Bush-era Medicare hike (which many, many conservatives opposed) and the insurance company water-carriers. The arguments that principled conservatives have made for alternative plans remain unaddressed. Instead, the ProJo editors lump good-faith opposition together with the so-called hypocrites and bribe-takers. For example, they complained that "the public option was forced out of the legislation by Connecticut’s Joe Lieberman, an 'independent' who is quite dependent on insurance-industry contributions." Big insurance bad. Big government good!Of course as often is the case in the sausage-making of legislation, the public’s memory of the hypocrisies involved is dim — for instance, that while many Republicans now in Congress voted for President Bush’s $1 trillion Medicare drug plan (which had no stated way of paying for itself and was a grandiose gift to the drug companies), they now oppose plans that would offer close to universal health coverage to non-elderly Americans –– including kids and poor working adults, of all people.
Now, even as their dreams have come true and a purely partisan bill has passed the Senate and moved into conference (or whatever the House and Senate Dems are doing behind closed doors), the ProJo editors are trying to have their cake and eat it too. They've argued for the passage of anything, explaining that "the warts can be removed later" and, as an example, recently urged the Democrats to remove the special deal cut by Nebraska Senator Bill Nelson that would exempt his state from any health reform related tax hikes. Fine and dandy. Now we await the editorials on the numerous other deals cut by Senators and other interest groups that enabled the passage of this health care "reform" that the ProJo editorial board has pushed at all costs. Right.
For now, they seem content to blame the majority of the public that opposes this mess for our "vast willful...ignorance of what’s actually in the House and Senate health-care bills." Silly us. And here we thought we were opposing a pastiche of bloated government power-grabbing and special deals masquerading as health care reform. I, for one, am all for reform. But this ain't it and calling it such doesn't make it so, no matter what the ProJo editors want us to believe.
ADDENDUM: It's being reported (h/t) that the leaders of organized labor have twisted enough arms to get an exemption for "collectively bargained health care plans" that would otherwise be considered "cadillac plans" and thus subject to taxation that would help pay for the current health care reform proposal. I wonder if the Providence Journal will draft an editorial against this "wart", too? It seems like creating a billion dollar program that everyone supposedly wants requires an awful lot of sausage making.
January 12, 2010
If You Don't See It, You Don't Feel It
For those who remember when health insurance used to be only "hospital insurance" or "catastrophic", this chart shouldn't be a surprise.

Veronique de Rugy puts it in context:
Much of the rationale behind the current reform of the healthcare system is about controlling inflation in healthcare costs. However, based on the trend presented above, a better alternative to the semi-nationalization that the president has in mind would be to increase individual responsibility for medical decisions and costs. When people aren’t exposed to the true cost of their care—even if they pay for it in foregone wages and higher taxes—they consume more.
January 11, 2010
It's Our Habits, Not Our Healthcare
Redington Jahncke explains why "skepticism turned out to be the correct impulse in the case of the WHO rankings" of nations' healthcare systems, as well as in the case of a Commonwealth Fund study of the "health of nations." It's his conclusion, though, that points toward a new question about Obamacare:
Indeed, lifestyle and behavioral factors, including unhealthy diet, lack of exercise, smoking, etc., are the prime causes of America's number one killer — heart disease. And the reversal of these factors is as important in preventing death from heart disease as any medical treatment. A doctor cannot "administer" lifestyle changes and behavior modification the way he can administer drugs.
Let's put aside, if we can, the probability that the Democrats' healthcare plan, whatever it ultimately turns out to be, will drive costs up even more while decreasing the effectiveness of the healthcare system overall. If we concede that lifestyle and behavior are critical contributors to health — and how can we not concede it? — then what sort of system would be more likely to encourage healthy behavior: A system that requires financially painful, but not physically fatal, treatments and procedures, or one that hides their costs in a combination of employer withholdings and welfare?
A more frightening question: How will the government seek to make you live more healthily when it turns its giant eye toward that problem?
January 6, 2010
Whitehouse Gets Things Backwards
Of all the letters that have appeared decrying or endorsing Senator Sheldon Whitehouse's recent screed against those who oppose Obamacare, one by Pamela Burdon, of Warwick, was especially poignant:
The Nazis took my parents from their families when they were teenagers. My parents miraculously survived under impossible conditions. They then fled communism, coming here to become American citizens and work their hardest to provide for their children.They were so proud to be Americans that they would rarely speak the many European languages they knew. ...
As a way of honoring their memory, I feel it is my responsibility to preserve the freedoms that they valued so highly. Can I sit idly by and let their America be destroyed? Could I live with the knowledge that they sacrificed everything to come here, for a better life for their future generations, only to let hastily passed legislation eventually turn this country into a replica of the ones they fled?
January 5, 2010
Rights and Benefits
As Monique insisted, last night, healthcare is not an "inalienable right." Because it requires other people (doctors, et al.) to provide services, it is actually a consumer good. It's a vital one, to be sure, and one for which people will exchange significant percentages of their resources, but that doesn't make it a right.
It does, however, make it an attractive target for people who would like to control your life, such as the current collection of Democrats and their armies of government bureaucrats, who believe doing so to be their right. The ideological distortion of the nature of healthcare serves no purpose but to disguise the fact that government cannot provide this "right" at a lower cost than people can procure it for themselves. If the Democrats' motivation were otherwise, their solution would exclude all of the interference and fluff and provide for the government to grant healthcare to those who want it but can't afford it, and deliberations would consist of a debate about what aspects of "healthcare" are rights, and which are extra. Instead, the objective of legislation has clearly been to determine who controls the industry and how.
Recasting the structure of healthcare "reform" with the assumption that healthcare is a right shows the notion to be nonsense. What other "right" do we require citizens to purchase? What other right requires that people provide the services and that employers offer access to those services as a benefit? Again, rights aren't the sort of things subject to determination of cost effectiveness.
Ezra Klein makes a related point when he suggests that "health-care coverage is not a benefit. It's a wage deduction":
Cost control is not, in fact, all pain and no gain. It's some pain in return for a fat raise. A 2006 study, for instance, by Harvard's Katherine Baicker and Amitabh Chandra used malpractice payments to estimate the effect of premium increases on wages. They found that a 10 percent increase in health-care premiums "results in an offsetting decrease in wages of 2.3 percent" and an increase in unemployment of 1.2 percentage points. Compensation is basically a set sum for employers, and they don't seem to care much whether it goes into wages or into health-care costs.
Assessments of value exist all along the healthcare service chain. Doctors become doctors because the career presents an opportunity to earn the standard of living that they desire through an occupation in which they have an interest. Employers provide health insurance because it helps them to attract and retain employees more effectively than simple cash remuneration. Heretofore, as with all benefits, workers could presume the exchange to be worthwhile; they were giving up part of their natural pay in order to gain something that would cost them more were they to pay for it individually. If one spouse's employer provides better value, the couple switches. If the employee is healthy, he or she opts to take the money instead. The legislation on track to become law merely layers on disguises that enable citizens to ignore the fact that healthcare has a cost.
Back to Klein:
When Americans rejected managed care [such as HMOs], in other words, they didn't know they were ending wage increases, too. But since 1990, wages have tracked changes in premiums more closely than they've tracked the growth of GDP. Maybe if more workers knew that, they would be more interested in efforts to control health-care costs.
Anybody who has watched unions negotiate their contracts can appreciate the point. They'll give up wage increases if their negotiators believe that health insurance benefits will ultimately result in a greater transfer of wealth, and vice versa. What legislators who profess the healthcare-as-a-right doctrine are effectively doing is declaring that somebody must pick up the bill for extensive coverage without reference to the exchange in wages or economic activity or whatever else the burden will land on. And because those ultimately paying the cost won't know the dollar amount (indeed, they probably won't realize they are paying it at all), the bill can only increase.
Personally, I see it as more appropriate to insist that we have a right not to pay more for a service than we are willing to pay for it.
December 31, 2009
A Commission (a "Panel," if You Will)... That's the Ticket!
Thomas Sowell puts it pretty starkly:
The appointment of White House "czars" to make policy across a wide spectrum of issues — unknown people who get around the Constitution's requirement of Senate confirmation for cabinet members — is yet another sign of the mindset that sees the fundamental laws and values of this country as just something to get around, in order to impose the will of an arrogant elite.
The problem is that it isn't just the political elite who lack a sufficient understanding of the real value of democratic processes. Sowell blames "dumbed-down education in schools and colleges that have become indoctrination centers for the visions of the Left," although the reference to political direction might obscure the essence of the poorly formed vision — namely, that it is possible for people to figure out and design broad social programs that will improve life for all if they're only given the power to implement them. And so, we get this disappointing, but not surprising, editorial from the Providence Journal:
Neither Congress nor the Obama administration (nor that of George W. Bush) has shown the gumption to act honestly to confront these costs. Perhaps commissions will give them adequate cover to take on the "special-interest groups." (We're all de-facto members of several such groups; one man's pork is another man's national treasure.) ...So a bipartisan congressional committee should pick the members of these commissions and give them as much power as possible. Such panels would probably feel compelled to recommend higher taxes and sharp cuts in some programs.
In the Projo's telling, such a plan is all up-side: giving an unelected panel as much power as possible (to break some eggs) with adequate immunity to push elected representatives to do that which the public does not want. That attitude is a recipe for totalitarianism and a collapsed nation, but it's frighteningly pervasive. Everybody, after all, has a vision that would clearly work... if only it could be forced on the nation.
As if to prove its own incoherence, the editorial shifts gears to complaints that people are heeding ideological sympathizers whom they trust to specialize in sensing political winds, rather than giving rein to Congressional "staffers specializing in the subject at hand" as they craft complex legislation. The essay ends thus:
Representative democracy is a terrible system, but, as Churchill noted, better than all the others.
One might get the erroneous impression that the editorial writers are supporters of representative democracy, even after they'd spent a few hundred words advocating for rule by unelected groups and behind the scenes staff experts.
December 29, 2009
A Refreshingly Different Projo Voice on Healthcare Reform
I'm going to go out on a limb and speculate that it's not Edward Achorn who's been the primary author of the Projo's recent series editorials on healthcare reform.
The position of the Projo editorial board has been pass anything, it doesn't matter if the legislation has been read or not, so long as it means that the government will be on the path to more control of the healthcare system.
Achorn's position is a bit more nuanced…
It is not an act of Aryan supremacy to wonder what part of the Constitution empowers Congress to compel people by threat of jail or fines to buy very expensive products — in this case, health insurance — produced by private companies with influential Washington lobbyists.It does not make one a “birther” to question how the struggling middle class will afford all this — the vast new government entitlement in the teeth of massive deficits, the huge tax hikes to pay for some of it, and the mandates for expensive insurance.
One need not be a member of a right-wing militia to feel suspicious when a law that will affect every American is crafted behind closed doors, larded up with bribes to politicians, and rushed through the Senate in a series of votes in the dead of night, capped by one on Christmas Eve, when any reasonably sane citizen is distracted from guarding the national cookie jar.
December 28, 2009
The Members' Interests Are Not Primary
Mike, of Assigned Reading, noticed a strange omission of activism on the part of his and other teachers' unions:
Teachers enjoy some of the best benefits available. And as a result, we working class Americans will be subjected to a 40% premium tax, a punishment for having healthcare plans better than most Americans.One would think the teachers’ unions in particular would be loud and vocal in their opposition. This would be true if the teachers’ unions were most interested in teachers. But when push comes to shove, the unions will put down their arms if it helps secure a victory for the Democrats.
I wonder if union organizers ever get heat from their members for activism that is either unrelated to or actually hostile toward their interests. The impression, from outside, is that there's a sort of compromise between teachers unions and teachers, such that the former pull all kinds of stunts and compromise the quality of education in order to provide ensure incessant growth for the remuneration of the latter, who pay dues more as a fee for service than as a cost of entry. In other words, the union gets to do whatever it wants, because it's really an independent organization from the workers whom it supports.
Somehow, I don't think it's supposed to work that way.

Roland Benjamin: Health Care Calculations
For those following the health care debate, this will come as little surprise. Linking the massive reform bill to practical, everyday application has largely been ignored by our lawmakers.
A recent non-partisan poll indicated that 91% of Americans with existing health coverage are at least somewhat satisfied with that coverage. The bill being debated in Washington does nothing to protect this.
Despite my business's currently competitive benefit package, the bill would penalize LFI, Inc., $750 per employee as the plan's design does not meet the new law's universal standard . The resulting choices would then be a) pay an approximately $53,000 fine/tax while paying $400,000 for the current plan structure, b) increase the current plan structure by $70,000 to $470,000 and avoid the fine, or c) discontinue offering health benefits and pay the $53,000 fine toward subsidies helping lower-income employees offset premiums they will be required by law to pay.
Thus, there is enormous pressure on employers to drop coverage. This is especially true when businesses pay into the subsidy pool regardless of whether they offer a health plan. These fines take effect in 2014, so preparations can be made. Some fines start sooner. The likelihood that LFI discontinues health benefits in 2014 is moderate, with hundreds of variables still unidentified.
Individuals will be required to buy a federal and state authorized plan. Consumer-directed plans enabling lower premiums will be dramatically restricted. By 2014, premiums for an authorized family plan will exceed $17,000 per year. Some will receive subsidies, but current language requires that individuals pay around 10% of household income toward their health plans (e.g., a two earner household with $70,000 in combined income will have to pay at least $7,000 in premiums before applying for federal subsidies). These subsidies phase out in households with combined earnings around $85,000. Anyone in that category will be required to pay the full premium. Additionally, because United Health and Tufts do not offer individual plans, most would have to buy a plan from Blue Cross Blue Shield under current regulations. This might change should a robust "exchange" emerge in the state. But it might not.
For employers, the reform offers an immediate and plausible exit option. Health care is one of the least controllable expenses we face and entails an immensely time-consuming process. I am forced to make decisions that must satisfy more than 50 families each year and explain to each why more dollars are diverted from their compensation toward unnaturally inflating health costs. This is not fun.
Once this law is enacted, annual renewals will see increasing pressure to drop coverage. Should reform perform some unintended miracle in trimming health care inflation, that pressure might ease. But the objective of the law is to expand coverage to the uninsured, not to tame the inflation in health care spending. Health care experts and economists around the country, including Rhode Island's own experts in a recent ProJo analysis, confirm that "Obamacare" does nothing to affect health care inflation. Within a few years, employer-provided coverage will erode until it is no longer a competitive advantage in the marketplace for new employees.
The decision to drop coverage would not be made lightly. But I would rather take the $400,000 now paid toward health premiums and divert some to employees while reinvesting the remainder in the business, knowing that those who need the most help will have a federal subsidy to buy coverage.
As an American, I am incensed by this, though. Today, the premium paid for by your employer is earned as part of your compensation. When forced to beg for a subsidy to offset health premiums, that sense of earning diminishes, and the independent spirit erodes with it. They are replaced with an unhealthy combination of entitlement and dependency that threatens the American experience.
Never in human history have the freedoms envisioned by our Founding Fathers been realized by so many. They recognized that liberty, having been endowed by our creator, could only be taken away by man and government, not enhanced. This unique American Experiment has enabled the broadest prosperity across an entire population ever known to mankind. And we have dragged the rest of the world forward with our innovations and generosities. Health care reform in its current state has the potential end this.
To prepare, pay close attention to your Health Savings Account. Should your employer discontinue health benefits after 2014, money in an HSA will be critical. Those dollars may be used to pay premiums and also may determine which plans you will be allowed to purchase by law. In other words, the greater the balance in your HSA, the more flexibility you will have.
There is still the possibility that this reform will be derailed. It faces several procedural hurdles. A Senate vote to advance the bill by Christmas was a political necessity for the Democrats, but the bill is extremely unpopular, with a significant majority of voters opposing it. Democrats want the bill out of the news as soon as possible. They hope the memories of the voting public are short. Republicans, with only 40 elected members in the Senate, do not have the numbers needed to continue the debate to make this reform right. Democrats, needing 60 Senators in lockstep, voted unanimously twice to cut off debate in order to meet the arbitrary Christmas deadline and then passed the bill with the same margin. Not a single Republican voted to end the debate or to pass the bill.
To get these 60 liberal Senators in line, the bill includes hundreds of millions of dollars to states like Louisiana, Connecticut, Vermont, Florida, Pennsylvania, and Nebraska. Because our Senators "drank the Kool-Aid" long ago, Rhode Island gets no "bacon" from Washington. Instead, we get Senator Whitehouse accusing concerned citizens of bigotry! The intellectual vacuum of his argument is an embarrassment to Rhode Islanders.
This health care bill is tyranny and is unconstitutional. Whitehouse showed quite clearly that liberals have lost the intellectual debate and resorted to slinging mud at the majority of Rhode Islanders uncomfortable with the bill. Pressure from everywhere can stop this reform. But it has the momentum to pass if nothing is done.
December 26, 2009
To Better Deceive the People: Hurry Up and Wait
All revved up for negotiations to reconcile the House and Senate versions of economically destructive health "reform"? Well, you're going to have to wait over a month, until after some soaring rhetoric from the Deceiver in Chief:
The White House privately anticipates health care talks to slip into February — past President Barack Obama's first State of the Union address — and then plans to make a "very hard pivot" to a new jobs bill, according to senior administration officials.Obama has been told that disputes over abortion and the tight schedule are highly likely to delay a final deal, a blow to the president, who had hoped to trumpet a health care victory in his big speech to the nation. But he has also been told that House Democratic leaders seem inclined, at least for now, to largely accept the compromise worked out in the Senate, virtually ensuring he will eventually get a deal.
Internally, White House aides are plunging into a 2010 plan calling for an early focus on creating jobs, especially in the energy sector, along with starting a conversation about deficit reduction measures, the administration officials said.
In other words, the propagandists are going to give the United States a break from the masochistic legislative beating that the Democrats have been inflicting on voters, settle down for a few quiet winter weeks to see if Americans will (per habit) lull themselves back into apathetic slumber. Then, the president will play his preacher-like oratorical cards with a state of the union address once again promising the giveaways and fantasy improvements of healthcare and energy legislation that is, although he'll pretend otherwise, still pending and declaring it to be (guessing) "time to move past the divisiveness of the past and do the work that Americans so desperately need done."
Then, in his usual practice, Obama will make vague promises about jobs legislation... that he'll leave entirely up to legislators to define, so as to keep his hands abstractly clean... and try to paint Republicans as obstructionist when they point out that the Democrats are merely proposing to give more (unborn) taxpayer dollars to their political supporters. The only employment legislation that might have a chance of working would have to move in entirely the opposite direction from that in which the Democrats are marching on every single issue in their agenda.
Whether the political choreography will work is another matter. It would certainly be characteristic of Americans to long for some political hibernation, but media cheer leading notwithstanding, the economy is likely to remain stagnant, or worse, and people in pain are less able to drift into sleep. Moreover, a year's experience watching the centrist uniter and his party turn Washington, D.C., into an even more hyper-partisan, money-grubbing, backroom-dealing swamp of oligarchical vampirism should prove to have inoculated a sizable portion of those who've been fooled by the rhetoric before.
December 24, 2009
Mugged on Christmas Eve
Of all the aspects of the healthcare debate and legislation that are rightly making Americans shake their heads, I think the schedule is the most egregious and representative. Think about it: The major votes have all been held over the weekend, and the final vote came on the morning before Christmas.
The profundity of that struck me as I drove in to work this morning. No school buses. Light traffic. And massive legislation being voted on — and passed — in the Senate.
This is criminal "leadership," and I don't just mean the new taxes and other ways in which Congress is trying to rob the people whom it's meant to represent. This is a real taste of what citizenship is like in nations that have tipped toward one of those discomfiting descriptions, such as totalitarianism and oligarchy.
The Democrats think they've gotten over the threshold and now can enter a phase of recovery before the next election cycle rolls around. I think they're dramatically overestimating the chances that Americans will treat this matter with their habitual delayed apathy and forget about it. It's too much. Too dumb. Too sneaky. And if we let this go, we might as well get fitted for shackles.
December 23, 2009
What Obamacare Does to the Middle Class Budget
Terry Jeffrey helpfully boils down a key portion of the Congressional Budget Office's take on the Senate health care bill: how it would affect an average middle-class family's bottom line. How does another $15,000 in "fees" (or, taxes if you want to call 'em that!) sound? Here's a summary of his summary
Fact 1: You will be forced to buy health insurance...Such a deal!Fact 2: You will be eligible for a federal subsidy to help you buy health insurance, but only if you earn less than 400 percent of the poverty level ($88,200 for a family of four), your employer does not offer you coverage and you purchase a government-approved plan in a government-regulated insurance exchange...
Fact 3: Your employer will not be required to offer you coverage, and will face a maximum fine of $750 per worker per year if it does not...
Fact 4: Your insurance provider will face new federal mandates that will increase its cost for any plan it offers you...
Fact 5: Your family insurance plan -- if your employer drops your coverage and you are forced to buy it on your own -- will cost about $15,000 per year when the legislation is in full force in 2016...
The Senate health care bill gives employers two powerful incentives to stop offering health insurance coverage to their workers. First, if an employer does offer coverage, its lower-wage workers will lose the federal insurance subsidy they would otherwise get. Secondly, if an employer does not offer coverage, the $750-per-worker fine it faces will be far less than the premiums it would pay if it did offer coverage.
Where does this leave a mom and dad with two children and an annual income greater than $88,200? It leaves them without employer-based health insurance and facing a federally mandated $15,000-per-year insurance bill.
December 22, 2009

Are key portions of Obamacare going to be unrepealable?
It is worthwhile to listen to Senator Jim DeMint discuss one critical aspect of the Senate Obamacare bill:
Sen. Jim DeMint (R., S.C.) has thumbed through Harry Reid's manager's amendment and discovered some "particularly troubling" rule-change provisions, especially with regards to the proposed Independent Medicare Advisory Board, which he finds could be unrepealable
John McCormack:
According to page 1001 of the Reid bill, the purpose of the Independent Medical Advisory Board is to "reduce the per capita rate of growth in Medicare spending." For any fearmongers out there tempted to call an unelected body that recommends Medicare cuts a "Death Panel," let me be clear. According to page 1004, IMAB proposals "shall not include any recommendation to ration health care"—you know, just like the bill says there's no funding for abortion.
William Kristol:
Why did the authors of the legislation want to specially protect the Independent Medicare Advisory Board by making it difficult for future Congresses to legislate in that area? Because the heart of the bill is the attempt to get control of our health care permanently in the hands of federal bureaucrats, who would allegedly know better than doctors and patients what’s good for them, and who would cut access to care and the quality of care...
A GOP Senate staffer writes:
The bill changes some Senate rules to say we can't vote in a future Congress to repeal the IMAB (death panels)....It also shows that this provision in particular is very important to Dems. They chose this section out of all others to give the highest possible protection against change or repeal showing how insatiable their desire is to allow Washington bureaucrats to control our lives.
And for these sorts of issues, it is critically important to force a vote on Christmas Eve before the word can get out about the true nature of the bill.
Meanwhile, the Republicans are not articulating a compelling strategic alternative to draw American citizens into their realm.
It's too bad we can't send everyone home from Washington, D.C. until the 2010 elections.
Quinnipiac Poll on Healthcare
Quinnipiac University has released a poll today reporting a national level of opposition to Democratic healthcare reform consistent with the Rasmussen results released yesterday (h/t Instapundit)...
As the Senate prepares to vote on health care reform, American voters "mostly disapprove" of the plan 53 - 36 percent and disapprove 56 - 38 percent of President Barack Obama's handling of the health care issue, according to a Quinnipiac University poll released today.Voters also oppose 72 - 23 percent using any public money in the health care overhaul to pay for abortions, the independent Quinnipiac (KWIN-uh-pe-ack) University poll finds.
December 21, 2009
Full Text of Senator Whitehouse's Healthcare Speech
Senator Sheldon Whitehouse’s floor speech on healthcare from Sunday has been receiving national blogospheric attention since the quote below, broadcast on C-SPAN, was picked up by the Washington Times...
Why all this discord and discourtesy, all this unprecedented, destructive action? All to break the momentum of our new, young President. They are desperate to break this President. They have ardent supporters who are nearly hysterical at the very election of President Barack Obama: the ``birthers,'' the fanatics, the people running around in rightwing militias and Aryan support groups. It is unbearable to them that President Barack Obama should exist. That is one powerful reason.The full text of the speech, taken directly from the Congressional Record, is posted below the fold.
I believe that the “they” referred to by Senator Whitehouse are Senate Republicans, meaning that the Senator is not saying that all opponents of healthcare reform are birthers, fanatics, and/or rightwing militiamen (and militiawomen) -- only that support from birthers, fanatics, and rightwing militiamen (and militiawomen) is significant enough to merit mention in the assessment of Senate Republican motives.
Of course, opposition to the Democratic Party's plans for building healthcare reform around an employment-based system that's liked by no one -- except for, apparently, Congressional Democrats and insurance companies -- is very widespread...
The latest Rasmussen Reports weekly tracking update shows that 41% of voters nationwide favor the bill and 55% are opposed. Those figures are essentially unchanged from a week ago. This the fifth straight week with support for the legislation between 38% and 41%....Most voters (54%) believe they personally will be worse off if the legislation passes....so if the Senator stands by his position that birthers, fanatics, and/or rightwing militiamen (and militiawomen) form a significant base of opposition to Democratic health "reform", will he let us know how much of the 55% of the population reported by Rasmussen to be skeptical of the current "reform" plan he believes to be members of extremist factions?
Or is expressing opposition to the Democratic party's belief that everything can be improved by higher taxes and more government control now enough, by itself, to make you a fanatic?
ADDENDUM:
The Washington Post's Dana Milbank picks up on a couple of historical references that I had passed over (full text of the speech below the fold, if you don't believe that they're all there)...
Sen. Sheldon Whitehouse (R.I.) had just delivered an overwrought jeremiad comparing the Republicans to Nazis on Kristallnacht, lynch mobs of the South, and bloodthirsty crowds of the French Revolution.Asking for a bill to be read and deliberated before being voted on is on par with racial lynchings, anti-Jewish pogroms and the guillotine?"Too many colleagues are embarked on a desperate, no-holds-barred mission of propaganda, obstruction and fear," he said. "History cautions us of the excesses to which these malignant, vindictive passions can ultimately lead. Tumbrils have rolled through taunting crowds. Broken glass has sparkled in darkened streets. Strange fruit has hung from southern trees." Assuming the role of Old Testament prophet, Whitehouse promised a "day of judgment" and a "day of reckoning" for Republicans.
Continue reading "Full Text of Senator Whitehouse's Healthcare Speech"
December 20, 2009
What Government Healthcare Really Means
Well, this about sums it up:
Far from being a brilliant plan constructed by top doctors and financial experts in a government brain trust, this health-care bill is a twisted, deformed political document, seen in its entirety by only a few high-ranking politicians belonging to a single political party. Its components have not been precisely crafted as part of a fantastic system calibrated to ensure the maximum access to quality health care for all Americans.The bill is not being examined with transparency and careful deliberation by representatives who behave as humble servants of the people and their Constitution. Instead, it's being hastily rammed through in the dead of night, over the objection of powerful majorities of the American people, with desperate last-minute deals cut to acquire the necessary votes, financed by vast sums of taxpayer money. The primary consideration is not crafting the most sophisticated and intelligent health care reform... it's getting a bill pushed through before angry voters have a chance to blast the Democrats out of Congress. Look at it this way: if the average middle-class American paid about $5000 in federal income tax last year, then you might be one of the 20,000 people who paid for Mary Landrieu's vote, in the hope of giving Barack Obama a bill to sign as a Christmas present.
November 29, 2009
Speaking of Healthcare...
Here's another result found in Rasmussen's polling:
Forty-nine percent (49%) of voters nationwide now rate the U.S. health care system as good or excellent. That marks a steady increase from 44% at the beginning of October, 35% in May and 29% a year-and-a-half ago.The latest Rasmussen Reports national telephone survey finds that just 27% now say the U.S. health care system is poor.
I suppose as people go through the compare and contrast process, they become increasingly wary of results like this across the pond:
The key findings of the report were:- appalling hygiene and cleanliness in A&E
- patients left in A&E for ten hours and treated in full view of others
- four deaths among patients with learning disabilties
- a lack of children's nurses and doctors in A&E
- blood splattered on curtains and mould in vital equipment
- lack of basic nursing skills with failure to feed patients or give medication correctly
- elderly patients frequently developing bed sores, prompting concerns from nearby care homes.
Maybe it's time for the newspapers to run some more of those nice letters from doctors in Canada who just happen to think it worth their while to let far away opinion page editors know how great their system is.
With Time, the Truth About Healthcare Is Coming Out
So, according to Rasmussen, public opinion on the Democrats' healthcare plan is currently at 38% for, 56% against. The specifics are even less positive:
Only 16% now believe passage of the plan will lead to lower health care costs. Nearly four times as many (60%) believe the plan will increase health care costs. Most (54%) also believe passage of the plan will hurt the quality of care.
One wonders how much of an effect it has had that, as the longevity of the debate carries it over Americans' great wall of apathy, people are catching on to the oft-repeated falsehoods such as Ramesh Ponnuru addressed in a recent National Review article:
Earlier this year, Ceci Connolly reported, in another front-page story for the Washington Post, that people who go without health insurance raise premiums for the rest of us by $1,000 a year. Supporters of universal coverage routinely invoke this factoid. It's not a fact. The source is a left-wing advocacy group, and nonpartisan observers, including the CBO, believe that the real premium increase is much smaller, perhaps $220 a year.In the same piece, Connolly reported that the U.S. spends more money on health care than other countries while generating less impressive statistics. She specifically cited our high infant-mortality rate--without mentioning that we have, for example, a higher proportion of low-birthweight babies than other countries, which is hardly the fault of our system of health finance.
Maybe Connolly's worst blunder was to report that there is a "consensus" that the cost of health care undermines the competitiveness of American business. That consensus includes other news outlets, such as Reuters, and President Obama. There is a directly opposed consensus that includes most health-care economists, the CBO, and some members of Obama's economic team. It holds that health-care costs come out of wages, not profits, and thus generally do not affect firms' competitiveness.
The mainstream media, by the way, is in a tough spot. If they continue with their current practices, many of its practitioners will be entirely devoid of credibility by the end of the Obama administration, and the same will be the case if they turn around to the opposite tack. Of course, the opportunity always exists for a great self-reckoning and a deliberate, visible effort to recapture objectivity.
November 27, 2009
Guarding the State in the Church
The person who brought my attention to Senator Sheldon Whitehouse's scheduled appearance at Central Congregational Church, in Providence, this Sunday, suggested that the politician is likely to face a very friendly audience as he gives his national healthcare pitch. It's all too obvious to wonder what might be the reaction were a right-of-center politician giving a political presentation at a more conservative church, but it's curious the effect that the event's being held by a religious organization can have on political opponents.
My own religious observation would cause me to miss this particular gathering, anyway, but I have to admit a reluctance to crash an event on somebody else's holy ground, as it were. Even with explicit permission from the church's leaders, there would feel something surreptitious about attending as political opposition.
Others with challenging questions for the senator might not share my inhibitions.
November 23, 2009
SNL Parodies Obama's "Wimpy Economics"
Saturday Night Live's most recent parody of President Obama (he's finally fair-game, apparently) calls attention to his "Wimpy Economics"--pay now, and we promise you'll receive later. Right.
“I am noticing that each of your plans to save money involves spending even more money.”
Health care "reform" is but the latest example--cuts and taxes will kick in immediately while benefits will start in 2013, for instance. And the promised savings are dubious anyway. For instance, the plan actually shifts Medicare costs onto the states, forcing them to deal with finding additional revenue (tax increases?) to handle the additional burden mandated by the federal health care "reform" plan.
November 21, 2009
A Deadly Scheme
Henry Aaron and Isabel Sawhill, of the Brookings Institute, provide a wonderful example of the insanity of allowing individuals to plan large segments of the economy:
So here is what we propose: Congress should enact a value-added tax, the equivalent of a broad-based sales tax on all goods and services. It should take effect only after unemployment has fallen to a predetermined level or in, say, five years, whichever comes first. Congress should link revenue from the new tax and other sources directly to public healthcare spending through a newly created healthcare trust fund. The trust fund would pay for all federal healthcare spending. This framework would mean that Americans would get the healthcare they are willing to pay for. If spending outpaces projections, Congress will have to choose between raising taxes and finding ways to slow the growth of spending.By balancing revenue and healthcare spending, such a reform would help solve America’s long-term fiscal problems. In the near term, it would also support and sustain the economic recovery. Consumers would be encouraged to buy now, before the tax takes effect. And by showing financial markets that Congress is determined to put our fiscal household in order, it would help keep interest rates low and encourage investment. The trust fund mechanism would strengthen incentives to institute reforms that will actually bend the healthcare cost curve, because measures to slow the growth of healthcare spending would avoid unpopular future tax increases that would otherwise be necessary.
How is it possible that people who are paid, essentially, to think can argue that a looming tax increase equivalent to one-sixth of the U.S. economy will encourage consumers to splurge while the splurging's good without making the parallel assessment that the huge taxes will suppress the economy once implemented? One of the reasons given in a previous paragraph for rejigging the healthcare system in a public direction is that, with ever-improving "medical interventions... [p]atients will insist on having them." Well, if the government must thus bend to supply what patients demand, why won't consumers learn the lesson and start demanding the things for which Aaron and Sawhill assume they'll splurge?
This program — which one may suspect will be the end result of the Democrats' healthcare path — would be a recipe for the hollowing and destruction of the United States of America, beginning with its entrepreneurial soul.
November 19, 2009
Incredulousness About Democratic Healthcare Promises is the Mainstream
If you didn't believe me last week when I posted…
We know that very few seriously believe that the Democratic reform proposals, in their current form, are going to truly reduce medical costs or control medical inflation.…will you believe Jeffrey S. Flier, aka the Dean of Harvard University's School of Medicine, who adds quality of care and access to care directly to the list of things that will not improve under the healthcare plan currently advancing through Congress…
Our health-care system suffers from problems of cost, access and quality, and needs major reform. Tax policy drives employment-based insurance; this begets overinsurance and drives costs upward while creating inequities for the unemployed and self-employed. A regulatory morass limits innovation. And deep flaws in Medicare and Medicaid drive spending without optimizing care.Speeches and news reports can lead you to believe that proposed congressional legislation would tackle the problems of cost, access and quality. But that's not true....In discussions with dozens of health-care leaders and economists, I find near unanimity of opinion that, whatever its shape, the final legislation that will emerge from Congress will markedly accelerate national health-care spending rather than restrain it. Likewise, nearly all agree that the legislation would do little or nothing to improve quality or change health-care's dysfunctional delivery system.
Progressive Warns: "If Conservatives Ran Healthcare"
Maggie Mahar of the Century Foundation warns:
If you’re a progressive like me, and you’re upset by the Stupak amendment, which bars federally subsidized insurance from covering abortions, consider this: What if we had a single-payer health-care system and someone like Jeb Bush or Sarah Palin were running the country?She then lists all sorts of bad things that bogey man Jeb Bush or the whirling dervish Sarah Palin could do if they controlled a theoretical single-payer system. The thing is, I wonder if she feels the same about all of the other liberal "must have" social engineering programs out there? Sounds like spin to me.Many liberals remain angry and disappointed that single-payer legislation never stood a chance in Washington. To them, a government-run health-care system seemed an obvious way to put patients ahead of profits.
But a single-payer system would have put us at the mercy of whomever happened to take control of Washington. I’m very happy to have a public plan as an option. But since I don’t know who will be in the White House in the years to come, I’m glad that government-run health care won’t be the only game in town.
Two Distinct Topics
Marc brought the topics of Vegas and boobies to last night's Matt Allen Show, and yes, they were two distinct topics. Stream by clicking here, or download it.
November 18, 2009
To Hell With "Government Experts", Keep Feeling Your Boobies
As an engineer, I'm quite familiar with the concept of the feedback loop, root cause analysis, etc. when it comes to preventive maintenance. For example, lets say you're supposed to change your oil every 3,000 miles. But over time, it's discovered that your car's engine runs just as well and doesn't wear any worse when the oil is changed every 5,000 miles. The obvious cost-savings is further bolstered by costs saved due to a reduction in the chances that the local lube shop will break something while performing this routine maintenance. (Generally, studies show that up to 20% of machine failures are introduced through scheduled maintenance).
It looks like the new recommendations that include pushing breast cancer screenings to 50 years old from 40 years old and advising against women performing self-breast examinations is based on a similar process.
The U.S. Preventive Services Task Force, a government panel of doctors and scientists, concluded that such early and frequent screenings often lead to false alarms and unneeded biopsies without substantially improving women's odds of survival.The problem here is that people aren't machines. When your talking about human life, the anecdotal examples that fall outside of the guidelines prove to be the rule. For every 5 false-positive 43 year olds, there is another 43 year old (or younger) who caught her breast cancer thanks to the current guidelines. There is no commensurate dollar figure."The benefits are less and the harms are greater when screening starts in the 40s," said Dr. Diana Petitti, vice chairwoman of the panel.
Dr. Eric Braverman, a clinical assistant professor of integrative medicine at Cornell Weill Medical College in New York, also backs the new guidelines, arguing that mammograms are not nearly as effective in detection as some other tests, like MRI's and ultrasounds.
"I'm not impressed by mammograms in general," said Braverman, who called manual examinations a "total failure."
"I support the new guidelines because I think it will lead to better testing. [The ultrasound] is a better screening procedure that's safer and easier and picks up things fast," he said, adding that he thinks women should receive ultrasounds as part of their routine medical exams, beginning at an early age.
Meanwhile Health and Human Services Secretary Kathleen Sebelius has said that "our policies remain unchanged" and that she "would be very surprised if any private insurance company changed its mammography coverage decisions as a result of this action." Wanna bet? Dr. Cynara Commer, a professor of surgery at Mt. Sinai's Surgical Oncology Department in New York...
...is very concerned that the new guidelines are the top of a slippery slope toward rationing, and questioned the timing as the Senate is about to vote on health care reforms that could end up containing a so-called public option.And men, don't take this sitting down. Your ass (colonoscopy guidelines) could be next."The government-run insurance companies are definitely going to be using these federal guidelines as opposed to using the American Cancer Society guidelines, and the American Cancer Society is not going along with these guidelines, and we can only hope that the private insurance companies don't follow suit," she said.
"I think it's coming down to saving costs. I don't think we should be doing that at the expense of women," she added.
November 13, 2009
A Fishy Kind of Reform
Andrew and Matt mulled evidence, on Wednesday night's Matt Allen Show, that there might be ulterior motives to current versions of healthcare reform. Stream by clicking here, or download it.
November 11, 2009
The Future of Healthcare Reform, If It's Built on Top of the Employer-Based System
An underreported aspect of the health reform proposals being advanced by Congressional Democrats (in both the House and Senate) is the conscious intent to maintain the current system of employment-based health insurance as the basis of the American healthcare system. Nobody implementing a healthcare system from the ground-up, from either the left or the right, would design a system that links health insurance eligibility to employment as American laws and regulations currently do, yet a majority of Congressional Democrats are firmly committed to extending into the immediate future, at least, the disproportionate role played by employers in access to health insurance.
Support for employer-based healthcare may make frighteningly raw political sense, if enough people have bought into the mistaken idea that employer-based healthcare is something that they receive for "free" (when in reality, it is no more free than any other part of employee compensation) and that tax-code and regulatory changes intended to remove the advantages that corporate health insurance purchasers have over individual insurance purchasers amount to corporate health plans being taken away by the government. Nobody likes to be told that something they already have is going to be taken away.
But I fear that an even more cynical calculation may underlie the Democratic commitment to employer-based health insurance.
We know that very few seriously believe that the Democratic reform proposals, in their current form, are going to truly reduce medical costs or control medical inflation. There just aren't that many convincing examples to point to where Federalizing regulation, providing subsidies and imposing mandates have historically reduced the cost of anything. Yet, Democrats are proceeding untroubled by this, mainly because of 1) a general detachment from fiscal reality that is the hallmark of the modern Democratic party and 2) a sincere faith that government can achieve any goal given enough power and treasure -- give government infinite resources and it will do infinite good!
Ultimately, the economics of the Democrats' plans depend upon cost-controls being imposed from the top-down, after the government has amassed enough power over healthcare to impose them. But Dems are not keen on explaining this aspect of their plan to the public -- they are quite fuzzy on what exactly the mechanism to control costs will be. So who will they blame, when it turns out that creating a government-run insurance company and new bureaucracies to oversee an employment-based healthcare system, in order to cover more people than are covered now without any reduction in quality of medicine, fails to reduce costs?
I suspect the blame will be directed towards the middlemen, to the employers placed by legislation and regulation between individuals and health insurers. Advocates for ever-increasing government power over healthcare will argue that their well-intentioned plans haven't worked because of choices made by greedy employers (who maintain disproportionate influence over healthcare choices under Democratic health reform plan) and that if more people can be moved into more directly government-controlled programs, then everything will improve as "planned".
In the end, the Democrats are setting up the American people for a choice between letting employers make their health insurance decisions for them and letting government make their health insurance decisions for them. If people are interested in a third option -- allowing individuals make their own health insurance decisions, without substantial interference from government or employers -- they need to let their representatives in Congress know that they want that choice, because the Democrats are in the process of creating a health care framework for the United States that could soon make this into an impossibility.
Medicare for None
Howard Walker, of Rockville, had a good letter in the Projo in response to the "Medicare for All" component of Froma Harrop's single-minded theme, of late. Unfortunately, the letter doesn't appear to be online, but here's it's key point:
Ms. Harrop never tells us how Medicare for All would contain health-care costs. In Rhode Island, Medicare "contains" costs by paying hospitals and doctors less than 90 percent of the actual cost of treating Medicare patients. Private insurers make up the difference: They pay more than the actual cost of treating patients and pass that expense on to their policy holders in higher premiums.That is, Medicare doesn't "contain" costs at all: It just hides them by shifting them to private insurance, which subsidizes Medicare. ...
There is no way private insurers can compete in such a marketplace. They will go out of business, leaving the government as the "single payer" — exactly the result left-wingers want but know they cannot sell to the public honestly.
How are Medicare and Medicare for All going to contain health-care costs once there are no private insurers left to shift them to? ... Medicare is already $35 trillion in the hole.
As with much else, when it comes to government involvement in the economy and our lives, it sounds good at first blush — and one can even get multiple 700-word columns whacking the same topic — but it doesn't withstand scrutiny.
November 8, 2009
An Even Bigger Bomb
As much as it's more pleasant to spend Sunday morning talking about our near neighbors' building bombs, moral obligation requires us to note that, by a margin of five votes (out of 435), the House of Representatives passed an even larger bomb, in the night, one that is certain to destroy our nation:
In a victory for President Barack Obama, the Democratic-controlled House narrowly passed landmark health care legislation Saturday night to expand coverage to tens of millions who lack it and place tough new restrictions on the insurance industry. Republican opposition was nearly unanimous.The 220-215 vote cleared the way for the Senate to begin debate on the issue that has come to overshadow all others in Congress.
A triumphant Speaker Nancy Pelosi likened the legislation to the passage of Social Security in 1935 and Medicare 30 years later. ...
The legislation would require most Americans to carry insurance and provide federal subsidies to those who otherwise could not afford it. Large companies would have to offer coverage to their employees. Both consumers and companies would be slapped with penalties if they defied the government's mandates.
There is no way that would-be nanny state totalitarians will be able to resist the temptation that this represents, or that our economy will survive it. It's times like this that I'm grateful that life forced me to learn a practical, hands-on trade.
We can only hope the behemoth collapses in the Senate.
November 7, 2009
No Coverage of Abortions Amendment to be Offered, in an Attmept to Get a Healthcare Bill Passed Today
Multiple sources are reporting that, in order to try to get the US House of Representatives to pass a Democratic version of healthcare reform today, House Speaker Nancy Pelosi has agreed to a floor vote on an amendment that would prohibit either a public-option insurance plan or any plan eligible for a government subsidy from covering abortions. Here's the New York Times' take…
[Congressman Bart Stupak’s] amendment would bar any insurance plan that is purchased with government subsidies and the new public plan from covering abortion. Other insurance plans, approved by the government for sale through new exchanges or marketplaces, would be allowed to cover abortion provided they did not accept federal money. Separately, people who purchase subsidized insurance, could buy separate coverage, with their own money, for abortions.Also of particular local interest, the Politico website is reporting that the United States Conference of Catholic Bishops has issued a letter stating that they believe the Stupak amendment provides enough of a restriction on the use of public money for abortions to enable them to support an overall healthcare bill.
November 6, 2009
Absolutes Only Halt Debate When They Meet with Intransigence
I'm straining for a silver lining, to be sure, but Congressman Patrick Kennedy does offer the useful service, from time to time, of stating rhetoric that is sufficiently blunt to expose the error underneath. With reference to the fight he picked with the Catholic Church:
Kennedy also said that no group "is getting everything it wants" in the medical overhaul. The church "has every right to promote its position," he said, but if a group "seeks to impose absolutes on the debate, we are left standing idle instead of moving our nation forward."
That's only the case if those determining the course of the issue are intransigent in the face of the absolute. Every party to a negotiation has a bottom line that it will not cross; the process moves forward by determining the proximity to that line that other parties find tolerable.
This is even true of folks like me, whose bottom line is that the government should not be a significant force in the healthcare system. The way forward would be to figure out my determination of "significance" and explore alternate methods of achieving hoped-for ends. (That assumes, of course, that the hoped-for end isn't in actuality government ownership of the healthcare system, which is probably the case for more than a few healthcare "reform" advocates.)
November 5, 2009
Mark Zaccaria: Respite Care vs Political Posturing
As an avid follower of the activities of Representative James Langevin, I read with interest his recent release on the subject of Respite Care here in the Ocean State. I read it with interest, but also with a certain amount of approval.
The Congressman correctly highlights the aid rendered by the many uncompensated family caregivers here in Rhode Island, at least 114,000 by his count. All of us should celebrate the contributions made by these family members and friends of those in need of ‘round the clock care in an increasingly expensive world. Most of these important members of the health care chain became links in it due to circumstance rather than by choice. I know. For 28 years my wife, Ruth, and I were part of that team as we provided home care for our son Adam.
The eldest of our three children, Adam was diagnosed with autism as a toddler. It set our family on a path of gaining expertise about that syndrome which none of us ever planned on acquiring. Like the 114,000 Rhode Islanders the Congressman referenced in his release last week, though, Ruth and I did what we had to do. In fact, during the period of my business career when I was a corporate nomad we did it in several other states. None of them had programs or even formal support nearly equal to that we received when we got back here for good, ten years ago.
So I applaud my Representative in Congress for the focus on respite care he spotlighted in his recent release. It is a service to uncompensated caregivers that exists in this state but most certainly does not in many others. Respite care can also be a Godsend to parents, friends, or siblings who find themselves stretched to the breaking point. They can be recharged by a day-off from long term homecare duties. It frequently lets them return to the fray reinvigorated and better able to shoulder the load.
In reading my Rep’s account of his action in support of this cause, however, it was hard to miss a couple of glaring admissions. He wrote that he’d spent five years working to pass legislation to support respite care and he even referenced HR3248 of the 109th Congress, known as the Lifespan Respite Care Act of 2006. The bill was introduced in the House in September of 2005 by a New Jersey Rep. and it was passed in 2006 by both chambers and signed into law by President Bush on December 21st of that year. For the record, Congressman Langevin was one of this bill’s 84 co-sponsors in the House. Now, nearly 3 years after passage, he touts a grant of $200,000 for Rhode Island that has been secured under the legislation.
That amount, which averages out to just over $1.75 per Ocean State caregiver, will be split between three existing programs here. No doubt the money will be well spent to cover the on-going overhead expenses of keeping them running.
What I feel I do have to doubt is that this amount will be granted again at any predictable point in the future. It’s very nice that Mr. Langevin has brought home a couple slices of bacon, and chooses to trumpet that fact. It must mean that’s the best action on our behalf that he’s got to crow about right now. It also must mean that he has not set himself about assisting these important local programs with any kind of long term support that their managers could count on to help improve things for Rhode Islanders for years to come. Dare we ask why there was no talk in last week’s press release about expanding the availability of respite care as a direct result of the Congressman’s efforts?
They can’t all be home runs, of course, but it strikes me that our guy has tried to slip one past us with his recent puff piece on respite care. Right now the excess spending of past administrations has become the egregious and unsupportable spending of this one. It’s a time when I would have preferred to hear about how my Representative plans to assist in warding off the price inflation that looms on our horizon as a result. He seems to have voted in favor of every single one of the recent spending initiatives that have taken billion-dollar deficits and made them trillion-dollar deficits in less than a year. Can you help me understand how that’s a good thing for me, Congressman?
The saddest part of it all is that he must think we’re not watching. He must think he can get away with keeping his name in print with the legerdemain of an occasional misdirection press release while he attends to business as usual in Washington. As I said at the top, I’m watching. I bet you are, too.
Mark Zaccaria is a small businessman and former elected official who was Congressman Langevin’s GOP opponent in the 2008 election. Mr. Zaccaria plans to run again for the seat in 2010.
November 4, 2009
No Price Tag Doesn't Mean No Price
Professor Stephen Mathis has come across my post responding to his op-ed, and he comments, in part:
I think the ultimate problem with devaluing people or their organs is problematic precisely because it makes them vulnerable to more powerful folks. But I do disagree that disallowing a price tag on organs makes them worthless: I think it simply makes them incommensurable with money, which marks off their special status as things that are unlike everyday commodities. The same goes for laws outlawing the selling of sex. Making it impossible to buy or sell sex doesn't make it worthless, rather it delineates it as something so special it shouldn't be open to the pressures of the market (that usually come from the powerful/rich).
I don't know Mr. Mathis's background, but I'd suggest the possibility that he's just never encountered a situation in which he's needed a sufficient amount of money that would justify the sale of a body part. I'll tell you the honest truth: I'd part with certain bodily properties if I could thereby erase my debt.
The economics are unavoidable: Every body part has an abstract value; that we disallow their sale just removes the motivation to assign a dollar amount to it. The same is true of sex, although the value is so much lower, and unlike organs, its sale doesn't deprive the seller of its use, so some people will always make the transaction, whatever the law says.
Drawing the Wrong Conclusion from Statistics
Just a minor observation based on the story in ProJo about Tamiflu, which states:
A recent check of prescribing data from pharmacies around the state found that 15 percent of Tamiflu prescriptions were filled five days after they were written.Not so fast, doc. I have a prescription for Tamiflu given to me "just in case". I haven't filled it yet because I don't have the flu. I wonder how many other people do the same thing--get the scrip and wait until flu actually manifests before filling. I can understand the conclusion being drawn, but peoples actions aren't always so "A --> B".That means a lot of wasted Tamiflu, says Health Director David R. Gifford –– because the drug works only if you take it within a day or two after you start feeling ill.
November 3, 2009
Error and Redundancy
Congressional United Church Pastor Eugene Dyszlewski took to the Projo letters section, on Sunday, to attack Roman Catholic Bishop Thomas Tobin for his criticism of supposedly Roman Catholic Congressman Patrick Kennedy, who had attacked the Catholic Bishops for continuing to oppose abortion funding within healthcare legislation. Writes Dyszlewski:
The congressman poses a legitimate question about how the Catholic Church could be against the biggest social-justice issue of our time. It remains to be seen what specific language in what bill raises the abortion concern. Federal law already includes a ban on abortion financing; demanding redundant legislative language in the bill under the threat of opposition seems oddly unnecessary.
It would be preferable if religious leaders were less prone to logical error and the promotion of misinformation. For illustration of the first count, imagine a "comprehensive healthcare bill" that would cover all those millions of uninsured Americans (or non-Americans, as the case may be), but that had a provision for the execution of Protestant ministers. Would it be inexplicable opposition to "the biggest social-justice issue of our time" to require the removal of that provision as a prerequisite for supporting the bill? The reverend is merely trading in deceptive political rhetoric.
On the second count, Dyszlewski is astonishingly strident about the redundancy of the language for which pro-lifers are calling. At best, it appears that the only real question is the mechanism by which federal dollars would flow to abortion providers. If Dyszlewski is referring to the Hyde Amendment, he's simply wrong. That annual appropriations rider applies only to the Health and Human Services appropriation, from which healthcare legislation would have distinct revenue. The upshot is that unique legislation does, in fact, require a targeted ban.
If Rev. Dyslewski believes that financing the killing of unborn children is a small price to pay for a bill that will ensure the erosion of our healthcare system, then it would be more honest of him to come out and say as much. In the meantime, I'd caution him against making common cause with the likes of Stephan Brigidi, of Bristol, who used the same space a couple of days previous to express his zealotry for banning religious leaders and their beliefs from the public square. "For far too long," writes Brigidi, "this interference has gone unchallenged, such as the reciting of rosaries and prayers under the State House rotunda to oppose certain legislation."
There's a reason the "right" to abortion rises up in tandem with an urge to restrict rights of religion and free speech, and religious folk would do well to contemplate it.
November 2, 2009
In Favor of Options – Even Non-Government Ones!
Hurrah to the Projo editorial board, for recognizing that governmental regulations can artificially increase the price of health insurance in non-rational ways…
We noticed the other week, for instance, that an insurance policy in Maryland has a premium half the size, and with better coverage, than a similar policy sold by Blue Cross and Blue Shield of Rhode Island, but other than by moving to Maryland there is no way to buy it....There is some chatter in the internet about the best route to change the laws (see here, for example), but the point is that medical inflation rates greatly in excess of the basic inflation rate are not the result of some unalterable force of nature. They've been created, in large part, by the unintended consequences of poorly-thought out laws -- laws that can be changed if their adverse impacts have created problems that are bigger than the original problems they were intended to address.Getting rid of the antitrust exemption and letting people shop for insurance nationally would be good steps in controlling costs.
A Healthy Market
Wheaton College Philosophy Professor Stephen Mathis questions "how appropriate it is to address health concerns using a for-profit model":
Consider that we have numerous treatments for erectile dysfunction, while drug companies have resisted putting resources into finding a cure for malaria, a disease most prevalent in poorer countries.
Professor Mathis might profit from a viewing of my video blog describing the effects of attempts at manipulating economic behavior. We have treatments for erectile dysfunction because people want them. Reformulating the healthcare system in such a way as to deny that sort of research and to force investment in other areas of less market demand will not have the intended effect and will require escalating infringements on freedom.
For the individual, the choice isn't between cures for erectile dysfunction and malaria research, but between cures for erectile dysfunction and a new car (or whatever else the individual might spend his money on). Push hard enough, and the choice becomes one between funding malaria research and declining to work so hard or take financial risks with the hope of prospering.
Mathis has other misconceptions about medicine and the market:
First, we tend to think it inappropriate to profit from others' misfortunes, whether they are illnesses or accidents. This also helps explain why our police and fire departments are all either government-funded or volunteer. So when it comes to protecting lives or saving them, we disapprove of those who profit from others' misfortunes because they take advantage of others when they are vulnerable.Second, we have laws against buying and selling human organs. We do not let individuals buy or sell organs because we think it is inappropriate to put a price tag on such things as bodily organs. This also explains why we do let individuals donate organs.
In the first case, I'd suggest that it isn't an abstract sense of appropriateness at play, but of danger. Nobody begrudges financial gain for those who save lives; rather, we're wary of circumstances in which lifesavers could leverage dire need at a crucial moment in order to extort greater payment. It's not that we have a moral problem with police and firefighters making a healthy living for their services and the risks that they take; it's that we fear a scenario in which they stand at the door with their hands out before collaring the murderer or dousing the flames. The former is a matter of compensation; the latter is a matter of complicity in crime and destruction.
Similarly, in the second case, we don't fear that devaluing organs through sale will devalue their owners. The devaluation of the person comes first. If you're a person with explicit dominion over your body, then others must approach you as a being capable of making decisions, a peer; if you're a shell for valuable organs, then others can focus on plying those organs from you. Consider:
... outlawing organ sales is a way of making clear that, as a society, we think individuals should never have to face certain decisions — say, between filing for bankruptcy or selling a kidney.
Wrong. Outlawing organ sales is a way of preventing immoral actors from targeting your finances as a means of acquiring your kidney. Indeed, it cannot be moral, and it devalues organs, to declare that a man must watch his family suffer because we've erased his kidney's market value. Not allowing individuals to "face certain decisions" doesn't relieve them of the horror of their circumstances. In that case, organs are literally worthless, except insofar as they keep individuals sufficiently healthy to make of themselves workhorses. But it devalues the entire person — and his family, too — if constructing an economy full of pitfalls can push him toward harvesting his body. In other words, it isn't the decisions of the individual against which we're guarding, but the decisions of the entire society.
The implications for our healthcare system are straightforward. My premise is that we restrict acute freedoms (such as selling one's organs) and circumscribe the profitability of safety in order to protect the vulnerable from the powerful. Consolidating healthcare decisions and handing the powerful a right to make them hardly alleviates that danger.
October 28, 2009
RE: Medicare Fraud
I referenced a 60 Minutes report on Medicare fraud earlier this week. Mark Hemingway adds some additional context:
Medicare fraud amounts to $60 billion dollars a year. That is one heck of a lot of money. In fact, Medicare loses seven times as much money in fraud every year than the combined profits of the 14 health insurance companies on the Fortune 500. Medicare currently covers 46 million people. How much more money will be lost to fraud when an additional 88 million people are dumped off of employer health insurance rolls in favor of a public option?And remember, one of the primary reasons that the public option is supposedly better than private insurance is low administrative costs. Well, a major reason why private insurance has higher administrative costs is that, unlike the federal government, they make a genuine effort to combat fraud.
October 26, 2009
Medicare Fraud: "They would pay first and send an auditor later. "
Proponents of the "public option" like to point to MediCare. It ain't the panacea they say, as 60 Minutes reported:
President Obama says rising costs are driving huge federal budget deficits that imperil our future, and that there is enough waste and fraud in the system to pay for health care reform if it was eliminated.An example:At the center of both issues is Medicare, the government insurance program that provides health care to 46 million elderly and disabled Americans. But it also provides a rich and steady income stream for criminals who are constantly finding new ways to steal a sizable chunk of the half trillion dollars that are paid out each year in Medicare benefits.
In fact, Medicare fraud - estimated now to total about $60 billion a year - has become one of, if not the most profitable, crimes in America.
Once criminals like Tony get their hands on usable patient numbers, they try and charge Medicare for the most expensive equipment possible, which requires having access to a list of Medicare codes.How could this happen?Asked what some of the best codes were, Tony told Kroft, "Artificial limbs, electric arms, electric wheelchairs. I mean, a regular patient, you can put them on two artificial legs and an artificial arm and they'll pay for it."
And that's what happened to former Federal Judge Ed Davis. He was one of those patients who started getting charges on his Medicare statement for artificial limbs.
"And I looked at it and it had charges for prosthesis. And I knew I had my arms," Judge Davis explained.
Though he has two healthy arms, his statement showed Medicare had been billed for a left and a right arm.
"Didn't anybody in Medicare check to see if any of these charges were valid?" Kroft asked Tony.
"Sometimes they'll do it. But by the time they did it, it was too late," Tony said. "We've already made $300,000, $400,000, $500,000 on it. And then we will never send 'em nothing back. And then at 30 days they'll send an inspector to your office. And by that time…it's all closed down."
They would pay first and send an auditor later.
Kim Brandt, Medicare's director of program integrity...[said] "Well, it really does come down to the size and scope of the Medicare program, and the resources that are dedicated to oversight and anti fraud work. One of our biggest challenges has been that we have a program that pays out over a billion claims a year, over $430 billion, and our oversight budget has been extremely limited," Brandt said.That statement by Holder is about as naive as it gets.About that there is little dispute: Medicare has just three field inspectors in all of South Florida to check up on thousands of questionable medical equipment companies.
"Clearly more auditing needs to be done and it needs to be done in real time," Attorney General Eric Holder said.
Asked why it has taken Medicare so long to figure out they were being scammed, Holder told Kroft, "I think lack of resources probably. And then I think people I don't think necessarily thought that something as well intentioned as Medicare and Medicaid would necessarily attract fraudsters. But I think we have to understand that it certainly has." {emphasis added}
October 23, 2009
Kennedy and Obama vs. Catholic Church and Fox
Something's been gnawing at me since Andrew posted video of Congressman Patrick Kennedy proving once again why we should all hope his handlers keep him well away from any real power, and it took a revistation of Ed Achorn's concern about the Obama administration's jihad against Fox News to jar the pest loose. Here's Achorn:
The White House's declaration of enemy status for Fox seems to reflect a growing disrespect throughout our society for free speech, the wellspring of America's greatness and generous spirit. A president of all Americans, even those who disagree with him, should have the grace and bigness to realize that.Ominously, growing numbers of Americans seem to think that it is illegitimate for anyone to have an opinion at variance with their own. And that those who disagree — or would report facts that challenge their viewpoint — become a fit target for retaliation, punishment, abuse, even the coward's art of slander.
Kennedy's dismissing the Church's easily foreseeable objection to the probability that the Democrats' version of healthcare reform will fund abortions as a "red herring," and his declaration that the bishops are sowing "dissent and discord" is precisely in the line of Achorn's criticism.
When Reform Doesn't Fix What's Wrong
Firefighter and EMT Michael Morse, as he works to get his body back into occupational shape, reflects on the future of healthcare in a system that calls a city ambulance rather than permitting patients to take their cars to another building in the same medical campus:
... The medical community is as clueless as the rest of the population who abuse the 911 system on a daily basis. I can hardly wait for whatever healthcare reform comes out of Washington. Something tells me I'll be driving people to Physical Therapy appointments, at taxpayer expense.
And then what happens when the heathcare system planners work the cost of such transportation into the total cost of the therapy and begin denying treatment in some cases because the total expense is too high? I know, I know. It'll never happen. We can trust our government and its functionaries to be reasonable.
October 17, 2009
Killing in the Name of the Law
Put assisted suicide on the long list of issues that ought to be left to the states, but that I'd oppose in my own. In the name of civil liberties that conflict with the (until recently) long-standing moral consensus of our culture, we're building a giant trap that will at some point close on us all — probably too slowly to cause alarm — and leave us absolutely free to drug ourselves into a stupor for a neighborhood orgy as a sendoff to a middle-aged friend who'll be visiting the city death dispenser because public healthcare won't cover his methadone anymore. As for practicing religion, speaking our minds on politics during campaign season, and engaging in productive economic activity... well, a culture's got to draw the "unfree" line somewhere.
But back to states' rights and euthanasia — sorry, assisted suicide. The problem with the state-by-state experiment model is that those who advocate for the creation of innovative culturally discordant laws have incentive to make their ill effects difficult to trace, and so we get a scenario such as Wesley Smith describes here:
These advances would not have happened but for a powerful myth promoted by assisted-suicide advocates and helped along by a compliant media: the notion that Oregon's experiment with legalized assisted suicide has been a success, in which problems and abuses are rare or nonexistent. It is true that the annual statistical reports published by the Public Health Division (henceforth OPHD) of Oregon's Department of Human Services have revealed very few problems. But there's a reason for that: The reporting system was designed by the authors of the assisted-suicide legislation to be incapable of vigorous policing and in-depth data gathering.As a result, nobody knows precisely what is going on in Oregon. The data in the state-published reports are based overwhelmingly on self-reporting by death-prescribing doctors — who are as likely to admit violating the law on this matter as they are to tell the IRS that they have cheated on their taxes. Indeed, as the bureaucrats charged with publishing the annual report admitted to an investigative committee from the British House of Lords, the OPHD engages in only very limited and random checking of the information it receives. Moreover, the department has no budget or authority to investigate apparent violations of the law, and all documentation relied upon in writing the annual report is destroyed once the report has been published. Dr. Kathleen Foley, perhaps the nation's premier palliative-care doctor, and suicide-prevention expert Dr. Herbert Hendin wrote in the Michigan Law Review last year that the OPHD "does not collect the information it would need to effectively monitor the law and in its actions and publications acts as the defender of the law rather than as the protector of the welfare of terminally ill patients."
The cliché of the distopia is a sepia-hued society in which everybody fears to act — fears to do anything but work and support the government. The reality, I prognosticate, will be much more a colorful pictures of people free to indulge their darkest notions but undermined wherever they seek to build something positive.
October 16, 2009
ProJo Editors Support Single-Payer and Higher Taxes
In his Wednesday column, "The trouble with health care is paying for it", Michael Barone wrote:
We know now that it costs a lot of money to pay for insurance policies with expanded coverage for an expanded number of people. And we know that no one wants to pay the price.It also happened in Maine and other states that tried to offer a "public option." For their part, the ProJo editors see the mish-mash of problems reflected in the current plans being considered in Washington and think the problem is lack of a "public option". Further, they remain convinced that the best option is not less government intrusion into health care, but more. Particularly in the form of a universal, single-payer system:We may be in the process of learning something else. Which is that insurance coverage that further insulates patients from costs results in unanticipated increases in health care spending. Yes, it bends the cost curve, but in the wrong direction. That's what has happened with the much-praised Massachusetts system.
....how much more economical and efficient a single-payer plan would be than the mosaics being created in Congress to please the insurance companies spending so much money there. Health insurance works best for the public when the pool covers as wide a spectrum of the population as possible.However, as they admit, we'll have to be taxed more to pay for this "economical and efficient" system:
Such devices as taxes on fancy “Cadillac” insurance plans, meant to move people into less-expensive ones, and smaller federal subsidies for private Medicare plans, which have been wonderful cash cows for insurers though very expensive for the public and providing no real benefit to public health, would help a bit.Well, at least their honest. If we really want the European style health care the ProJo continually trumpets, we'll have to pay European style taxes to support it. With the current recession, that's really good timing, guysBut broad-based taxes will have to be raised (or invented) to pay for universal coverage and for Medicare costs for the Baby Boomers as they slide into decrepitude.
October 14, 2009
That PwC Report on Healthcare Costs
The Providence Journal headline was "Insurance lobbyists take the gloves off," and the AP report above which it appeared cast the story in terms of the political battle, as if it is immaterial and unknowable whether a study issued by PricewaterhouseCoopers is accurate:
The firm's study projected that the legislation would add $1,700 a year to the cost of family coverage in 2013, when most of the major provisions of the Baucus bill would be in effect.Premiums for a single person would go up by $600 more than would be the case without the legislation, it estimated.
In 10 years' time, premiums would be $4,000 higher for a family plan, and $1,500 more for individual coverage.
From the voter/consumer perspective, this is a bit like watching two giants wrestle over who gets to eat more of us. Neither of them is interested in measures that would actually set us free or in our desire to explore the marvelous facilities that they've promised will be found in their belies. So, put the article aside and refer back to it, in a decade, so we'll know whom it is we hear saying "I told you so" as we're digested.
October 13, 2009
Links to various articles
Power Line on Taking the National Debt Seriously
Veronique de Rugy on Elinor Ostrom and the Essence of Economics
Jagdish Bhagwati on Feeble Critiques: Capitalism's Petty Detractors
Power Line on Democrats to Curtail Free Speech
Cato on What Does the State Department Not Want Us to Know about Honduras?
John Derbyshire on The Thatcher Giant
ADDENDUM #1:
Harsanyi on The doers against the "thinkers"
Russ Roberts on Stimulus in the Real World
Victor Davis Hanson on The Power of Payback
Milton Friedman on 4 Ways to Spend Money
Milton Friedman on Libertarianism (Part 1 of 4)
Milton Friedman on Libertarianism (Part 2 of 4)
Milton Friedman on Libertarianism (Part 3 of 4)
There Will Be Rationing
Further to this morning's vlog, John Goodman's got a good explanation of the reason that Sarah Palin's "death panel" comment was broadly accurate. He touches on the public sections of the healthcare industry, but then moves on:
As currently envisioned, private health plans and at least one public plan would compete. The plans would be free to set their own premiums but would have to charge all enrollees the same price, regardless of their health status. Because some plans will attract a greater percentage of sick enrollees than others, a government administrator will have the power to "tax" plans with healthier enrollees in order to subsidize plans with sicker enrollees, through a process called risk adjustment. And it is through this process that the government will have enormous power to control what is done for the sick.Suppose a plan attracts an above-average number of people whose doctors say they need hip replacements. The company asks the government risk adjuster for a subsidy to cover the cost. The risk adjuster may decide these hip replacements constitute "unnecessary care" or "futile care" and deny the request. In this way, the risk adjuster will effectively force doctors to deny people care.
The risk adjuster will be aided by a national health board, which will do "comparative effectiveness" analyses. If the health board decides that a hip replacement is "unnecessary" or "futile," it will offer cover for the risk adjuster to deny payment and for insurers to deny care.
Vlog #9: Planning Against Human Nature
Herewith, further thoughts emerging from things said at healthcare town halls. The focus is, obviously, healthcare, but the argument is against socialism in general (ahem).
October 12, 2009
Swine Flu Disconnect
Is it just me, or is there an odd disconnect with this swine flue thing? The White House human services secretary has been giving the vaccine a round of marketing, and I know that schools in Tiverton, at least, are offering it to students on the premises. Yet, our pediatrician doesn't recommend it (which is not to say that she recommends against it).
It's a bad bug, as Mark Hemingway attests, but as Hemingway also attests, it's hardly a beast more fearsome than many of us who've made it into adulthood have already experienced several times. We face such illnesses down and survive, appreciating what it means to be healthy and sick.
Personally, I can't shake the feeling that there's something more to this hysteria. Some model to prove or cultural impulse to change, and being conservative, once suspicious, I'm resistant.
October 11, 2009
Congressional Candidate John Loughlin Healthcare Town Hall, 9/30/09
As I said, I was a little late to John Loughlin's healthcare town hall, a couple of weeks ago, but I did get most of it on video and capture a good number of interesting points from all involved.
Continue reading "Congressional Candidate John Loughlin Healthcare Town Hall, 9/30/09"October 6, 2009
More of the Same from Kennedy
Hiding behind his quaking fear of "violent rhetoric," Congressman Patrick Kennedy staged a comfy tele-town hall meeting:
Most of the participants — each of whom had their questions screened ahead of time by Kennedy staffers — appeared sympathetic toward changes to the nation's health-care system. ...Tiverton resident Teresa Rudd said she remained on the line for much of the hour to ask Kennedy about how the proposals now in play treat the abortion issue. She didn't get the chance to ask.
"It didn't seem like there was any opposition," Rudd said afterward. "It seemed like one big commercial for health-care reform."
However much outrage Kennedy may express on behalf of the powerless rabble, it's clear by his actions that he doesn't hold his constituents in very high regard.
September 30, 2009
A Campaign Event Healthcare Town Hall
I'm about a half hour late, but I've made it all the way across town in Tiverton for John Loughlin's healthcare town hall event, as part of his campaign for Congressman Patrick Kennedy's seat. There are quite a few people here — somewhere around 130 or 140 — with a high local contingent. I can't be the only person who found the 5:30 start time a little early for a three hour event, but plenty of people turned out.
Steve Peoples and other Providence Journal folks are here. Local papers. And a couple small-camcorder folks.
As I set up, RIILE's Terry Gorman was talking about illegal immigration and healthcare. That issue has dominated the audience questions. It appears to be a very friendly crowd, by the way.
6:28 p.m.
Bill Felkner just quoted Obama's "if you like the healthcare that you have" line and the audience pretty broadly agreed: "he lies."
Loughlin: "Is Joe Wilson here?"
6:53 p.m.
One audience member noted that a family of five owes more as a function of national debt than the average mortgage payment in Rhode Island. "Are we nuts?"
7:01 p.m.
The tempo of the event seems to pick up when the topic pushes the boundaries of the healthcare issue. One audience member just asked Rep. Loughlin about his intentions with respect to the military and veterans. Loughlin was clearly more animated, and the audience began to get worked up.
Perhaps the lesson is that he should have issue-related events with targeted audience and relevant panelists (e.g., military folks speaking on military issues... Afghanistan would be good). Keep momentum rolling. Use the campaign almost as a political tool for raising current events, making the emphasis of his campaign the issues — and the voters' concerns — rather than himself.
7:07 p.m.
One of the panelists made the point that the American healthcare system is not the best healthcare system in the world. The audience was split on whether to shout objections or to shout objections to the objectors.
7:09 p.m.
Peter Asen (of Ocean State Action, I believe), who was also at the Kennedy event, just stated that, in Rhode Island, only Blue Cross offers individual plans because only Blue Cross is willing to play by the rules and abide by coverage mandates (such as preexisting conditions). His argument was that we can't allow healthcare buying across state lines because everybody will flock to the cheapest programs in states that let them get away with everything.
Well, that pretty much sums up the differences in philosophy. The left wants to institute "fixes" and then layer on controls when the outcomes don't match their desires. As they must, the controls will simply ratchet.
Every newspaper in the room sought comment from Mr. Asen.
7:20 p.m.
The audience isn't ready to move away from the question of whether the United States has a bad healthcare system.
Room thinning quickly.
Hints of Things to Come with Public Healthcare
An interesting find by Joseph Bottum. Belmont Abbey College, an institution sponsored by Catholic monks, opted to remove provisions for abortion, contraception, and sterilization from the healthcare plan that it offered employees, as it must do as an institution run by believing Catholics. The matter will end up in court, but the Equal Employment Opportunity Commission chimed in with this specious ruling:
Now, after a complaint was filed by eight faculty members, the U.S. Equal Employment Opportunity Commission has ruled that Belmont Abbey is discriminating against women: "By denying prescription contraception drugs, Respondent is discriminating based on gender because only females take oral prescription contraceptives. By denying coverage, men are not affected, only women." Should the college and the faculty members who filed the complaint not be able to reach an acceptable settlement, the EEOC can file a lawsuit against the college in federal court.
Apart from setting an apparent precedent that any medical procedure relevant to only one gender must be covered on the grounds that the other gender isn't affected by lack of coverage, the ruling contrasts explicitly with North Carolina law. An unelected federal board, in other words, is attempting to assert its authority above elected representatives at the state level.
This is one of those topics on which we must remind the ruling political faction that they will not always rule (no matter how confident "progressives" are that things will always move in their direction). Removed from all ideological specifics, the size and reach of the ever-growing federal bureaucracy cannot be otherwise than a suppressant of freedom.
September 29, 2009
Democrats Agree: Health Care Reform Should Cover Illegals
President Obama recently exhibited some clumsiness trying to play a shell game on illegal immigrants and health care reform:
Even though I do not believe we can extend coverage to those who are here illegally, I also don't simply believe we can simply ignore the fact that our immigration system is broken," Mr. Obama said Wednesday evening in a speech to the Congressional Hispanic Caucus Institute. "That's why I strongly support making sure folks who are here legally have access to affordable, quality health insurance under this plan, just like everybody else.Other Democrats are being more straight forward:Mr. Obama added, "If anything, this debate underscores the necessity of passing comprehensive immigration reform and resolving the issue of 12 million undocumented people living and working in this country once and for all."
Fearful that they're losing ground on immigration and health care, a group of House Democrats is pushing back and arguing that any health care bill should extend to all legal immigrants and allow illegal immigrants some access.The Democrats, trying to stiffen their party's spines on the contentious issue, say it's unfair to bar illegal immigrants from paying their own way in a government-sponsored exchange. Legal immigrants, they say, regardless of how long they've been in the United States, should be able to get government-subsidized health care if they meet the other eligibility requirements.
"Legal permanent residents should be able to purchase their plans, and they should also be eligible for subsidies if they need it. Undocumented, if they can afford it, should be able to buy their own private plans. It keeps them out of the emergency room," said Rep. Michael M. Honda, California Democrat and chairman of the Congressional Asian Pacific American Caucus....Mr. Honda and his allies, though, say illegal immigrants should be allowed to pay for insurance if they can afford it, even if it comes through a government-established exchange. As a generally young, healthy part of the population, illegal immigrants could help reduce overall costs for those who buy into health exchange plans, the lawmakers said.
September 26, 2009
Violence and Fear in Healthcare
Steve Peoples' article about this morning's event focuses on Kennedy's lamentation that heated protests may produce violence — of which (he stated) his family has seen too much. There's an interesting juxtaposition if we play Peoples backwards, as it were (emphasis added):
"Unfortunately, these town hall meetings have been hijacked by these Tea Party folks and extremists who really take away from the honest dialogue on the facts of the debate and end up seeing this issue devolve into fear mongering and the peddling of misconceptions," [Kennedy] said, referring again to the sign that referenced his father's death.
But earlier:
Tsiongas said that those who depend on the current health-care system are right to be afraid."What they should be afraid of is that we do nothing," he said, "because if we do nothing we can no longer be able to afford this health-care delivery system as it stands."
I guess fear mongering is only a bad thing when conservatives and Republicans do it.
Kennedy and Friends in Forum
Inasmuch as the first 10-minute video clip from this morning's forum on healthcare began attracting viewers almost as soon as I posted it, and the first has surpassed many clips from previous events that have been up for weeks, interest would seem to be high.
Therefore, I've put the videos that the various computers involved have finished processing in the extended entry and will add the rest as they're available. (There are twelve, in all.)
Continue reading "Kennedy and Friends in Forum"
A Confusing Set of Intentions
The sales pitches for the Democrats' healthcare reform are flying so furiously that it's difficult to trace the intellectual threads that ought to be binding the various parts of the plan together. Consider:
President Barack Obama has endorsed the proponents of the insurance tax. This says it would help lower health care costs by encouraging people to become more cost-conscious health care customers.Most high-cost health care plans cover co-payments and deductibles so there is no dollar spent for health care.
Unions argue that they are giving up higher pay to secure better health care benefits. It is likely that insurers will pass on the cost of the tax through higher premiums.
Even if we adjust for the journalist's poor writing skills, the rhetoric has a thrown-against-the-wall quality. Pull the sticking pieces apart, and this is about what you get:
- A tax on high-end health insurance plans will be levied to help with "covering the uninsured."
- The tax will be passed on to premiums, increasing the price to consumers.
- Consumers will move away from plans that hide copays, thus increasing their awareness of the costs of their healthcare and making them more likely to conserve.
What happens when people react to the incentives such that there are fewer high-end plans to tax, leaving insufficient money to cover the uninsured? One supposes that the answer would be some variation of, "It doesn't matter." It doesn't matter, because a coherent strategy is not the objective; either an emotional balm or a route to bigger government is.
Democrats and their supporters have spent far too much time rehearsing the Obama school of political salesmanship: promise to heal the wounds of the suffering, mix in some of the opposition's language so "moderates" can imagine that your policy is economically rational and objectively considered, and pretend the cost will be borne only by the ultra-rich minority.
If increasing "cost consciousness" among healthcare consumers were a goal, there would at least be lip service paid to health savings accounts. If the transfer of healthcare dollars from the rich to the poor were the goal, then there would be some plan to adjust to the predictable free-market shifts caused by government incentives.
Ultimately, the whole thing is either a scam or a failure of thought so thorough as to undermine the very premise that a government organization could operate a flashlight, let alone a healthcare system.
Healthcare Town Hall... Not So Much
Quite a different event, Congressman Patrick Kennedy's version of the healthcare forum. Whereas Congressman Langevin placed himself bare before a roiling theater setting and Senators Whitehouse and Reed rolled up their sleeves for a folksy round of after-dinner discussion (somewhat more controlled, but with agreement and disagreement), Kennedy is participating as a "special guest" in an AARP "health care reform forum." He's one of four panelists, the others being:
- RI State Nurses Association Executive Director Donna Policastro
- AARP-RI Executive Council Member Ann Gardella
- RI State Medical Society Former President Nick Tsiongas

Sadly, nobody is outside in the parking lot protesting either Kennedy's position on this issue or his version of "meeting with constituents."


9:07 a.m.
Lots of suspicious looks from the party folks and the other members of the media with whom I'm sharing the back of the room. I'm not the only small-camcorder tripod operator, either, although I take it that's not necessarily an indication of citizen journalism, any longer.
Kennedy's making the rounds. Were I a politician, apart from discomfort with the room-working, I have to say I'd be annoyed at the constant camera presence. Guess you learn to live with it.

9:21 a.m.
Well, the event is scheduled from 9:00 to 11:00, and the breakfasts were just served. So, we seem to be looking at an hour or so presentation shared by four panelists. Even if the congressman fights for equal time, that's a total of about 15 minutes in the hot seat. We probably shouldn't expect much depth.
9:36 a.m.
The event proper has begun, with the AARP moderator Kathleen S. Connell, Senior State Director, AARP-Rhode Island. Each speaker will make a presentation, and then questions will be accepted, at first in written form from the tables.


9:49 a.m.
Kennedy's staff should expend some effort to teaching him to adjust his speaking tone depending on setting. He's shouting at us like it's a potentially hostile audience, although I suppose it's fitting, inasmuch as he's throwing the world of politics at the issue: "This bill is not just about healthcare. It's about..." everything from peace of mind to homeland security.
"YOU'RE ALREADY PAYING FOR THE UNINSURED!"
The high price of healthcare is apparently the fault of uninsured asthmatics who use the emergency room for care.
9:53 a.m.
America needs the government to step in and get primary care doctors to coordinate all of the patient's care. See, without federal mandate, doctors just don't do that sort of thing.
"ONE-THIRD OF YOUR HEALTHCARE DOLLAR DOES NOT EVEN GO TO HEALTHCARE DELIVERY!" "That's a crime and we shouldn't allow it to continue."
Although, he just said that four-fifths of "your healthcare dollar" goes to 20% of healthcare consumers.
9:56 a.m.
And yet, doctors support the Democrats' reform 3 to 1 because... they're tired of paperwork.
10:00 a.m.
"Do you want the public, through the members of congress to be the ones who regulate healtcare, or do you trust the private insurance companies? They are accountable to stock holders and boards of directors. The public option is accountable to the public."
Hey, he's got a point. If the public is paying the bill, and the healthcare system is accountable to a representative democracy, the payer won't have to worry about customer backlash if it's got political cover for such things as, say, rationing.
10:01 a.m.
Kennedy: It's all paid for through efficiencies and other obvious savings. Defensive medicine, etc .
Why not save all that money first and then move to expand the government involvement?
10:04 a.m.
We need a public option because the current system doesn't treat people as anything other than a monetary unit, and the government would see them as people. (Or, you know, voting units and campaign donation units, but we'll put that aside.)
Kennedy just complained that his friends call him up from emergency rooms all the time so he'll come down and get them special handling. On the fact that powerful folks get special treatment: "That's morally outrageous, and that's the country we live in right now."
Bad, materialistic America.
10:09 a.m.
By the way, to put a face to the journalism, this is Steve Peoples:

10:13 a.m.
Kennedy's done. Ann Gardella is speaking. Congressman Langevin just arrived.
10:15 a.m.
Tivertonian Dr. Nick Tsiongas is up.
10:17 a.m.
Mr. Tsiongas related the story that his parents recently visited and suggested that he ought to take down the healthcare reform political sign he's put on his Main St. property. Everybody who receives healthcare should be "afraid" if this reform doesn't pass; reference to Churchill's line about Americans always doing the right thing... after they've tried everything else.
Bad, backward-looking America.
10:22 a.m.
Donna Policastro is up. She's pleased that this issue has brought the R.I. State Nurses Association together with the SEIU and Ocean State Action.
Nurses are tired of working so hard to make the healthcare system work for their patients. I wonder if Congressman Kennedy would position that in contrast to those primary care doctors who don't help their patients coordinate their various specialists.
10:29 a.m.
Langevin is wired with a mic, and he's going to get a turn to speak.
10:31 a.m.

10:34 a.m.
Q&A time (read off cards).
By the way, Langevin mentioned the unsustainable trends in premium costs. The argument brings to mind a graphic that reader Roland Benjamin emailed me the other day:
<
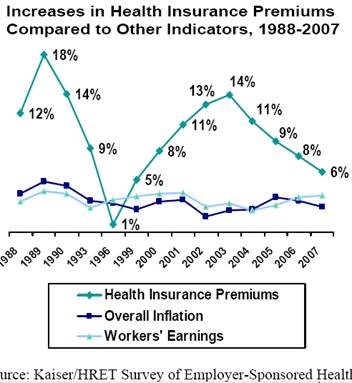
The big dip in 2003 follows the introduction of healthcare savings accounts.
10:47 a.m.
Interesting collision of issues: Ms. Policastro is talking about the coming shortage of nurses, and she cited the problem that many potential nurses get a year or two into their education and realize that there's more hard science than they'd expected, her conclusion being that high school and lower education has to improve.
Amen to that, for a multitude of reasons. Of course, the solution of the sorts of people populating this room is to flow more money to the problems, which happily benefits their friends in labor unions and other public-sector-related organizations. I suspect I'm not alone on the other side in believing that that solution is the problem.
10:53 a.m.
Kennedy's redirected to his push for more money and requirements for care, which will benefit those who provide care ("NO COPAY!" for screening procedures). Eventually, it comes down to taking money from some Americans to give it to others. Everything in between is quibbling about the "who" and in what form.
10:59 a.m.
Tsiongas just put the difference in practical philosophical approaches to the issue of healthcare: He wants to take "all of the money" currently constituting the healthcare system — consumers, unions, providers, insurers — and put it all together in one pile "so we can make better decisions."
How can such folks not see the clear consequence of that sort of consolidation? Defining the "we" who will make the decisions becomes a huge battlefield. Let's assume the pure motives of Mr. Tsiongas and everybody else who currently advocates his position. By what mechanism do the Tsiongasians intend to keep control of the decision making process? And to the extent that they create those mechanisms, why should we trust them to have that expanding power?
11:04 a.m.
Kennedy: "If the insurance companies and everybody is so good at lowering prices and finding efficiencies, why aren't they doing it?" Umm. Government mandates, requirements, and regulations.
11:11 a.m.
Moderator Kathleen Connell called for a round of applause for the press for coming out on a Saturday. Curious.
11:15 a.m.
Steve Peoples started to ask me my thoughts on the event but had to run after Kennedy for a comment. For the benefit of all media types who may want the right-wing opinion (as filtered through my potpourri of philosophical and personal inputs) should feel free to call or email or, you know, just read the above...
ADDENDUM:
I've posted the video from the event here.
September 24, 2009
Contrasting Healthcare Fora
I've just received word that I will be allowed to do my liveblogging, YouTubing thing at Congressman Patrick Kennedy's limited-attendance healthcare forum, on Saturday. We can then compare and contrast the candidate, audience, and message with State Representative John Loughlin's healthcare town hall meeting in Tiverton on Wednesday.
Roland Benjamin: A Response to RI Health Care Experts
The Providence Journal reported the responses of health care experts around the state to President Obama's speech on reform to Congress a few weeks ago:
Five Rhode Islanders with expertise in health care were among the many who watched President Obama's speech Wednesday night. A professor, a doctor, a hospital president, a businessman and a government official each offer a unique perspective…
Most of the responses in one way or another commended the President on his efforts to transform our health care system. With one exception, though, they seemed skeptical about the upside to the details.
For many individuals, inflation of care and plan costs is of paramount concern. The nonstandard inflation in health costs has eroded coverage as insurance prices push individuals out of the market. That said, two of the experts are not convinced that ideas will do anything in this regard.
Rhode Island Health Insurance Commissioner Chris Koller states:
Nothing in the president's proposal last night directly gets at changes in the way we use medical care services, which are what's driving our cost increases.
And Chairman of the Rhode Island chapter of the Smaller Business Association of New England Grafton Willey is concerned that businesses would pick up the price tag:
Mr. Obama said it would not be funded through tax hikes, but Willey worries that small businesses could end up paying.
If costs are to be contained, and there is only marginal indication that this is a goal of the reform, two other experts hint from where cuts will come.
The President of South County Hospital, Lou Giancola, expressed concerns that providers will bear this burden.
Giancola worries that cost control, as often happens, will come down to simply paying providers less. Reductions in Medicare reimbursements have already been proposed…
Professor James Munroe at Brown University, a political science expert and coauthor of a new health care reform book, offers little relief to the concerns of the provider community with a more pragmatic reality check on how cost containment might be achieved.
Once everyone is insured and the government is at risk for the costs, he said, the government will clamp down — by paying less to providers.
So the Rhode Island experts agree that either costs will continue to rise, requiring a necessary tax or premium increase, or providers will pay through diminishing reimbursements, ultimately affecting quality of care. But if the reforms are not designed to contain costs, where is the upside? Naturally, the ambiguous goal of insuring the uninsured might be coercively achieved, by requiring millions who do not see the value of insurance to buy it. But that is a revenue grab to force tens of millions of folks who already have access to insurance, but choose not to pay for it, to fork over their resources for the common good.
Beyond insuring the uninsured, the president promised to provide more consumer protections for those already covered. Commissioner Koller acknowledged that much of these reform elements already exist in the State:
Most of the insurance reforms that President Obama is proposing in his health-care plan, such as bans on preexisting-condition exclusion, are already part of Rhode Island law, Koller said. The state has a robust set of consumer protections passed by the legislature over the years.
This probably has little correlation to the fact that Rhode Island has higher family plan premiums than 42 other states and is only 3% less than the highest premiums in the country. Ask any employer whether these consumer protections have contained premium inflation rates.
The one Rhode Island expert that was completely supportive was Dr. Elizabeth Lange, President of the Rhode Island chapter of the American Academy of Pediatrics. She marginalized the opinions of those outside of the health field:
"I don't think nonmedical people understand what a crisis the system is in," Lange said. "What we're doing now is unsustainable. We have to make a change."
Of course, doctors, hospitals and pharmaceutical companies are on the receiving end of a vast majority of dollars pumped through the insurance process. The natural tendency of these groups is to protect what they have. Mr. Giancola is obviously cognizant of that and Dr. Lange seems more the purist in her beliefs that expanding primary care to everyone will make for a better society. In both instances, there is a bias towards increasing cost without any increase in overall quality care.
Once again, the true failure of the reform debate comes in the diagnosis of the problem. The patient is virtually completely insulated from the direct financing of health care purchases. This by itself has produced the unnatural inflation that has made much of health care, and now insurance premiums, unaffordable. Regardless of payer, reform that diminishes this insulation is the only path to cost containment that coincides with quality improvements.
Consumer Driven Health Plans do just that. A May compilation analysis from the American Academy of Actuaries found the following:
- First year savings of CDH implementation of 12% to 20% compared to traditional plan offerings.
- Inflation trends after the first year run 3% to 5% less than traditional plans. i.e. Normal inflation.
- All of the studies show increases in preventative services and most showed that participants were as or more likely to follow recommended care for chronic conditions while providers were more likely to follow evidence based protocols. i.e. Better quality of care.
- Premium cost shifting from employer to employee is not incurring. i.e. Employers are forwarding premium savings from higher deductible plans directly to the employees.
These real numbers are the exact results needed from reform, but the ideological left will not acknowledge these solutions. Our own Senator does not understand that premium savings fund health care spending. In Wednesday's speech, our President promised to "place a limit on how much you can be charged for out-of-pocket expenses". Both comments reveal fundamental misrepresentations of economics and health care. And in a study published in the American Journal of Managed Care last year, [emphasis mine]
…on a mail-in survey of 528 physicians… less than half (48 percent) said they felt ready to discuss medical budgets with patients, and 43 percent said they had little knowledge of how consumer-driven health plans work. About one-third said they had scant understanding of how health savings accounts function.
So it should be little surprise that Dr. Lange, Rhode Island's own primary care expert, does not see the value in consumers playing a role in their own health care financing:
If you have a plan with a $5,000 deductible, Lange said, "That makes you essentially uninsured as well. You're not going to be seeking medical care."
Of course, I know plenty of people with deductibles that high. This includes my family with a plan I chose deliberately. I had an appointment with my primary care physician last week. I have never had a better relationship with my children's pediatrician, nor have I spent as much with her. Anecdotally, I can give you dozens of examples that directly contradict what Dr. Lange believes. Empirically, the studies analyzed by the Academy of Actuaries contradict Dr. Lange's belief with significant data.
The real solution is to encourage a migration of health care financing to individuals. This is already being done and must be enhanced through tax policy. But when some of the stakeholders do not understand the basic economics of the solution, the ideas get pushed off the table. Couple this with the ideologically dominant progressive Democrats calling the shots, an idea that strays towards individual liberty is about as likely as the left extending the 2001 and 2003 tax cuts.
September 22, 2009
Taxing on Your Health
Periodically, I catch an episode of The Mentalist, in which a non-cop, always-right, psychiatrist-type character assists the police with their cases. One episode featured the actor who played Chip on Kate and Allie, who — if I may indulge in a spoiler — played a murderer who had spent years posing as a mentally handicapped fixture of the town.
The memorable moment came when the mentalist had figured the case out (based on the not-so-subtle clue that Chip had a well-worn copy of Moby Dick in his trailer) and was trying to draw him out of his facade in the interrogation room. "Come on. I see you," he said. That's how one begins to feel about long-running political debates.
Come on. We can be honest, now. Is there anybody who doesn't anticipate where this is going?
The tax [on "Cadillac" healthcare benefits] is meant to raise more than a quarter of the $774 billion needed to pay for the Baucus plan. But, just as much, the tax is intended to discourage the overly generous coverage that many experts say has helped fuel the country's reckless spending on medical care.As it turns out, though, many smaller fish would get caught in Baucus' tax net. The supposedly Cadillac insurance policies include some that cover many of the nation's firefighters, coal miners and older employees at small businesses -- a whole gamut that runs from janitors to college professors, from union shops to Main Street entrepreneurs.
The net will catch more people than initially explained. Folks will begin taking their pay and benefits in a different form. Loopholes will emerge. And the government will have to find a way to come up with even more money to supplement the tax-the-rich shortfall. It's too obvious not to be incorporated into the Democrats' plan, even if only as a problem to address later, once the deal is sealed.
We need a national political mentalist to coax our leaders through the facade of their double-speak.
Union and Democrat Party, Speaking with One Voice
This past weekend's episode of Newsmakers, with AFL-CIO RI President George Nee, is worth a watch:
Nee is among the more reasonable-sounding of the labor representatives, but that presentation only emphasizes the absence of space between how he responds to questions and how any given Democrat partisan would answer them. Sure, he's the guy who said that the state needs more political competition between the parties, but some Democrats have said the same thing, and there's an underlying insinuation that the Republicans should become more like Democrats and, for one thing, court labor more enthusiastically.
His take on a "public option" in healthcare, for example, comes directly from a conversation with Senator Sheldon Whitehouse: He cites public universities as an example thereof. Perhaps to the extent that "public" means "union jobs," the comparison has some validity, but in practice the two structures are substantially different. Notably, public universities are state-level operations, not federal.
More importantly, though, universities hire professors and not only put course offerings together, but fulfill them, as well. Health insurance is almost purely a matter of paper processing and funding. "Public option" doctors would not be competing with private-sector doctors to offer a more attractive healthcare regimen. Moreover, given the location-specific nature of higher education, translating such a thing into healthcare would represent a dramatic restructuring — with clients having to travel to a central healthcare campus, or the government seeking to place its doctors in every community.
Federal and state governments also have not built a web of regulations and mandates for higher education. Apart from accreditation and general business laws, colleges and universities operate under their own directives, which allows actual competition. In healthcare, so many offerings are explicitly required, and the incentives guiding the means of payment are so heavily manipulated, that the entire system is effectively becoming a "public option."
Somehow, I suspect that Nee, like any partisan Democrat, would not extend the principle of competition — which the left is happy to extol under the currently restrictive circumstances — if it meant permitting citizens to purchase plans more freely and companies to offer a greater variety.
September 21, 2009
Medicaid as Boomer Inheritance Program?
Stephen Moses, Health Care Policy Fellow for the Ocean State Policy Research Institute, brings to light an easy to miss loss of state dollars:
In 1993, the federal government made it mandatory for state Medicaid programs to recover the cost of benefits paid to older people with exempt (sheltered) assets out of their estates. In research I conducted for the Health Care Financing Administration in 1988, we found that Oregon, for example, recovered 5.2 percent of its Medicaid nursing-home expenditures from the estates of deceased recipients.The comparable number for Rhode Island is only .67 percent. In other words, Rhode Island, which recovered only $2 million last year from estates, is leaving over $13 million on the table by not pursuing this non-tax resource more vigilantly.
Whoa! Wait a minute. Isn’t estate recovery like "picking the bones of the elderly"?
Not at all. With very generous income- and asset-eligibility rules, easy ways to self-impoverish and little estate recovery, Rhode Island's Medicaid long-term care program has become, in effect, free inheritance insurance for Baby Boomer heirs. Is that really how Ocean Staters want to use their scarce public-welfare resources?
I remain in the starve-the-beast camp, but there are other sectors of the population that could make better use of this break.
September 20, 2009
The Distressing Versus the Frightening
The rapid transformation of this country into a European-style socialist democracy is certainly distressing. American life is on its way to becoming more difficult and less free, less innovative — in a word, less American. But it is the combination of that atrophy with the existence of nations seeking to duplicate the international accomplishment of the United States (a global sphere of influence, if you will) without adhering to its methods.
More specifically, it is the combination of a strong-handed government at home with a weak-kneed government on the international scene:
The U.S. Defense Secretary is already on record as opposing an Israeli strike. If it happens, every thug state around the globe will understand the subtext — that, aside from a tiny strip of land on the east bank of the Jordan, every other advanced society on earth is content to depend for its security on the kindness of strangers.Some of them very strange. Kim Jong-Il wouldn't really let fly at South Korea or Japan, would he? Even if some quasi-Talibanny types wound up sitting on Pakistan's nuclear arsenal, they wouldn't really do anything with them, would they? Okay, Putin can be a bit heavy-handed when dealing with Eastern Europe, and his definition of "Eastern" seems to stretch ever farther west, but he's not going to be sending the tanks back into Prague and Budapest, is he? I mean, c'mon . . .
September 16, 2009
Ignorance, Arrogance, and Deceit
I suppose I lack the grounds to object to Robert Whitcomb's protestations in yesterday's Providence Journal (not online) that his experience living in France doesn't jibe with the warnings that he hears fellow Americans giving against socialized medicine:
The ignorance and dishonesty in the U.S. health-care debate are beyond belief. ...Then there are the idiotic observations about other developed nations' health-care systems. ... In fact, there is far more red tape and bureaucracy in the American health-care "system" than in countries with universal coverage, as there is in our tax "code."
Inasmuch as Whitcomb doesn't cite any idiots in particular, one cannot address the relevance of his French experience or specific claims about red tape. (And I'll resist the temptation to make populist appeals to my fellow gauche Americans qui n'est pas comme il faut. But a logical fallacy has the same repercussions no matter the language or airplane hours logged:
Consider how some people loudly worry that their taxes will go up if the government covers more people, while never noting how much their premiums for for-profit insurance go up 7 to 10 percent a year. Would they rather pay 7 to 10 percent a year to, say, United Healthcare or 3 percent annual increases to pay for Medicare for all? Test scores often show how badly Americans do in math, b ut this innumeracy is amazing.
Whitcomb conveniently sidesteps the reality that the debate is over how to reform healthcare, not whether to do so. The dilemma is false. Obviously so. Amazingly so. And it raises questions about how much readers should consider Whitcomb's other points persuasive, lacking, as I've said, any particulars that one could address beyond Robert's own personal experiences at some unidentified time in the past with an unspecified segment of the French healthcare system.
Wyden Criticizes the Democratic Health Reform Product
Given his long record interest on the subject (which Anchor Rising was reporting on before reporting on the details of healthcare reform was a big thing in the blogosphere), Oregon Senator Ron Wyden's (D - Oregon) strong skepticism about Democratic healthcare reform plans is a potentially significant development.
From an article posted last night at the Oregonian newspaper's website…
The Senate's leading health care proposal is seriously flawed, Oregon Sen. Ron Wyden said Tuesday, declaring that it fails to fulfill President Barack Obama's primary reforms and could force millions of Americans to pay more for the medical care they receive."Under this bill as it is written now, more than 200 million Americans would not get choices like the president of the United States called for," Wyden said in an interview. "Middle-class people certainly will pay more, based on the draft we're seeing."
September 14, 2009
What Are They Investing In?
This graphic showing the stock gains made by six health insurance companies after President Obama's healthcare speech is interesting fuel for contemplation. What is it that has attracted investors' interest?
- The possibility that health insurers are moving toward becoming another category of government-backed business?
- The possibility that consumers will rush to acquire plans that will be grandfathered into the healthcare "reform" (if only for a few years)?
- The likelihood that the Democrats' plan will accomplish nothing so effectively as preserving the dominance of a handful of leading corporations
Now Democrats Want to Tax Artificial Hips to Pay for Healthcare
Blogger "Tigerhawk" is reporting on a proposal by Senate Democrats to raise taxes on medical devices to pay for their healthcare reform plans (h/t Instapundit)...
Senate Democrats are proposing [to levy] a "value added tax" on medical device companies according to their proportion of U.S. sales. This tax would be without regard to profitability, so it would amount to a capital tax on start-ups and a massive income tax surcharge on profitable companies, varying as net margins do.Tigerhawk ultimately describes the plan as an excise tax. The New York Times' Prescriptions blog, on the other hand, refers to "fees" and "givebacks" in its description of the the plan...
The future of Senator Max Baucus’s compromise health care proposal is far from certain, but one industry group was quick to fire back on Tuesday. The protest came from makers of medical devices like heart pacemakers and artificialhips – companies that would have to pay hefty new fees under the Baucus plan.And, by the way, it's the Times article that's the source of the title of this post, for anyone who thinks it's unfair.In an interview, Stephen J. Ubl, the president and chief executive of the Advanced Medical Technology Association, a trade group, said the organization opposed the proposal’s call for annual givebacks from device makers. The fees, which the proposal says would be allocated on the basis of each company’s market share, would total $4 billion a year.
“We do strongly oppose the $4 billion tax, which we believe is a tax on medical progress,” Mr. Ubl said.
One question brought to mind by the Times' reporting is if this actually is a "giveback", then what have medical device makers been taking that they're being asked to give back? The answer, also from the Times article, doesn't seem to be anything more than payment for their products; the government wants the manufacturers to give some of that money back, because some of their customers are hospitals, and hospitals are reimbursed by Medicare...
For lawmakers, some form of tax-like fees might be the only way to extract givebacks from device makers because of the way such companies are reimbursed. Government-financed programs like Medicare do not pay directly for medical devices, but instead reimburse hospitals and other providers for the procedures in which they are used.So, if you deal with someone who takes money from the government, anything the government wants to take from you is now a "giveback", and raising taxes on someone can be justified by the fact that they don't take subsidies!
Based upon what the Times has presented (I leave it to the reader to determine the reliability of the source), the Democrats' reasoning is that because a big government program reimburses hospitals, taxes have to be raised on non-hospitals, so the government can take back part of what's been given to hospitals, so the government will be able via new subsidies to give more money to hospitals. But it is a bit difficult to see how raising taxes on medical devices, including things like pacemakers and artificial hips, will contribute to either lowering healthcare costs or raising the quality of medical care.
Call me a cynic, but I think that this scheme pretty well represents the quality of economic thought that's going into Democratic health reform plans.
September 10, 2009
A Quick Philosophical Point on Rights
Something resonated oddly for me, the other day, and it occurred to me that there's an important philosophical point to be made in response:
"What we can be proud of in Europe is the ground rules, that everyone has the right to health care," said Jose Martin-Moreno, a health expert at the University of Valencia in Spain. "But the implementation has been difficult and one size does not fit all."
We've gotten a bit too free, in the West, with the "rights" language over the past few decades, to the point that it's easy to slide within the same word choices from nice privileges that we'd like to provide in an ideal world to irreducible allowances that governments simply cannot take away. That's truly a detriment to language and a loss to social discourse.
So plainly put: Is there a right to healthcare? Well, compare it with other rights:
- With the right to free speech, we have a right to speak, but not to be heard.
- With the right to bear arms, we have a right to own and operate guns, but not to be given guns for free.
In these terms, we would have the right to procure healthcare, but not to have it provided to us, to an extent of our own or somebody else's determination.
Why Subsidize-And-Regulate Isn't Enough to Fix Healthcare
For another perspective on why plans that focus on Federalizing the regulation of and providing subsidies to the existing employer-based healthcare system aren't likely to be an effective pathway to reform, David Goldhill's article in September's Atlantic Monthly is worth reading. In the opening section of his article, Goldhill writes…
The persistence of bad industry practices—from long lines at the doctor’s office to ever-rising prices to astonishing numbers of preventable deaths—seems beyond all normal logic, and must have an underlying cause. There needs to be a business reason why an industry, year in and year out, would be able to get away with poor customer service, unaffordable prices, and uneven results—a reason my father and so many others are unnecessarily killed.Based on Goldhill's description of the problem, allow me to re-iterate a question I posed at the beginning of this year's town hall season: could supporters of the President's healthcare reform framework provide a few examples to use as a model from economic history where Federalizing regulation, providing subsidies, and mandating spending has brought down the cost of something, while solving the multiple irrationalities that Goldhill describes?Like every grieving family member, I looked for someone to blame for my father’s death. But my dad’s doctors weren’t incompetent—on the contrary, his hospital physicians were smart, thoughtful, and hard-working. Nor is he dead because of indifferent nursing—without exception, his nurses were dedicated and compassionate. Nor from financial limitations—he was a Medicare patient, and the issue of expense was never once raised. There were no greedy pharmaceutical companies, evil health insurers, or other popular villains in his particular tragedy.
Indeed, I suspect that our collective search for villains—for someone to blame—has distracted us and our political leaders from addressing the fundamental causes of our nation’s health-care crisis. All of the actors in health care—from doctors to insurers to pharmaceutical companies—work in a heavily regulated, massively subsidized industry full of structural distortions. They all want to serve patients well. But they also all behave rationally in response to the economic incentives those distortions create. Accidentally, but relentlessly, America has built a health-care system with incentives that inexorably generate terrible and perverse results. Incentives that emphasize health care over any other aspect of health and well-being. That emphasize treatment over prevention. That disguise true costs. That favor complexity, and discourage transparent competition based on price or quality. That result in a generational pyramid scheme rather than sustainable financing. And that—most important—remove consumers from our irreplaceable role as the ultimate ensurer of value.
Gotta Have Humor on Healthcare
Both of us being giddy with anticipation prior to the president speech last night, my conversation with the host of the Matt Allen Show was full of sarcasm and laughter, which strikes me as the only appropriate posture to the current situation. Stream by clicking here, or download it.
Oh, by the way, the person who called out "You lie!" — causing a very interesting moment in the speech #&151; when the president declared that no illegal immigrants would receive taxpayer-financed healthcare under his plan was Republican South Carolina Representative Joe Wilson. The Associated Press tsks at the "nastiness" of the moment, but if that's the gauge, there were plenty of moments of nastiness in the speech itself.
September 9, 2009
Health Care Reform - Onto a Tabula Not So Rasa
Under "Liveblogging the President's Healthcare Speech", Justin comments
It's almost nauseating to hear politicians argue for a "public option" on the basis that competition is so limited, when the reason is clearly government regulation and mandates.
This is an excellent point also raised recently by Andrew. Health care reform is being designed not upon the clean slate of a health care system operating under purely market conditions but upon layers of regulations built up over several decades - and not all were promulgated to advance the best interest of the consumer/patient.
Let me hasten to add here that I would be dubious at best of a health care system that operated under pure market conditions completely without regulation. But isn't it also possible to have too much of a good thing?
If, indeed, the goal is more competitive (stipulating for a moment that 1,200 insurance companies do not engender sufficient competition) and less expensive health care coverage, perhaps the best reform would be the modification or elimination of some existing regulations, not the addition of another layer.
Two items that come most readily to mind are tort reform and elimination of the barrier to buying health insurance across state lines, though the list certainly does not end there. This approach, happily, would also conform to President Obama's stated desire not to "accept the status quo as a solution". The change created by taking a red pen to certain sections of our health care law could be just as drastic as appending chapters to it.
Liveblogging the President's Healthcare Speech
We'll be using the comments section of this post to liveblog the president's speech to Congress on healthcare. Based on the information currently provided it looks like we're in for a guilt campaign that attempts to change the aesthetics of the debate without doing much to modify the substance. People are suffering. We must work together. The basic outline of the Democrats' plan is the only solution, and any attempt to suggest otherwise is merely divisive greed.
When I called in to his show, at the turn of the hour, Matt Allen quoted this excerpt from the speech:
Everyone in this room knows what will happen if we do nothing. Our deficit will grow. More families will go bankrupt. More businesses will close. More Americans will lose their coverage when they are sick and need it most. And more will die as a result. We know these things to be true.
As I told Matt, this is merely another example of the President striving the conquer the Politics of Fear with the Politics of Hope.
One simple question and then some reflections
In advance of President Obama's speech tonight about healthcare, I have one simple question -
If a government-run option is such a good idea for all of the rest of us, why do Obama and the Congress refuse to sign up for it themselves?
On a related note, Ponnuru discusses the Left's disregard for truth.
Glenn Reynolds links to Martin Feldstein and adds his own comments:
"The higher taxes, debt payments and interest rates needed to pay for health reform mean lower living standards." But lower living standards for you are a small price to pay in exchange for more power for the political class — whose living standards won’t be going down at all...
All of which is what the American people have instinctively figured out. Just like we have throughout history.
Camille Paglia, an Obama supporter, writes about the divide:
...Why did it take so long for Democrats to realize that this year's tea party and town hall uprisings were a genuine barometer of widespread public discontent and not simply a staged scenario by kooks and conspirators? First of all, too many political analysts still think that network and cable TV chat shows are the central forums of national debate. But the truly transformative political energy is coming from talk radio and the Web — both of which Democrat-sponsored proposals have threatened to stifle, in defiance of freedom of speech guarantees in the Bill of Rights...Why has the Democratic Party become so arrogantly detached from ordinary Americans? Though they claim to speak for the poor and dispossessed, Democrats have increasingly become the party of an upper-middle-class professional elite, top-heavy with journalists, academics and lawyers (one reason for the hypocritical absence of tort reform in the healthcare bills). Weirdly, given their worship of highly individualistic, secularized self-actualization, such professionals are as a whole amazingly credulous these days about big-government solutions to every social problem. They see no danger in expanding government authority and intrusive, wasteful bureaucracy. This is, I submit, a stunning turn away from the anti-authority and anti-establishment principles of authentic 1960s leftism.
How has "liberty" become the inspirational code word of conservatives rather than liberals?...I always thought that the Democratic Party is the freedom party — but I must be living in the nostalgic past...
Meanwhile, all of these developments have occurred while the Republican party has been comatose on policy ideas.
September 8, 2009
Quick Clarity on Health Care Debate
Congress is back after a 40 day recess. A lot has happened--namely, bi-partisan "comprehensive health care reform" looks dead--but there will be much discussion over the next few weeks. The Washington Post (h/t) oofers a summary and preview, including this helpful bit from Republican Congressman Mike Pence:
House Republicans, who held hundreds of their own town hall meetings that drew more than 100,000 voters, according to preliminary estimates, viewed the break as a galvanizing moment for opposition to the Democratic legislation. "I heard people saying, 'Look, we need health-care reform. We need to do something to lower the cost of health insurance for families and small businesses and lower the cost of health care,' " said Rep. Mike Pence (Ind.), the third-ranking GOP leader. "But I also heard people say that they don't want a government-run plan that is going to lead to a government takeover of health care."It's an important point. For all the sturm und drang we've seen at the town hall meetings, what was missing was an explanation that those on all sides (not "both", there are more than two options out there) of the issue think something needs to be done.
September 7, 2009
Rationality and Rationing
Michael Kinsley has argued that, when it comes to rationing, healthcare reform would only make explicit something that the system does inherently:
In practice, people die all the time because some effective treatment is too expensive. But whenever an issue gets drawn into the political system and becomes explicit, it becomes harder. That is what health-care reform will do to the question of rationing. ...... The easiest way to raise your averages -- maybe even the best way, if we're being honest -- is to concentrate on the general level of care and not to squander a lot on long-odds cases. But if the long-odds case is you or a family member, you may well feel differently. ...
Here is a handy-dandy way to determine whether the failure to order some exam or treatment constitutes rationing: If the patient were the president, would he get it? If he'd get it and you wouldn't, it's rationing.
To some extent, Kinsley is correct to remind us that the inhumane error is sometimes easier. It's easier to fault chance for outcomes that we failed to avoid. Seeking to address a question that will not go without answer, one way or another, exposes, rather than introduces, our own personal responsibility. But that doesn't mean that we are right to claim responsibility in every situation.
In my view, "rationing" requires a deliberate decision not to provide something with resources under the group's control. Rich folks and presidents will always possess resources beyond a medical system's control, so in that sense, the only way to eliminate "rationing" (by Kinsley's definition) would be to ensure that additional services are not available. An individual's willingness to pay for a particular test, pill, or procedure ultimately sets its worth in the only way that is adequately humane, and because tests, pills, and procedures have absolute costs, wealthy people will have a higher threshold for "must-haves." Poor people's thresholds will often prove to be lower than a moral society should prefer.
It might be possible, in theory, to devise a formula to adjust the equation for individuals such that each expense requires roughly equivalent judgment. In essence, the cost of a procedure would translate into a percentage of personal income and worth: a man worth twenty grand would pay $1,000, while a man worth twenty mil. would pay $1,000,000. The impossibility of making such a system workable should be plain to see. Not only would the wealthy have incentive to opt out of the system, in one way or another, but the society must invest some body with authoritarian redistributive power, making the cure worse than the disease (not the least because the wealthy would inevitably have imbalanced influence).
I wouldn't presume, at this point, to put forward the formulas and guidelines that a fully reformed medical system should follow, but it seems to me that the general principles would not be new. Let people pay for most services as they go, carrying insurance as they choose for life's unpredictables, and let other people form groups and pool money to help as morality requires. There's a bit of trusting in the wind to lift our wings, in such a plan, but I truly believe the outcome would be better when judged by socially holistic criteria.
We simply don't see the ripples of our decisions in the public sphere, but the bigger and faster the man-made vessel that we place in the water, the more extensive, and detrimental, those ripples can be — and the more critical control over the steering becomes.
September 5, 2009
How Would Government Healthcare Address This?
I have yet to hear back from Congressman Patrick Kennedy's office regarding my inquiry about the meaning of "screening" when it comes to mental illness and addiction, with specific reference to an amendment to the healthcare "reform" bill in the House. Sometimes, though, when you've this sort of thought filed in the back of your mind, relevant examples emerge, as if of their own volition.
Such is the case with findings related to childhood depression:
Depression in children as young as 3 is real and not just a passing grumpy mood, according to provocative new research.The study is billed as the first to show major depression can be chronic even in very young children, contrary to the stereotype of the happy-go-lucky preschooler.
What sort of preventative measures might be taken, in light of this information, were the government financially interested in controlling costs? The question drifts into creepy (even terrifying) ground pretty quickly:
Depression was most common in children whose mothers were also depressed or had other mood disorders, and among those who had experienced a traumatic event, such as the death of a parent or physical or sexual abuse.
If an event in a child's life should trigger red flags in a screening process, a treacherous path exists for the government to assert its authority as implicit medical caregiver. Drugs. Institutional care. Restrictions and mandates on parents and family members.
There's a risk of letting one's imagination run too wild, here, but blending our culture's increasing social liberalism with a clinical view of psychological and spiritual well-being and a government-directed healthcare system makes for a dangerous, dangerous cocktail.
Concern About the Swine Flu Crisis Mode
Does anybody else see imaginary warning signs whenever news media convey urgency related to the swine flu and its predicted resurgence with the resumption of school? Parents and non-parents alike do well to pay attention to developments on the H1N1 front, but before leaping onto the latest and greatest protections, all should seek context like this:
It is not clear whether the new virus is more dangerous than ordinary seasonal flu for children, though some health officials suspect it is. ...Swine flu was first identified in April and is now responsible for almost all flu cases in the United States. It has caused more than 1 million illnesses so far, though most were mild and not reported, the CDC estimates. More than 550 lab-confirmed deaths and 8,800 hospitalizations have been reported.
Those statistics don't mean the new flu is worse than seasonal flu, which is particularly lethal to the elderly and plays a role in an estimated 36,000 deaths each year, the CDC says.
Cause for concern, yes, but anybody who declares that any particular action is necessary to halt certain death and the decimation of human society on its basis has an ulterior motive.
A Zealot's Confidence, Not an Advisor's Circumspection
Since the pre-Anchor Rising days of Dust in the Light, I've found it to be among the great puzzles of Rhode Island media that somebody is actually willing to pay Froma Harrop a living wage to write political opinion pieces. The young writer might be tempted to find encouragement in the apparent height of the bar, but he or she should not fail to recall that the rules vary by ideology, among other things.
With the escalation of the healthcare debate, Harrop has been helpfully reminding me why it was that I gradually came to find my time better spent elsewise than trying to sort through her sentences in search of something that might profitably be raised in discussion. I recently noted her apparent inability to understand why there's any left-right controversy over the currently floating healtcare "reforms" at all. In a subsequent offering, Harrop seems immune to suspicions of risk; that is, the question of whether the proposed regime will work never enters her argument:
On Nov. 2, 2010, voters will not be asking, "What's in it for me?" They'll already know.And consider how voters would feel if there were well-designed health reform. The uninsured would be delighted, of course. But that newfound sense of security would have spread to Americans covered through a workplace: A lost job would no longer leave their families vulnerable in a medical crisis.
Older people would see that nothing they care about in Medicare has changed. They might even find themselves enjoying new benefits included in current legislation: a gradual phasing-out of the drug benefit's "doughnut hole" and no co-payments or deductibles for colonoscopies and other preventive-care screenings.
Employers might already be observing their health-insurance premiums moderating, thanks to more efficient delivery of care. And their workers might have begun enjoying higher paychecks as the boss started to pass on those savings.
Considering that the legislation piles mandate upon unwise regulation, rather than streamlining the healthcare system and aligning incentives appropriately between user and funder, I'd say that the more likely outcome is that bosses will have begun pushing their employees onto a public option and pocketing most of the savings for themselves (perhaps to compensate for increased expenses resulting from cap 'n' trade). But the point, here, is Harrop's total lack of fear that Congress's passing anything could have a worse outcome for the country than its passing nothing. By the next election, she writes, "America will have fixed the health-care mess or it will not have," depending in binary fashion on whether the Democrats have passed a bill. The jaw-dropping insinuation is that the Democrats' style of "fixing" the economy is as sure a fix as plugging a damaged tire.
If that legislation is so masterful, I wonder, why delay various provisions and hide them from view? Why backload the costs to hit after the next presidential election? I'm inclined to see it as ignorance, rather than deceit, that guides Harrop away from the fact that Republicans hardly have to make things up to "spook" voters about the potential to lose their current healthcare. One need only read the bill, which explicitly kills grandfathered policies after five years of forced attrition.
The sentence that doesn't enter Harrop's rhetoric, though it should is: Of course, all this requires that Democrats keep their tendencies toward big-government excesses in check and actually contrive a "reform" that will work. She has an unbounded faith in liberal government agents pushing forward an increase in government control.
Far be it from me to offer the Democrats political advice, but a sense of fair play compels me to suggest that, wherever they ultimately seek guidance, Froma Harrop's columns would be a sweet-tasting laxative formulated to kick into effect at precisely the wrong moment.
September 4, 2009
The Appearance of Free Stuff
Could it all be as simple as getting folks to think through their arguments? That's an encouraging thought, but probably overly optimistic. Consider (emphasis added):
In Amsterdam, where I spend part of the year, every time I go the pharmacy and take out cash to pay for a prescription, the pharmacist and all the well-insured customers who never seem to pay for anything watch me like I've pulled a frog out my pocket. Then the pharmacist looks at me and my money with pity and says, "Oh, you're American." She doesn't elaborate.
Appearances can be deceiving. Frida Ghitis's observation of Europeans' government-induced delusion is of a piece with Senator Whitehouse's remark that government healthcare takes a cost burden from the shoulders of European businesses. I'd suggest that, whatever they may believe along the leading edge of Western Culture's decline, Americans should be proud that they are resistant to scammers and schemers proclaiming how easy it all could be if we'd just accept their offers to give us something for nothing.
September 3, 2009
Obama Administration Basks in Glow of "Previous Administration's" Work
I heard yesterday that the Obama Administration held a celebratory press conference about getting a couple billion dollars out of Pfizer for some thing or other. Except, as Glenn Reynold's pointed out, it was the Bush Administration that actually extracted the dough.
The pharmaceutical giant Pfizer agreed to pay $2.3 billion to settle civil and criminal allegations that it had illegally marketed its painkiller Bextra, which has been withdrawn.And then there's this:It was the largest health care fraud settlement and the largest criminal fine of any kind ever.
Although the investigation began and largely ended during the Bush administration, top Obama administration officials held a news conference on Wednesday to celebrate the settlement, thank each other for resolving it and promise more crackdowns on health fraud. {emphasis added}
Top Republican officials rarely publicized drug marketing cases or appeared during news conferences about them. Eli Lilly agreed to pay $1.4 billion over its marketing of Zyprexa, an antipsychotic, in January, before President Obama took office. The announcement was made by prosecutors in Philadelphia.Or it suggests and Administration desperate for a "win." Even if someone else got it for them.Ms. Sebelius’s decision to make the Pfizer announcement in Washington suggests that the political environment for the pharmaceutical industry has become more treacherous despite the industry’s commitment to save the government $80 billion as part of efforts to change the health care system.
Come Along on England's "Death Pathway"
I'm not sure whether or not this constitutes a "death panel," but it's certainly got the "death" part:
In a letter to The Daily Telegraph, a group of experts who care for the terminally ill claim that some patients are being wrongly judged as close to death.Under NHS guidance introduced across England to help doctors and medical staff deal with dying patients, they can then have fluid and drugs withdrawn and many are put on continuous sedation until they pass away.
But this approach can also mask the signs that their condition is improving, the experts warn. ...
"As a result a national wave of discontent is building up, as family and friends witness the denial of fluids and food to patients."
So without patient or family consent, doctors make the determination that a patient is close enough to death that they ought to spend their remaining hours under heavy sedation that might mask improvements in their condition. All that remains to do is to show them pretty pictures of mountain scenes and then ship their bodies off to the Soylent Green factory.
Mark Zaccaria, on Congressman Langevin's First Town Hall Meeting
On August 19, I attended the Town Hall Meeting called by Representative James Langevin for what was said to be an opportunity for him to gauge the pulse of his district during the summer recess.
There was little doubt in anyone’s mind that Topic A for the evening’s exchange would be the proposed changes to US healthcare now on the table. Certainly the Congressman thought that, since there was a PowerPoint presentation rolling as folks filed in to take their seats. The slides went back and forth between ideas that were characterized as myths about the healthcare legislation now pending and what were said to be facts that refuted those myths. It would be instructive to know who created that presentation. Whether it was the Congressman’s staff or some other entity in the Administration, the slides established our host’s position beyond any doubt before the meeting even began. This was not an opportunity for the congressman to listen to his constituents but a sales pitch for the legislation known as HR 3200.
The Congressman’s comments were confusing, sometimes contradictory, and at times, frightening. Of particular concern to me, and others was his statement that healthcare was too important a matter to be left to market forces and the private sector and that he did not go to Washington to vote on such important issues.
When asked if he had personally read the text of the pending legislation on healthcare he went great distances to avoid answering. In fact, he has not read any of the five competing healthcare bills now working their way through the federal legislature. But instead of saying there was no single bill on its way to an up or down vote, he used considerable time-consuming detail in his circular answer to avoid coming out with the simple truth. To me, that awkward moment spoke volumes about our current Representative’s shortcomings in the area of leadership, and had me questioning his impact within the chamber. It was abundantly clear that our Representative will do exactly what he is told to do by those in power in Congress, whether or not it’s what his constituents want.
I accept that the Congressman has not read every Whereas and Therefore in every bill to change the name of a post office or bridge in some far off state. But he himself indicated he understands that healthcare is the issue of the day so I think he should have read this one. I accept that his staff may have read all five of the current crops of these bills, but we did not elect his staff to represent us on this or any other issue. Right now Healthcare is too important a topic to delegate to staff, and far too important for our Representative not to have read HR 3200.
In answer to a question on whether or not he would vote in favor of a bill 70% of his constituents opposed I was expecting to hear a statement on how a representative Republic functions. Instead, I listened as my Rep in Congress dodged the question by saying he was actually here on a Fact Finding Mission. My translation: He’ll vote the way Nancy Pelosi tells him to, without regard to what we think.
Wearing Out the Public
Matt Allen and I touched on the legislative process on last night'sMatt Allen Show and the way in which it wears the public out as legislation moves toward law. After all this heat and energy, we still have multiple versions in the Senate over which to argue, likely with various provisions, all of which have the potential to drift out of awareness only to reemerge during conference. Stream by clicking here, or download it.
September 2, 2009
Revisiting the Wheelchair Clause
An interesting comment was just made to my August 19 post looking at strange changes to language concerning the purchase of wheelchairs that the current healthcare "reform" would make:
The supplier will no longer be able to get the lump sum payment for basic powered wheelchairs and have to wait 13 months for their 105%, it's bad for cash flow and only the largest suppliers will be willing to provide these chairs, if any. It will also push suppliers into trying to justify more expensive "complex rehabilitative power driven wheelchairs so they don't have to wait 13 months for their 5% profit.The end user gets to make this decision, by the way, and it really makes no difference to that person how the supplier makes or does not make money... until they can't find a provider because medicare reimbursement has driven everyone out of the market.
So, rather than one predictable and undesirable result of government involvement (rationing), it looks like another (market restrictions favoring large incumbents).
Langevin's Town Hall Tomorrow: A Preemptive Invitation
Below is the text of an e-mail invitation to Congressman Langevin's health care town hall in Westerly tomorrow. [Thanks to Scott Bill Hirst, a registered Republican in Hopkinton, for forwarding. I'm sure rumors that the RNC has now launched a full-blown investigation into the question of your party status, Scott, are completely exaggerated.]
I wanted to send you an urgent invitation to an important town hall with Rep. Jim Langevin this Thursday, September 3rd.He'll be talking to constituents and gathering feedback. Whether you ask a question or show your support with a sign, attending this town hall is a powerful way to show where you stand and thank those in Congress who are fighting for reform.
I hope you can join us. Here are the details:
What: Health Care Town Hall with Rep. Jim LangevinWhere: Esplanade in Wilcox Park
44 Broad St.
Westerly, RI 02891When: Thursday, September 3rd
Arrival Time: 3:30 p.m.
Start Time: 4:30 p.m.Please arrive as early as possible, and make sure that the most powerful voices in this debate are those calling for real reform, not angrily clamoring for the status quo.
RSVP here:
http://ri.barackobama.com/WesterlyTH
First of all, isn't the point of this town hall to listen to the concerns and wishes - "gathering feedback" - of constituents? Why, then, is turnout from one particular segment and not all constituents being encouraged?
Secondly, notice that the "status quo" (i.e., preservation of an excellent health care system and one that provides care that 80% of Americans are satisfied with) is cast in a negative light while reform - "real reform" - is established, without facts or reason, as the positive goal. This is reinforced by the suggestion to "thank those in Congress who are fighting for reform". Isn't this preempting both the voices of many town hall attendees as well as the debate on the underlying issue?
August 31, 2009
Practicing the Healthcare Reform Preach: House Resolution 615 and a Suggested Amendment
Last night, a friend forwarded me House Resolution 615.
Expressing the sense of the House of Representatives that Members who vote in favor of the establishment of a public, Federal Government run health insurance option are urged to forgo their right to participate in the Federal Employees Health Benefits Program (FEHBP) and agree to enroll under that public option.
Indeed, if the public option is as admirable as we are told, members of Congress should have no qualms about signing on to this resolution, which presently has fifty seventy five co-sponsors.
The bill does, however, need amplification. We'll call it the Watson Amendment.
... with the exception of Congresswoman Diane Watson, who is urged to forgo her right to participate in the Federal Employees Health Benefits Program (FEHBP), who is further urged to enroll in the Cuban health care system and to avail herself exclusively of the care received by most Cubans, but specifically not the care received by the tiny percentage of the famous and the political elite at Cuba's show clinics, clinics that have succeeded in persuading a small handful of delusionists like herself and Michael Moore that public-only health care under a Socialist/Marxist government is a perfectly adequate and acceptable option for all countries.
It is possible that final phrasing of the amendment will need to be worked out in committee ...
Bradley's Health Care "Grand Bargain" Unlikely
August has been a tough month for Team Obamacare Force and prospects look pretty grim for their version of "comprehensive" amorphous health care reform. But as current Democrat politicians are being put on notice that they are in trouble come 2010, the old Warhorses are coming out to buck up the whippersnappers and remind them that they had better keep on keepin' on and pass health care reform. One of them is former Sen. Bill Bradley. In a Saturday New York Times (h/t) piece, Bradley recalled that President Reagan's tax reform plan of 1986 required real bi-partisanship, including the willingness of both sides to give up on some closely-held policy positions.
None of this would have happened had the Reagan administration not taken on some of the Republican Party’s sacred cows — the oil and gas industry, real-estate interests and large industrial enterprises, all of which benefited disproportionately from loopholes. Similarly, the bill would never have passed had some Democrats not taken on an ingrained party orthodoxy — the belief that equity demanded higher tax rates.According to Bradley, a compromise bill could achieve two long term goals held by each party:
Since the days of Harry Truman, Democrats have wanted universal health coverage, believing that if other industrialized countries can achieve it, surely the United States can. For Democrats, universal coverage speaks to America’s sense of decency and compassion. Democrats also believe that it will lead to a healthier and more productive country.I agree with Steven Hayward: "I give it less than one chance in ten of happening." Why? As the Washington Examiner editorializes:Since the days of Ronald Reagan, Republicans have wanted legal reform, believing that our economic competitiveness is being shackled by the billions we spend annually on tort costs; an estimated 10 cents of every health care dollar paid by individuals and companies goes for litigation and defensive medicine. For Republicans, tort reform and its health care analogue, malpractice reform, speak to the goal of stronger economic growth and lower costs.
The bipartisan trade-off in a viable health care bill is obvious: Combine universal coverage with malpractice tort reform in health care.
Howard Dean proved last week at Rep. Jim Moran’s health care town hall meeting that even a veteran Washington politician can level with people once in a while. The former Vermont governor and Democratic presidential aspirant was a practicing physician before he got into politics, so perhaps we should not be surprised by his explanation for why medical malpractice caps [i.e. tort reform] is not in Obamacare: “The reason tort reform is not in the bill is because the people who wrote it did not want to take on the trial lawyers in addition to everybody else they were taking on. And that’s the plain and simple truth.” Put otherwise, trial lawyers have effectively bought themselves veto power.Maybe Hayward's estimate of the chances of a Bradley-like compromise should be revised further downward.In the ranking by OpenSecrets.org of campaign contributions by the top 100 special interests during the past 20 years, the American Association for Justice (AAJ) – formerly the Association of Trial Lawyers of America – ranks sixth overall. The AAJ is the trial lawyers’ Washington lobbying group, and 90 percent of its $30.7 million in contributions since 1989 went to Democrats. At the other end of this pay-to-play process in the nation’s capitol, AAJ has spent nearly $14 million lobbying Congress just since Democrats won control of both chambers, including $2.3 million thus far this year.
Roland Benjamin: A Saving Health Reform
It should be no surprise that great unrest arises when our representatives casually dismiss health care reform ideas that are contrary to their agenda. Senator Reed’s comment demonstrates this:
Health savings accounts — another proposal dear to conservatives — are not effective for people who have lost their jobs, Reed wrote. "In addition, with the demands facing many families today, including saving for college, there is a pressure to set aside funds for health care rather than other needs," he added.
Health savings account (HAS)-eligible health plans have achieved great progress toward the major stated goals of reform, yet the ideological left dismisses them out of hand in ways similar to the above. The HSA route provides for the highest level of individual accountability and liberty. The antithesis of the HSA, namely the public option/co-op/insurer of last resort, does the exact opposite. By leaving benefit design to elected officials and bureaucrats, the public option strips away preferences one might have as an individual buyer of insurance.
Few issues frame the ideological divide better than healthcare reform. The conservative looks to increase individual liberty, while the liberal does not believe individuals can handle that responsibility. At root, this is driving the anxiety we see in town halls across America. Most may not completely understand the details of a 1,017 page bill, but we know our liberties may be compromised in the name of reform from the ideological left.
I began this as a reply to a legitimate question posed by a commenter on Anchor Rising regarding HSAs:
So do you have an HSA? How about you folks with kids?
I have an HSA and three kids. We made the decision to switch while trying for our third child back in 2006, knowing full well that we would hit the $5,600 deductible when my wife eventually got pregnant.
I pay for the healthcare we use from the premium savings of about $4,000 per year for the plan plus approximately $2,000 in tax savings I get by pushing it through the HSA. In the three-plus years that we've had the plan, we've hit the max out of pocket in two of the years. I now have roughly $4,000 in the HSA and have saved another $800 or so in taxes that, had I chosen a more conventional plan, would have gone to United Health Care in the form of higher premiums.
And the HSA has literally transformed the relationship we have with our kids' pediatrician. We are in at least once a month for one thing or another, and happily find value paying out of pocket for much of it in ways that most never do when paying a $15 OV copay. Because routine physicals are covered fully, we haven’t missed one yet.
I have 38 of 50 employees who have selected the $2,850/$5,600 plan over the $300/$600 deductible plan in the same boat as me. Collectively, these employees have more than $80,000 in their HSAs amassed in the last two-plus years. (None opted for the plan the first year, although many kicked themselves after looking at their 2006 spending) that otherwise would have gone directly to United Health Care. These employees are not simply the healthy ones. Most have kids, some are single professionals, others require treatments that cause them to hit the $5,600 deductible in February. Not one person has dropped the HSA once they got on the plan, and all have saved money. I wrote to the Providence Business News about the early success of this option.
Inflation of the healthcare spending in our group has stayed flat to moderate (0% to 3%) according to our account manager, although HIPAA prevents United from seeing actual spending data, as our group is relatively small. And because there is no coshare for the HSA-eligible plan, all employees who want insurance can have it.
So, for at least 50 people, I have an insurance option that:
- Trims the inflation rate of health care spending,
- Provides universal coverage to all who want it
- Provides a better experience when accessing the healthcare system (i.e., better quality)
- Encourages greater access to primary care and preventative behavior.
That sounds like the Holy Grail of healthcare reform to me. But to our Senator and most on the left, such an approach would leave too many Americans without a dependence on the government.
The only thing missing is breaking the linkage that requires my employees to buy this plan through me. The tax incentive individuals receive when buying insurance through their employers deters all from going out on the market to select their own plans. Increase the HSA contribution limit to $15,000, and you erode that linkage.
Once that link is severed, the states will need to free up the insurance market to sell to individuals. In Rhode Island, this is the most heavily regulated of all segments. ObamaCare, as defined by HR 3200, would eliminate this private segment altogether. I guess they do not trust people to select their own health plans, thinking it is bad enough when their employers do it. The left is confident that it can design a better choice for you and then force you to make it. Hayek actually has a term for this.
Mine is not the only company to experience the above. Whole Foods accomplished identical results and detailed it recently in the Wall Street Journal. The response from the left: boycott the heretic offering proven solutions that differ from their agenda.
When the response to opposing views is that aggressive, you have to wonder: Is this really about reform?
August 30, 2009
A Public Option, Despite It All
Sometimes a conclusion seems actively to grapple with the reasoning that precedes it. Such is the case with Michael Fine's Friday op-ed in the Providence Journal. Having complained of the rampant malpractice suits that current law allows, having lamented the "3 zillion government oversight agencies, having observed that "money distorts the public process of reform," and having acknowledged the power of lobbying public officials, Dr. Fine still concludes:
A few years ago, many doctors who thought they were self-employed realized they were working for health-insurance companies. If we are not careful, before long we'll all be working for health-insurance companies, and the U.S., as a nation, will be in a worsening economic mess.That's why we need the "public plan." It ain't perfect, but it provides a way to control the power of the health-insurance companies and the other health-care profiteers while we provide health insurance for all Americans. We'd really be better off if we just focused on what works, and built a health-care system for these United States, but as Winston Churchill so wisely observed, the U.S. usually gets the right answer, after it has tried all the other ones.
Why doctors would rather work for the government than for insurance companies, Fine doesn't explain. Neither does he grapple with the necessity of defining "what works" with reference to the corollary "for whom." But he does, through it all, highlight the common purposes that exist between those who desire government-centered reform and those who prefer government-averse reform. Far from empowering insurance companies, the conservative prescription is to ease the opportunity for others to compete and to transition health insurance back toward true insurance, rather than the whole health management programs that the term currently describes.
Our nation does need doctors to be self-employed business owners, offering personal care to clients whom they can rightfully call theirs. That requires a shortening of the distance that patients' dollars must travel, and changing the path from employer-insurer-biller-doctor to employer-tax collector-bureaucracy-doctor moves in the wrong direction.
August 28, 2009
A Little Further Thought on German Medical Innovation
Among the greatest benefits of blogging is the speed with which one often receives reminders against lazy thinking, and there was certainly a taint of laziness to one of the shorthand quips that I made while simultaneously liveblogging and videotaping the second Whitehouse & Reed healthcare community dinner:
A 75-year-old from German is testifying that his wife's small business has been having trouble keeping up with payments for employees health insurance. Germany, by contrast, is a nirvana of free healthcare. Not sure when the last time Germany led the world in healthcare innovation.
The allusion that I'd intended to express was to my periodic observation that the U.S. system for X (healthcare, military security, etc.) is often a prerequisite for related European systems that leftists turn around and use as a cudgel against the States. My first error was to state the thought in a negative fashion rather than a positive one, to wit: "But the U.S. system is the foundation for national and global innovation." Unfortunately, my first error was facilitated by my second, which was to stop shy (amidst my multitasking) of articulating the particular item I had in mind — a table of the "10 Most Important Recent Medical Innovations," on which I remembered Germany's absence.
The aforementioned reminder came with the following comment from Russ, after I'd provided a link to the table that I'd had in mind:
Interesting stuff, but hardly convincing unless you don't dig into the history:
- CT scans were the result of US and British research... check
- MRIs were discovered by Felix Bloch (and an American who shared the Nobel Prize for Physics), a Jew who fled the Nazis to the US from... you guessed it, Germany!
- balloon angioplasty is a terrible example for this debate (the first angioplasty was performed by German physician Werner Forssmann), later to win the Nobel Prize (along with 2 Americans) for his contributions to medicine.
- Statins were discovered and initially researched in Japan and then picked up in the 1970s by Merck. Yep, the US subsidiary of the German firm.
- Mammography? Also discovered by a German, Albert Salomon, the first to use x-rays to study breast cancer and later expanded by research by German scientists, including W. Vogel, who described how x-rays could detect the difference between cancerous and noncancerous tissues.Some proof!
My concession that the idea deserved more considered phrasing than I gave it does not dilute the fact that Russ has moved the bar considerably. My statement wasn't that Germany has never accomplished anything of value in the medical field, but that it isn't the world leader, and Russ's list doesn't contradict that proposition. If we separate CTs and MRIs, as he does, the list to which I referred has 11 items, of which he addresses five. Of those, he treats it as dispositive to find any German association with a given technology, even including corporate ownership of an American organization working from Japanese beginnings.
Again, I don't believe minimizing the achievements of German nationals to be critical to the point that I'd intended to make, but I do find it curious how many of Russ's examples progressed outside of their country. His reference to Bloch raises the methodology to the point of absurdity: A quick look at the link that Russ, himself, provides confirms that Bloch was Swiss and only happened to be in Germany when Hitler came to power. By the time of the achievement on the top 10 list, he had been in the United States for years and was a naturalized citizen.
Think about that, though: Russ wants to credit German society with the medical achievements of a Swiss scientists whom the Nazis chased out of Europe. I derive no small motivation for carefulness from the realization that my intellectual elisions are apt to drive those who would prove me wrong to such lengths.
The Oregon Trail, in Healthcare
There are warnings related to healthcare to observe in the experience of our neighbor to the north, but we should also turn our eyes westward:
You may have seen the headlines last summer, when Barbara Wagner, a 64-year-old Oregon great-grandmother with advanced lung cancer, got an unsigned letter saying that the Oregon Health Plan (OHP) would not pay for a $4,000-a-month chemotherapy drug, but would pay the $50 cost of physician-assisted suicide.That's because in 1989 Oregon decided to make a comprehensive list of all treatments and diagnoses and rank them by importance to society in preventing disease and doing the most good. ...
... When it first took effect in 1994, Oregon had about 18 percent uninsured. That number dropped to 10 percent but then climbed back up to 17 percent as budget woes in 2004 caused the Oregon legislature to cut back on services and close new enrollment. The latest cuts are in vision care and dental care.
Government-managed healthcare "reform" will not cure the ills that are driving up costs, so it will increasingly have to (1) raise more money via taxes and fees, or (2) decline to pay for procedures. A government body deliberating in the service of number 2 is about the coldest, most dehumanizing methods imaginable.
By contrast, if the critical principle behind reform is freedom, then society can work out the intricacies, leveraging its multiple spheres (e.g., culture, church, and, yes, state). Americans will also have the benefit of whatever additional money they were not taxed for healthcare upfront (whether directly or by pass-alongs from those people and organizations that do shoulder the burden).
Whitehouse and Reed Community Dinner, Take 2
Complete video of Wednesday's community dinner with Senators Sheldon Whitehouse and Jack Reed is available in the extended entry.
On a behind-the-scenes note, the tripod and new software have definitely helped. In fact, they helped so much that I was able to liveblog the meeting while filming it, which explains why it periodically takes a moment for the camera to adjust for movement of the speakers.
Continue reading "Whitehouse and Reed Community Dinner, Take 2"August 27, 2009
Reed's Unimpressive Spinnage
As I catch up with my Projo reading, an article describing a Web chat with Senator Reed reinforces my impression that he's spectacularly unimpressive. I see no intellectual interest in the man, only talking-point recitation:
When readers mentioned two proposals that Republicans tend to embrace, Reed pointed out what he views as their limitations. When a reader expressed support for tort reform to cut down on the practice of "defensive medicine" to avoid costly malpractice lawsuits, Reed replied, "Tort reform is not a primary or sole solution to the problem of accelerating health-care costs."Health savings accounts — another proposal dear to conservatives — are not effective for people who have lost their jobs, Reed wrote. "In addition, with the demands facing many families today, including saving for college, there is a pressure to set aside funds for health care rather than other needs," he added.
The tort reform retort merely shuffles the deck in an attempt to make the savings disappear under the assertion that they wouldn't solve the problem all on their own. The health savings account answer is simply shallow. First, with substantial resources saved in such an account, a temporarily unemployed American could more easily afford COBRA or other individual healthcare option. Second, the Democrats insist that people will continue to invest in their own healthcare, so they're already setting aside those funds for that purpose.
This is a man who claims to be able to invent a better healthcare system?
Senators Reed and Whitehouse in Johnston, Before the Main Event
At a short press conference prior to last night's community dinner in Johnston, I asked Senators Sheldon Whitehouse and Jack Reed if there was any support amongst Democrats in Congress for making the changes to the Federal tax-code that would help undo the biases against individual purchasers currently present in the health insurance market. The audio of their response is available at the link below...
A few of the other interesting items from the questions-and-answer session were…
- In response to a question about whether the Senators expected the tone of the evening be more respectful than the tone of last Thursday's community dinner, due to the passing of Senator Edward Kennedy earlier in the day, Senator Whitehouse volunteered that...
"I thought we had quite a respectful crowd, the last time…"
Look, I know that Senator Whitehouse will never be the most popular Rhode Islander on a conservative blog, but he deserves credit here, for encouraging his constituents of all ideological stripes who have come out and engaged the democratic process. Yes, that is part of the job of an elected representative, but Senator Whitehouse, as well as Senator Reed, have embraced this aspect of their jobs in response to recent events a lot more wholeheartedly than some other members of Congress -- and especially those in the leadership -- have done. - Senator Whitehouse gave an update on whether the "reconciliation" process might be used to allow a healthcare bill to bypass a Senate filibuster and pass with just 51 votes (or 50 plus the Vice-President's?), explaining that reconciliation could be applied only to a limited portion of the content of the healthcare program that is being proposed, and he believes that...
"…the best avenue is to continue to fight towards 60 votes."
- Senator Reed answered a question about whether he would support a bill without a "public option"...
"We're both going to work hard to make sure there is a pubic option…"
[WRNI radio's Flo Jonic] "That's not an answer…"
Senators Reed and Whitehouse in Johnston, Before the Main Event
At a short press conference prior to last night's community dinner in Johnston, I asked Senators Sheldon Whitehouse and Jack Reed if there was any support amongst Democrats in Congress for making the changes to the Federal tax-code that would help undo the biases against individual purchasers currently present in the health insurance market. The audio of their response is available at the link below...
A few of the other interesting items from the questions-and-answer session were…
- In response to a question about whether the Senators expected the tone of the evening be more respectful than the tone of last Thursday's community dinner, due to the passing of Senator Edward Kennedy earlier in the day, Senator Whitehouse volunteered that...
"I thought we had quite a respectful crowd, the last time…"
Look, I know that Senator Whitehouse will never be the most popular Rhode Islander on a conservative blog, but he deserves credit here, for encouraging his constituents of all ideological stripes who have come out and engaged the democratic process. Yes, that is part of the job of an elected representative, but Senator Whitehouse, as well as Senator Reed, have embraced this aspect of their jobs in response to recent events a lot more wholeheartedly than some other members of Congress -- and especially those in the leadership -- have done. - Senator Whitehouse gave an update on whether the "reconciliation" process might be used to allow a healthcare bill to bypass a Senate filibuster and pass with just 51 votes (or 50 plus the Vice-President's?), explaining that reconciliation could be applied only to a limited portion of the content of the healthcare program that is being proposed, and he believes that...
"…the best avenue is to continue to fight towards 60 votes."
- Senator Reed answered a question about whether he would support a bill without a "public option"...
"We're both going to work hard to make sure there is a pubic option…"
[WRNI radio's Flo Jonic] "That's not an answer…"
The Comedy Duo of Whitehouse and Reed
When Monique brought up our liveblogging from the healthcare community dinner hosted by Senators Whitehouse and Reed, on the Matt Allen Show, the conversation drifted toward the oddity of the Senators tackling this issue, locally as a team. Matt's thesis is that Reed doesn't care about the issue, while Whitehouse has all the background, yet he still knows that he'll take a political hit by not appearing to care. Frankly, having watched both events, now, I have to say that I think he's going to take a political hit based on the stark contrast in facility between him and his junior senator. Stream by clicking here, or download it.
August 26, 2009
Dinner in Johnston
Rhode Island roads are designed for people who already know where they're going. That's why I barely made it to Johnston in time to set up for the community dinner hosted b y Senators Reed and Whitehouse. And what do I find when I arrive:

Andrew sneaking up on Pat Crowley! We're a violent mob we right wingers. (No YouTubable video came out of that incident, unfortunately.)
6:03 p.m.
Whitehouse is listing ways to reduce costs in healthcare, most of which are unacceptable (e.g., throw people off the roles). His vague response is that we have to "reform the delivery system in ways that save money." No real solutions.
Jack Reed just repeated the lie that folks who like their insurance can keep it. He didn't add the necessary qualification that it would only last five years.
6:07 p.m.
A 75-year-old from German is testifying that his wife's small business has been having trouble keeping up with payments for employees health insurance. Germany, by contrast, is a nirvana of free healthcare. Not sure when the last time Germany led the world in healthcare innovation.
6:10 p.m.
Whitehouse is trying to explain that foreign companies have an advantage in exports because they don't have to incorporate healthcare for employees into their costs. Of course, the taxes must be worked into the price.
6:15 p.m.
Reed used a popular comeback when an older attendee spoke against the Democrats reform: "Well, what insurance do you have." When the answer is Medicare, he makes a face that says, "Well..."
6:22 p.m.
It's certainly the most quiet crowd tonight. Plenty of shushers when opposition voices make such suggestions as economics lessons in the Senate.
6:25 p.m.
An elderly man, who testified that he's happy with American care, brought up tort reform. Reed is downplaying the importance of that issue, and he looked to the table of planted Brown University medical students .
6:31 p.m.
A 14 -year-old asked whether a national healthcare would be Constitutional, and both Senators said "probably" and brought up a number of state-level public systems (e.g., colleges) as examples of its plausibility. Uh-huh.
6:35 p.m.
Will Grapentine just asked why, if America has the best of hospitals, medicine, etc., as he says Reed suggests, then why change it? He also suggested steps toward privatization.
Whitehouse is also bragging about America's medical facilities. "My concern is that we take all of that talent and excellence, and then we grind it through a system..." that kills people and leaves people out.
6:45 p.m.
Asked about free market competition, Reed said that they're trying to build a better system. Makes me wonder why, if they're such geniuses, in federal government, they went into "public service" instead of applying that insight throughout the economy as private actors.
6:52 p.m.
More repeats of favorite stories, such as Sheldon's example of hospitals not wanting to invest in efficiency equipment because it costs them billable minutes.
I've yet to hear anybody ask or explain why the feds aren't looking at specific problems, first, and then expanding to rewrite the entire system, if necessary.
6:58 p.m.
Whitehouse once again stated that the problems with Medicare originate in the fact that it hasn't been funded, as if some other entity than the government making those decisions.
7:11 p.m.
Whitehouse asserted that Obama has already cut taxes for the middle class, so we can trust him not to break the pledge only to tax rich people.
7:13 p.m.
Whitehouse expressed that the reform is intended to make the system, better, more efficient, and even more super duper. When asked how Congress will pay for it, he brought up digital medical records. First of all, can't that be done on its own? Second of all, is that really the big plan for saving money to pay for a public option et al.
7:20 p.m.
A young woman just noted that businessmen are not accountable to her, but these two senators are. Ah, youth.
A social worker just synopsized the liberal point of view by putting his entire perspective in terms feeling good about helping neighbors, equating a refusal to back a government system naked cruelty of soul.
7:26 p.m.
I have to say that I'm suspicious of the folks who come to these things in white jackets and stethoscopes around their necks are suspicious when they declare themselves doctors. Maybe it's just too much television as a youth, with the whole "I'm not a doctor but I play one on TV" thing.
One such doctor just said that a public option must be big enough to negotiate. That seems to conflict with earlier efforts to diminish the significance of a public option.
Overselling the Public Option, Continued
On WPRO radio's (630 AM) John DePetro show this morning, Senators Jack Reed and Senator Sheldon Whitehouse advanced their position that "the public option" portion of healthcare reform, i.e. a government owned and operated insurance company, would be simply one additional insurance company added to the market, on equal footing with the already existing players.
However, in their answers to a Tim White question on Sunday's WPRI-TV's (CBS 12) Newsmakers program on whether the public option is essential to the Democratic plans for healthcare reform, both Senators seemed to suggest that a public option was not just another choice, but an entity that could achieve goals that private insurers couldn't…
Senator Jack Reed: What we'd like to do is have [the public option] there in place to provide the kind of integrated care, the kind of we hope sophisticated care that raises quality and lowers costsAren't there are obvious problems with simultaneously claiming that the public option will be just like the other insurers, yet will also have impacts beyond those of "regular" insurance companies, having significant effects on the practice of medicine?Senator Sheldon Whitehouse: I think that the success of healthcare reform over time, particularly in terms of improving the quality of care, driving down costs, getting rid of some of the unnecessary waste and conflict and duplication in the healthcare system will be driven by these different public options in 50 different states, finding ways to improve the way that they deliver care…
The idea of the public option being a new source of medical innovation doesn't make immediate sense -- and you don't have to assume noble motives on the part of private insurers to see this. If the public option is truly just another insurance company, except for being owned and operated by the government, then the assumption that it will open the doors to cost-lowering quality-improving innovation is based on the idea that it will do things that private insurers could do, but won't. Er, because private insurers have no interest in lowering costs? If there are ways for private insurers to significantly lower medical costs in the existing employment-based system, why wouldn't private insurers already be doing them (if only to increase their profits, by not passing all or any of the savings along to their customers)?
The contradiction illustrates how much of the argument for "a public option", right now, seems to be based more than anything else on the idea that the problems in American healthcare can be solved by an insurance company that tells doctors and nurses how to be better doctors and nurses -- as long as the insurance company is run by the right people, of course. If the public is to believe that that desire for "a public option" is not driven by unrealistic expectations that government involvement can fix anything, and that it is not a stalking horse for much more intrusive government involvement into medical decision making, advocates for a "public option" need to start resolving their contradictory claims about its structure and the presumed impact it will have on healthcare practice beyond just the dynamics of the insurance market.
August 25, 2009
They've Heard Us
An understandably frustrated Karin commented to a recent post:
Does it really matter who yells and screams. They have no intention of changing the way they vote. The yelling is out of pure frustration that we have zero control over these guys.
One needn't read Sunday's Providence Journal article about our delegation's backing off the public option to comfort Karin that the voices of opposition are making a difference. Of course, it helps to read such things:
For that reason, Langevin suggested that it was a blessing in disguise that both houses of Congress failed to meet Mr. Obama's early-August deadline for passing a bill."I'm glad we had this break to slow this down a little bit," Langevin said, adding that the prospect of historic changes in health care has provoked his constituents to a rare outpouring of deep and personal feelings. Langevin said a powerful theme of the public response has been, "We have to do this the right way. Don't rush it."
Yes, the community dinner hosted by Senator Whitehouse and Senator Reed was a bit more subdued than Langevin's town hall the night before, and we'll see how things go for Whitehouse and Reed in Johnston, tomorrow night But our elected political insiders and their staffs can see the wind shifting away from the hard left.
That's no excuse, of course, for turning down the volume, if only to discredit such statements as this:
"If you like your doctor, you can keep your doctor. If you like your health-care plan, you can keep your health-care plan."But Langevin quickly acknowledged that it may not be possible to keep such a sweeping promise. "There is no guarantee" against at least some disruptions of health insurance coverage, he said.
For example, Langevin said, "It's true that some employers could opt for a penalty" rather than let their workers keep their current health plans.
"Certainly there are always unaccounted for, unpredictable and unintended consequences," in an enterprise as vast and complex as Mr. Obama's planned health-care overhaul, Langevin said.
Similarly, Reed was unwilling to repeat Mr. Obama's promise to the satisfied customer that "you can keep your health plan."
"That is our goal and that is our purpose," Reed said. "We will try our best."
I'm not referring to the persistent statement about keeping one's healthcare, which is a lie wherever it isn't followed by the phrase, "for up to five years." Rather, I mean to indicate the suggestion that consequences described by opponents of the plan are "unpredictable and unintended." The fact is that hundreds of Rhode Islanders — thousands of Americans across the country — have been showing up at their representatives' events explicitly to make such predictions, to the degree that not seeking to avoid the consequences would be strongly suggestive of intention.
Running into the Arms of Government
The reader really must sympathize with Froma Harrop's frustration and ire, and I'm truly sorry for the loss of her husband. The conclusions to which she comes, from that point of view, are, however, plain wishful thinking based on an idealization of an alternative straw to grasp:
An economic note: In 2006, William "Dollar Bill" McGuire, CEO of parent-company UnitedHealth Group, walked off with a $1.1 billion golden parachute (on top of the $500 million he had already raked in) — though he had to return some of it in an options-backdating scandal.What we wouldn't have done to have traded Dollar Bill's minions for a government bureaucrat. The bureaucrat would have given a simple "yes" or "no" based on official guidelines. He or she would have had no personal stake in denying you care.
Government office workers are not mere binary switches in a machine of rigid operation. Observe, even, the ordeal of some Tiverton students who wished to attend an out-of-district public school. Officials within the system led the families to believe that they were all set until, with less than a month to go before the resumption of classes, five strangers with no qualifications beyond the ability to garner a few thousand townie votes decided that the district could not risk setting a precedent.
Rather than simply imagining the purity of a government system, we would be better served to focus on the question of how McGuire was able to siphon billions from his company without putting it at a fatal competitive disadvantage. Until some employment changes enabled me to switch, a month or so ago, I also had UnitedHealth insurance, and were that still the case, I would have no realistic means of reacting, as a consumer, to Harrop's dramatic warning about the company's method of "service."
The problem that we face is that government mandates and regulations have created a mirror image, in the private sector, of a government program. With or without a public option, increased regulation means fewer entities able to clear the bar and enter or remain in the market, which means fewer providers seeking to exploit each other's excesses and affronts.
Harrop laments that her family had to leverage political influence to get the care that her husband required; the value of such political connections can only go up to the extent that the government involves itself in healthcare.
UPDATED: Langevin Town Hall Video
UPDATE: The video below is now complete; I've also managed to take some of the echo out of the audio, so it might be a little easier to understand what people are saying.
Given that Andrew and I attended a separate press session before Congressman Jim Langevin's town hall meeting in Warwick, tonight, and that the event itself went well over the scheduled hour, there's a lot of video to process. It doesn't help that YouTube won't accept videos longer than 10 minutes.
My plan is to upload all the raw footage — and some of it proves definitively that I need practice with my new blogging tool — in one swoop and then to go back and upload segments that merit a closer look for one reason or another. The raw footage phase will take place within this post.
Stay tuned.
ADDENDUM:
Congressman Jim Langevin 08/19/09 Town Hall, Warwick, RI, Preliminary Press Q&A (1):
Congressman Jim Langevin 08/19/09 Town Hall, Warwick, RI, Preliminary Press Q&A (2)
Additional videos in the extended entry.
August 24, 2009
Following-Up the Newsmakers Follow-Up on Illegal Immigrants and Healthcare Reform
Senators Jack Reed and Sheldon Whitehouse appeared on this week's Newsmakers program on WPRI-TV (CBS 12), offering substantive answers to some very good questions on healthcare reform asked by panelists Tim White, Arlene Violet and Ian Donnis. On at least one issue, however, the issue of how illegal immigrants are being addressed in the proposals currently being considered by Congress, viewers were left with a bit of ambiguity about the Senators' positions.
Tim White asked a question (originally posed by a viewer) on this subject and did his best to get a direct answer from Senator Whitehouse…
Tim White: Albert sent this via Facebook. He writes: "What are the unintended consequences of this reform. For example, I hear politicians state that nowhere in the reform does coverage include undocumented aliens but, conveniently, they don't state that nowhere (sic) are they are excluded either." This is, Senator Whitehouse, one of those hot-button issues. You got a lot of these questions last night. How about it, language to exclude illegal aliens…In his answer, Senator Whitehouse is referring to a Senate proposal different from the House bill (HR3200) which has generated much of the current discussion of the details of Congress' plans for health reform; for its part, HR3200 does not extend new coverage or subsidies to illegal immigrants.Senator Sheldon Whitehouse: I think it's clear enough to my satisfaction that this bill does not provide coverage for illegal aliens. A number of our colleagues in the Senate consider this to be a make-or-break issue, and they seem comfortable with it. I think we can safely say that this is not a bill that will provide Federal support for healthcare for illegal aliens.
TW: But would you support any specific language that excludes them?
SW: I have a bill that we've supported already, and it excludes them to my satisfaction. I'm comfortable that we're in the right place on that.
But even if the Senate proposal copies exactly the approach of HR3200, the issue is still not a settled one. Writing in the Hill earlier this month, Congressman Lamar Smith expressed concern about HR3200's failure to define the kinds of eligibility verification procedures used in conjunction with other Federal entitlement programs -- and about active resistance from House Democrats towards adding those requirements…
The legislation contains no verification mechanism to ensure that illegal immigrants do not apply for benefits. Republicans offered an amendment to close this loophole — it would have required verification using the existing methods that are already in place to verify eligibility for other federal benefits programs. But, when they were asked to put the language of the bill where their words were, in a party-line vote, House Democrats rejected the amendment to require verification and close this loophole.At an August 19 panel sponsored by the Center for Immigration Studies, carried on C-SPAN, Robert Rector of the Heritage Foundation went into a bit more detail…
If we were to look at the current healthcare reform legislation, this takes an unprecedented step in opening up the US welfare system to illegal immigrants. Under the current law, really forever, we have had a system of identity checks that largely prevents adult illegal immigrants from getting on to these means-tested welfare programs. You have to be able to substantiate that you're in the country legally and you have to be able to substantiate, if you're a legal immigrant, that you've been here over the time-limits for eligibility.As health reform legislation moves forward, the relevant question concerning this issue is likely to be whether the eligibility verification requirements for new healthcare entitlements are at as least as stringent as the requirements on other means-tested Federal programs, and if not, why there is a difference.The healthcare reform legislation turns that on its back and tramples it into the dust. It basically says we will not verify, we will not check….If you are going to do that with respect to healthcare, why would you not also establish the same precedent with respect to food stamps, to public housing, to the earned-income tax-credit and so forth, and I believe that that is indeed the direction that the Congress wants to go to, to allow all welfare benefits to be fully available to all illegal immigrants.
Take a Step Back to See the Socialization
Since she began targeting a national audience, losing the local flavor, reading Froma Harrop has become a chore that I'm less and less inclined to undertake, but she does still have a knack for highlighting the errors in the thoughts that she's repeating, as is the case here:
Reforming health care should be both a liberal and conservative mission. Securing medical coverage for all Americans is the liberal part. The conservative part is containing the explosive rise in health-care spending, which fuels government deficits and hurts American business in the global marketplace.
The problem is that the monstrosity currently being billed as "health care reform" isn't liberal merely in its motivation, but in the first premises of its strategy: regulate and socialize. Actually, let me stipulate that these are in fact the same premise, as Michael Cannon explained one National Review ago:
Although Romneycare included no insurance program explicitly run by the government, it gave Beacon Hill politicians so much power over the health care of Massachusetts residents that it might as well have. The individual and employer mandates, operating entirely within the private sector, imposed what amount to new tax burdens, gave government the power to regulate all aspects of health insurance and medical practice, and subjected residents' access to medical care to political calculation. Moreover, the fruits of Romneycare have been exactly what you'd expect from a government program. Before reform, Massachusetts's health-care sector was rigid and expensive, with some of the longest waiting times in the nation. Since reform, it has grown even more rigid and expensive — though the politicians have managed to hide more than half of its $2 billion cost. Waits are longer as well, though they hardly merit a mention compared with the more odious forms of rationing involved. ...Like any government health-care program, Romneycare has spurred its share of garden-variety "send a check to Uncle Sam" tax increases. Yet those taxes don't account for even half of Romneycare's costs. Individual and employer mandates are the taxes that politicians prefer when they don't want you to realize they're taxing you. As President Obama's National Economic Council chairman, Larry Summers, wrote in 1989, employer mandates "are like public programs financed by benefit taxes. . . . There is no sense in which benefits become 'free' just because the government mandates that employers offer them to workers." The same is true of an individual mandate: To the extent that government forces people to purchase something they do not value, it is a tax, even if the money never enters the treasury.
Thousands of pages of regulations don't leave much room for competition and choice; indeed, they read much like a specific health insurer's explanation of benefits. Public option or not, this healthcare "reform" is de facto socialization. That is why, despite all the repetition of the half-truth about keeping your coverage if you like it, the bill explicitly ends plans that don't conform to its manifold regulations within five years and forbids any new customers before that time. Otherwise, Americans would flock to the plans that were grandfathered in.
With so many mandates, a healthcare "exchange" will be a bit like a choice between large and extralarge, with most customers making up the difference for those who can only pay for a small.
August 21, 2009
UPDATED: Senators Whitehouse and Reed Meet in West Warwick
UPDATE: The collection of video clips (below) from this event is complete.
Thursday night's community dinner with Senators Jack Reed and Sheldon Whitehouse did indeed have its drama. It also had moments of should-have-been-revelation that we'll be exploring in the days to come.
In the meantime, I'm collecting the raw video in the extended entry section of this post.
Re: Wonks, to the Barricades!
Commenter "Mario" offers some substantive numbers on the number of people without health insurance at any one time in the US...
The CBO helpfully laid out the characteristics of the uninsured population in a paper last December (pg. 38).CBO projects that among the uninsured in 2009, 17 percent will have family income above 300 percent of the poverty level (about $65,000 for a family of four); 18 percent will be eligible for but not enrolled in Medicaid; and 30 percent will be offered, but will decline, coverage from an employer. Some people will be in more than one of those categories at the same time—so overall, about half of the uninsured will meet at least one of those three criteria.A census report (pg. 30) about the 2007 statistics show that 21% of the uninsured were foreign-born non-citizens (doesn't necessarily mean illegal), 20% made over $75k (40% made over $50k, but that doesn't control for family size), and about 17.5% were 18-24 (again, though, some could be all three).I have seen people use 8 million as the "real" number of uninsured, but I can't find anything to back that up. If you were to remove illegal aliens, the people that could buy it if they wanted, the people who could have government coverage if they were to apply, and the people who are only temporarily uninsured (which very much depends on your definition of temporary), my guess is that the number would be somewhere around 25 million.
August 20, 2009
In the Back Door, Again
Thanks to Andrew's emailwork with Sheldon Whitehouse staffers and Tim White's willingness to open the door for a loitering blogger, I've gained entrance to Senators' Whitehouse and Reed's healthcare dinner. I had my PB&J sandwich in the van on the way down, so I've got a moment to chat with you. Congressman Jim Langevin's staffers led us right to the room in which the press Q&A was to be held; tonight, I don't think I attached myself sufficiently tightly to Mr. White in order to make my way into the room where the senators currently are.
There are apparently two rooms, and the senators will only be in one; assuming I'm in the right one, there are some familiar faces from last night, including the Tea Party's Colleen Conley and some of the people who spoke last night. I have seen a number of folks with pro-reform stickers, though.
One thing that struck me in the hall was the general tone of familiarity, and I have to say I was disappointed to see state Senator Leonidas Raptakis body-hug Senator Whitehouse.


5:51 p.m.
I'm seeing a lot of people with "Health Care for America Now!" stickers and name tags, many of them sitting with folks in medical-provider-type uniforms. It would be disappointing to learn that the room in which the senators will be spending the evening is stacked in their favor, with the other one consisting of spillover.



7:45 p.m.
It's wrapping up, now. I'll say this: Although I did get the impression that some of the questions were, well, not unanticipated, there was definitely a healthy representation of the opposition.
Another thing I'll say is that it's edifying to see these guys talk off script. The holes that popped up in the statements and arguments could keep a full-time blogger busy for weeks. Perhaps the healthiest thing that can come out of these town halls — and the point came up that they would not be as big a deal as they are if the administration and Congress hadn't been so blatantly conspiring to push the bill through to law in the dark of a summer night — is to expose the flawed logic of those who lead our nation.
Blogging makes it a different world. Hopefully our politics will catch up before it's too late.
Takeaway #5 from Congressman Langevin's Town Hall: Wonks, to the Barricades!
Two questions of fact regarding healthcare in America, where consensus on all sides does not exist, came up during last night's town hall meeting with Congressman James Langevin…
- What is the count of uninsured people in America, major points of contention being…
- How many of the oft-quoted figure of 47 million unisured includes people who change jobs and don't have insurance for just a few months or even a few weeks during the year, and
- Does the 47-million figure include illegal immigrants?
- Where does the United States rate in quality of care?
- Although it wasn't asked directly, answering this question has to preceded by answering the question of how quality-of-care can be accurately measured.
Blame the Betcha Gal
When the Pawtucket Times' Jim Baron lobbed Congressman Langevin the "death panel" volley ball to smack down during the pre-town hall presser, it occurred to me that if (and I repeat: if) some monstrosity of a socializing healthcare bill becomes law, at least some of the blame with fall to Sarah Palin.
When she initially waded onto the ice with the notion of the government's making healthcare decisions, she was on reasonably solid footing:
The Democrats promise that a government health care system will reduce the cost of health care, but as the economist Thomas Sowell has pointed out, government health care will not reduce the cost; it will simply refuse to pay the cost. And who will suffer the most when they ration care? The sick, the elderly, and the disabled, of course. The America I know and love is not one in which my parents or my baby with Down Syndrome will have to stand in front of Obama's "death panel" so his bureaucrats can decide, based on a subjective judgment of their "level of productivity in society," whether they are worthy of health care. Such a system is downright evil.
This is an argument that can be made as a natural progression from the first principles of the reform, and with evidence from other countries to boot. But when the administration responded, the Palin camp saw the opportunity to declare "got 'im" and jumped on provisions concerning end-of-life decisions. Suddenly, the Democrats could dodge questions on the gravity of government healthcare controls by insisting that a "living will" is not a death panel.
Takeaway #4 from Congressman Langevin's Town Hall: There May Be Some People Thinking that the "Public Option" is Akin to Free Healtcare
At least twice during Congressman James Langevin's town hall meeting last evening, the idea was brought up that a "public option", i.e. a government created and run insurance company, needs to be included in any health reform proposal, as a safety valve for people who lose their jobs (in an employer-based system) and still need coverage.
But does this concept make sense? Unless the "public option" is engaged in seriously predatory pricing, or it is eligible for much bigger subsidies than the private plans on an "exchange" are eligible for, how does a "public option" become any more affordable than a private plan, for someone who has lost their job?
Could it be that some of the support for a "public option" is coming from people who believe it is going to be an entirely-taxpayer funded program?
Takeaway #3 from Congressman Langevin's Town Hall: Of Goals and How to Reach Them
Over the course his town hall meeting last evening, Congressman James Langevin expressed support for healthcare reform goals that would contain costs, expand coverage to the uninsured and prevent monopoly-like behavior from insurance companies. I didn't get any sense from the Congressman's responses that any of these goals were most or least important.
But given that an exact mix of policies that is supposed to brings about cost control (as opposed to providing subsidies to help some people pay their costs) has not yet been made clear, people have a reasonable fear of getting caught up in the government two-step, where the government says first we'll take more control of the healthcare system and then, only after we're in charge, we'll tell you how we're going to cut costs. Whether you like our plans or not.
If the government really knows how to cut costs, why can't they tell us now (in a way that the Congressional Budget Office would believe) -- or even better, why not use their strategies to bring Medicare costs into line?
On the revenue side, Congressman Langevin spoke very decisively in favor of a surtax on upper-income individuals, in order to generate the revenues required by new healthcare programs. But when large revenue is being generated from a narrow base, what is going to happen in the down years? Can we trust government to spend conservatively in the up-years, so there will be something left in the kitty to help bridge the down years -- or would it be more reasonable to expect government to follow its recent pattern and blow through everything it's got in the up-years, forcing big tax increases further down the income spectrum in the down years?
Takeaway #2 from Congressman Langevin's Town Hall: Employment-Based Healthcare May Have More Supporters Than You Think
The most surprising thing I learned over the course of last night's town hall meeting with Congressman James Langevin was of the Congressman's strong commitment to maintaining the employer-based system as the basis of American health insurance. I had thought that most current support for the employer-based system (outside of the insurance industry) sprang from a small-c conservative reluctance to alter what's in place now. Contrary to this idea, Congressman Langevin spoke very actively of wanting to maintain the employer-basis. (He also made it clear that he does not favor a change to a single-payer or a Canadian-style system).
If there was one big-picture healthcare issue I would ask the Congressman to reconsider, the wisdom of maintaining an employment-based system would be it.
Congressman Langevin spoke of ending insurance company "monopolies" over their customers as one of his policy goals. But those monopolies as currently structured are largely artifacts of the employment-based system, where employees are directed to a single insurance company by their employers and told that they can deal with that company, or else get nothing. "Exchanges" are supposed to remedy this take-it-or-leave-it aspect of health insurance, by giving everyone a choice of different companies to deal with, but while the goal here is a laudable one, using "exchanges" to achieve it is a gimmick.
The problem is that the employment-based system did not grow out of an unregulated market; it was created by advantages granted to corporate purchasers of health insurance, by the Federal government, including 1) tax-advantages for corporate insurance purchasers, but not for individuals 2) liability advantages for corporately purchased insurance plans, but not for individually purchased ones and 3) prohibitions against purchasing insurance across state lines, limiting the insurance pools that individuals can choose to join.
Having the government use its tax and regulatory power to strongly tilt the system in favor of employment-based monopolies, and then try to fix the problems it has created by adding new regulations and a new bureaucracy in an attempt to simulate a market is a Rube Goldberg approach to health coverage. The more efficient and more rational solution is to simplify things, by removing the advantages the government has given to corporate health insurance purchasers over individual ones and allowing people purchase their health insurance like they purchase their other kind of insurance.
When regulation has failed miserably, it doesn't automatically mean that the answer is more regulation. It often means that the government has to get out of the way and let people make their own choices
Health and the Town Hall
Monique and Matt hit on various topics related to healthcare and last night's town hall on the Matt Allen Show. Stream by clicking here, or download it.
August 19, 2009
Langevin Town Hall from the Media Perspective
Thanks to Andrew, the two of us were able to sneak through the media entrance to Congressman Jim Langevin's town hall meeting at the Warwick city hall.and to sit in on the private media Q&A. Andrew even got in a question (that wasn't directly answered. Me, I was takinbg video.
The place is packed, probably already at the 300-person capacity, and when I walked up, the line to get in stretched around the building.



Whether It Is or Not, It's What Rationing Will Sound Like
TPublico constructively offers correction of my mention of proposed healthcare-reform changes to wheelchair purchases under the Social Security Act:
That specific section in the Health Reform Bill has nothing to do with rationing, or as the source says '...if you don't specifically need the motorized chair for complex rehabilitation, Obamacare says you can freaking walk or crawl from now on. Or pay for it yourdamnself. ...'Here's the section of the Social Security Act as it is now that the HRB would modify:
(iii) Purchase agreement option for power-driven wheelchairs.—In the case of a power-driven wheelchair, at the time the supplier furnishes the item, the supplier shall offer the individual the option to purchase the item, and payment for such item shall be made on a lump-sum basis if the individual exercises such option.
So if someone needs a motorized chair, they'll still be able to get it... it only modifies a purchase agreement option - an option that is only in there because payment for the rental item (wheelchair) must be made on monthly basis. That source's interpretation is completely false, and way off base.
(I) In general.—Except as provided in clause (iii), payment for the item shall be made on a monthly basis for the rental of the item during the period of medical need (but payments under this clause may not extend over a period of continuous use (as determined by the Secretary) of longer than 13 months).
Following on the Lee Drutman piece to which I linked this morning, I lack the time and motivation to research this minute point across the range from Congressional debates to somebody actually buying a wheelchair, but the "way off base" accusation strikes me as a bit strong. Begin with the fact that, in the actual SSA language, the part about rentals (subsection I) is at a lower level of a different branch than the part about purchase agreements (subsection iii). The end user has three options: rent, rent to own, and straight-out purchase.
Heretofore, the choice to buy the machine outright, rather than rent it, followed the language that TPublico quoted. The Affordable Health Choices Act of 2009 changes that language such that it only mentions "certain complex rehabilitative" power-driven wheelchairs and limits the equipment to "complex rehabilitative power-driven wheelchair recognized by the Secretary as classified within group 3 or higher."
It's entirely possible that this amounts to a mere clarification of a practice already in effect, but it would seem likely that there's a more substantial reason for the change. It could be that this specific measure will cut down on waste, because people have been buying equipment that they really only needed for a few months. Or maybe, in the other direction, dealers want the rental option pushed because, by the time they turn over ownership after thirteen months, they've charged 105% of the purchase price. Or the government may be looking to limit people to a few months of rentals when they really could use the wheelchair in perpetuity. The bottom line is that a payment option that was available for power-driven wheelchairs is now only available for a limited class of power-driven wheelchairs. If that's not rationing, it sure sounds like it. (Keep in mind, of course, that I personally don't think the government should be paying for private medical equipment at all.)
More to the point — inasmuch as I raised this as an example of method, not of implementation — it remains serviceable as a taste of how a massive government-directed bureaucracy will sweep away benefits: with a few words requiring deep expertise in the midst of large, complicated legislation, and with references that snake from the legislation, through another piece of legislation, to a document or judgment from another government office, and then to who knows where, such that we blog disputants can debate at length what the whole thing means. And let's not forget that the current debate is over the House version of the bill. The Senate version will be different, and then the legislation presented for the president's signature could be different again.
The Special Interests Are in the Details
Lee Drutman reminds readers of a point that Milton Friedman made often:
And yet, start reading the actual legislation, and you quickly realize the U.S. health-care system is a dizzying jumble of a thousand and one interconnected pieces, which means a lot of little rules and incentives to get right if any reform is going to work (hence the very long bill). And so, while the public debate carries on in two colors and one dimension, a handful of Washington policy "experts" who actually can grasp the infinite subsections and crevices of health-care law work tirelessly to shape legislative language far from the spotlight.And who are these "experts"? Well, mostly (though not entirely), they are the representatives of doctors, hospitals, insurers and pharmaceutical companies, i.e., the special interests that have both the resources and the stake to actually invest in the expertise one needs to deal in the details. The health-care industry is now reportedly spending more than $1.4 million a day on lobbying.
This is a fundamental problem with treating government as an overarching means of social organization. By the time activists and partisans have riled enough people to get an assertion of government power rolling, entrenched forces and special interests have positioned figure out how to roll it in their favor. One suspects, by the way, that the overlap between those doing the riling and those guiding the roll is significant.
Open Thread: Questions on Healthcare
As we head towards our town hall meetings in the state of Rhode Island where the subject of healthcare reform will be a major issue, here is the big picture question regarding the proposals currently under consideration by Congress: The President and Congressional Democrats are promising that by expanding the Federal role in healthcare regulation (including an individual mandate and various tax penalties on both individuals and companies that don't provide insurance), increasing subsidies and maybe creating a government-run insurance company -- all while simultaneously leaving the Federal tax and regulatory advantages that corporately purchased insurance plans hold over individually purchased insurance plans in place -- they will...
...what exactly?
- Is the answer reduce healthcare costs? If so, could the public be provided with a few examples to use as a model from economic history where Federalizing regulation, providing subsidies, and mandating spending has brought down the cost of something?
- Is the answer expanded coverage? If so, could the public be provided with a few examples (in broad terms) of the kinds of regulations that will needed to achieve this goal, and why a vastly-expanded Federal regulatory structure for healthcare is needed to implement them?
- Would a government-run insurance company be granted the same legal protections that employer-based plans currently enjoy, and not be held legally responsible for the consequences of erroneous decisions to deny treatment? If so, how will this not lead to a competitive pricing advantage over the non-employer based plans sold through a government "exchange" (which presumably would be held responsible for the consequences of their mistakes) and eventually to predatory pricing on the part of the government-run company?
August 18, 2009
It Might Be Better to Face the Swine
Folks might want to consider this before signing up for inoculation:
A warning that the new swine flu jab is linked to a deadly nerve disease has been sent by the Government to senior neurologists in a confidential letter.The letter from the Health Protection Agency, the official body that oversees public health, has been leaked to The Mail on Sunday, leading to demands to know why the information has not been given to the public before the vaccination of millions of people, including children, begins.
It tells the neurologists that they must be alert for an increase in a brain disorder called Guillain-Barre Syndrome (GBS), which could be triggered by the vaccine.
GBS attacks the lining of the nerves, causing paralysis and inability to breathe, and can be fatal.
There's a whole lot of context that one requires from a doctor before issuing a notice of avoidance, but still...
It refers to the use of a similar swine flu vaccine in the United States in 1976 when:
- More people died from the vaccination than from swine flu.
- 500 cases of GBS were detected.
- The vaccine may have increased the risk of contracting GBS by eight times.
- The vaccine was withdrawn after just ten weeks when the link with GBS became clear.
- The US Government was forced to pay out millions of dollars to those affected.
Hard-Luck Cases Make Bad Law, Especially When the President Doesn't Understand Them
The third example used by President Barack Obama in his Sunday New York Times op-ed arguing for more Federal control of healthcare contains serious errors at both the factual and at the conceptual levels (as opposed to his first example, where the error is entirely conceptual)…
OUR nation is now engaged in a great debate about the future of health care in America. And over the past few weeks, much of the media attention has been focused on the loudest voices. What we haven’t heard are the voices of the millions upon millions of Americans who quietly struggle every day with a system that often works better for the health-insurance companies than it does for them.The third example is that of Otto Raddatz of Illinois, who was initially denied a stem-cell treatment by his insurance company (Fortis). However, as Mr. Raddatz’s sister described in Congressional testimony, the decision was eventually reversed…These are people like Lori Hitchcock, whom I met in New Hampshire last week. Lori is currently self-employed and trying to start a business, but because she has hepatitis C, she cannot find an insurance company that will cover her. Another woman testified that an insurance company would not cover illnesses related to her internal organs because of an accident she had when she was 5 years old. A man lost his health coverage in the middle of chemotherapy because the insurance company discovered that he had gallstones, which he hadn’t known about when he applied for his policy. Because his treatment was delayed, he died.
My brother was accused by Fortis Insurance Company of falsely stating his health insurance history, despite the fact that he had no knowledge of ever having any gall stones or aneurysms.Forget the fact that treatment was ultimately approved; the more important question, from a healthcare policy perspective, is why payment for the treatment was denied in the first place -- especially when there is a very good chance that the decision made by the greedy bastards at the insurance company not to pay was strongly influenced by Federal insurance law, which says that insurers are not liable for the consequences of their decisions to deny treatment, in cases where policies are sold through an employer.Luckily, I am an attorney and was able to aggressively become involved in solving this life threatening situation. I contacted the Illinois Attorney General's office and received immediate and daily assistance from Dr. Babs H. Waldman, M. D., the medical Director of their Health Bureau.
During their investigation, they located the doctor who ordered the CT scan. He had no recollection of disclosing the information to my brother or treating him for it.
After two appeals by the Illinois Attorney General's Office, Fortis Insurance Company overturned their original decision to rescind my brother's coverage and he was reinstated without any lapse.
Since we don’t know what was actually going through the minds of the Fortis employees involved in the "routine review" that led to a decision to deny payment, let’s suppose for a moment that the decision really was an honest mistake of some sort. Had the denial gone unchallenged and Mr. Raddatz died as a result, even if the denial was later determined to have been improper, if the insurance policy was provided through his employment, (let’s emphasize this one more time) Federal law (the Employment Retirement Income Security Act of 1974) dictates that the only damages recoverable would have been the costs of the treatments themselves. The Raddatz family would have not been able to recover anything related to the fact that a mistake by an insurance company led to loss of life.
Now, suppose the people of Illinois decide that this situation needs to be fixed, at least in their state. They bribe their legislators (What, you think I’m being unfair to Illinois here? Remember, I am writing this from Rhode Island, where the courts have ruled it legal for legislators to make their decisions based on bribes. I just thought that was the way things worked everywhere. But I digress…) into passing a law that holds Illinois insurance companies liable for costs that follow from their failure to properly honor the agreements they enter into.
If the state of Illinois tried to enforce such a law, the Federal Government would step-in and prevent them from doing so, on the basis that Federal law pre-empts state law when insurance is purchased through an employer and therefore that state liability laws cannot be any more stringent than Federal ones. (Presumably there is some boundary where state laws against fraud take over, if insurance companies collect money for policies that they never intend to pay out on, but the courts have yet to set clear rules defining this boundary at the present time.)
Ultimately, this leads us to an important question yet to be asked about the "public option" that may or may not still be a part of the President's health reform plans. If a so-called “public option”, i.e. an insurance company created and run by the Federal government, is included as part of the reform package, will this company be protected from being held liable for consequences resulting from its decisions to deny treatment, in the same way employer-based plans are protected from liability today? Are the American people ready for a reform that allows the big, new insurer on the block to evade responsibility for the mistakes that it makes?
And before promising that more Federal intervention in healthcare is guaranteed to improve things, shouldn't the President and Congressional Democrats show they are capable of remedying the inequitable treatment of individuals versus corporations that the Federal government has already created?
On Medical Absurdity
Wading through the self-defeating snideness of Ed Fitzpatrick's Sunday column on the healthcare debate (sorry to be harsh, Ed, but it oozes off the page), I wondered whether Fitzpatrick has heard the term "quality-adjusted life year." Here's the definition provided by MedicineNet.com:
A year of life adjusted for its quality or its value. A year in perfect health is considered equal to 1.0 QALY. The value of a year in ill health would be discounted. For example, a year bedridden might have a value equal to 0.5 QALY.
As the Wall Street Journal describes, the measure is particularly popular among bureaucrats in the United Kingdom:
The [National Institute for Health and Clinical Excellence] NICE board even has a mathematical formula [to dictate limits on certain kinds of care to certain classes of patients], based on a "quality adjusted life year." While the guidelines are complex, NICE currently holds that, except in unusual cases, Britain cannot afford to spend more than about $22,000 to extend a life by six months. Why $22,000? It seems to be arbitrary, calculated mainly based on how much the government wants to spend on health care. That figure has remained fairly constant since NICE was established and doesn't adjust for either overall or medical inflation.Proponents argue that such cost-benefit analysis has to figure into health-care decisions, and that any medical system rations care in some way. And it is true that U.S. private insurers also deny reimbursement for some kinds of care. The core issue is whether those decisions are going to be dictated by the brute force of politics (NICE) or by prices (a private insurance system).
The last six months of life are a particularly difficult moral issue because that is when most health-care spending occurs. But who would you rather have making decisions about whether a treatment is worth the price -- the combination of you, your doctor and a private insurer, or a government board that cuts everyone off at $22,000?
Attempting to impose objectivity on these decisions is clinically monstrous. A hugely successful British composer recently decided that a year of decline without his wife was actually worth paying to avoid. But what was the value — to himself and to society — of Stephen Ambrose's final days? Randy Pausch's? Me, far from a 50% detriment to my QALY, I'd see a bedridden year as an opportunity, probably to write a book, especially if I got to get out of bed and go on with my life afterwards.
Fitzpatrick winds up his essay with some powerful testimony from Rhode Island Medical Society President Dr. Diane Siedlecki, but she and he miss a key reality:
"I am the person you tell when you can no longer afford the medication prescribed, so you cut the doses in half or take [them] every other day, hoping at least for partial coverage," Siedlecki said. "I am the person patients call when they wish to be squeezed in for one last visit or for their annual physical exam because they are no longer covered after the end of the month. I am the person called when a patient loses his job and cannot afford to both come in and renew his medications. Or even when she has two jobs and still no has no insurance."
Involving government in healthcare does not alleviate these equations; it does not change the fact that a particular person has a certain amount of resources to contribute to the medical system and requires a certain amount of care. It merely offloads that judgment from the person him or her self. Rather than an individual's deciding whether the benefits of a given pill justify economizing in another area (whether food or the daily lottery ticket), a governing structure — a "death panel," if you will — decides whether one person's medication outweighs another person's cancer treatment or another person's contact lenses.
Whereas a free system allows patients to make their own quality-of-life adjustments, and advocate for themselves among friends, communities, and charities, a system manipulated through government regulation operates on a deceptive and presumptuous objectivity and political power.
The easy self-deception is that those folks calling up Dr. Siedlecki will no longer have to ration their own care, because the government will cover the expense. The other possibility is that they'll find a cold "system" making those decisions for them.
Congressman Langevin's Town Hall Has Changed Venue
Congressman James Langevin has changed the location of his town-hall meeting with constituents this week. It will be held at Warwick City Hall at same time as originally scheduled, 6 to 7 pm on Wednesday, August 19.
August 17, 2009
The Casual Assumption of Correctitude
There are surely practitioners of the stratagem on both political wings, and it's the sort of ploy into which one can slip from time to time, but it seems to me that it is much more characteristic of liberals to weave rhetorical comforters that allow them to slip opinions through as objective fact. This, from Jamison Foser of the liberal Media Matters, is a fine sample. After 75% of a conspicuously benign essay on the need for substantive discussion of the healthcare legislation, this paragraph rolls across the table:
When you see people yelling, "Keep your government hands off my Medicare," that's a clear sign that the public needs some solid facts. How many people do you think know that health-care reform with a strong public option would cost taxpayers less than a plan without such an option? I bet that a distressingly large number of members of Congress don't know that, and that very, very few voters do.
Thus, wrapped in a blanket of mutually agreeable observations about a heated debate, Foser slips through the talking point that really ought to be the object of his argument — because it's a point that actually requires argument. Given the organization for which he writes, promulgating the assertion about costs probably is the objective of the piece, even though it's offered in a tone of "for example."
Ponder, for a moment, the not-so-fine distinction between error and misinformation. On the surface, here, Media Matters is requesting bias; in actuality, the group is endeavoring to insert it.
The Road Not Mentioned
The scoffs that have been so prevalent in response to right-wing talk of "death panels" and such repeat a common liberal tactic of missing the point through deliberate myopia: "Why, this bill merely provides for consultations about end-of-life options, hardly a group of bureaucrats voting to pull the plug. As for rationing, show me one instance in which such a thing will occur." This citation assists in response to both paraphrased points:
Hey, you know those Scooter commercials, where the owner of the company promises that Medicare will pay for 100% of the cost of your motorized wheelchair or they'll eat the difference? In §1141, the phrase "power-driven wheelchair" shall now be replaced in the Social Security Act with "complex rehabilitative power-driven wheelchair." In other words, if you don't specifically need the motorized chair for complex rehabilitation, Obamacare says you can freaking walk or crawl from now on. Or pay for it yourdamnself. On the one hand, the Czar can see how this is a claim to save money—right, GOP? Why do those pesky elderly folks need taxpayers to help them live normal lives? On the other hand, there's something wickedly disingenuous about this. If AARP lived up to its name, this would be the first thing to decry.
That's the sound of rationing in a big government system. A couple of multisyllabic words added in the middle of a legal document so complex that it's barely English and so heavily cross-referenced that it's more like a kidnapper's cut-and-paste ransom note than a coherent narrative. And as Mark Steyn explains, the "death panel" has more of a passive authority:
The problem with government health systems is not that they pull the plug on Grandma. It's that Grandma has a hell of a time getting plugged in in the first place. The only way to "control costs" is to restrict access to treatment, and the easiest people to deny treatment to are the oldsters. Don't worry, it's all very scientific. In Britain, they use a "Quality-Adjusted Life Year" formula to decide that you don't really need that new knee because you're gonna die in a year or two, maybe a decade-and-a-half tops. So it's in the national interest for you to go around hobbling in pain rather than divert "finite resources" away from productive members of society to a useless old geezer like you. And you'd be surprised how quickly geezerdom kicks in: A couple of years back, some Quebec facilities were attributing death from hospital-contracted infection of anyone over 55 to "old age." Well, he had a good innings. He was 57.
The point is that criticism of healthcare reforms takes a longer view, accounting for that which the installed principles make inevitable. Technically, leaving a man floating in the mid-Atlantic on a 2x12 board isn't killing him, but it's likely a death sentence. Although progressives — who admit by their very name that they've got their eye on a broader project — may wish to hold the debate to the immediate effects of specific provisions, a wise electorate should workshop and brainstorm their lasting consequences.
A similar sleight-of-hand is behind the administration's apparent change of tactic in backing away from "public option" talk. In the end, without that fundamental change, the legislation will only exacerbate bureaucracy and complicate a healthcare system already crawling under the weight of regulation. Both political parties will lift up their arms in a declaration of victory, but the necessary reform would merely have been postponed.
There are two paths to the future enabled by the current legislation: a single-payer system that impinges on freedom and ensures the erosion of healthcare around the world, or the gradually corrosive over-medication of a regulatory bonanza. The path that we ought to follow — decreasing regulation and allowing choice to blossom from fertile demand — has scarcely been mentioned.
August 16, 2009
Status of the Public Option
At the time of this posting, the Drudge Report is displaying a big red headline that reads...
RETREAT: TEAM OBAMA DROPS 'PUBLIC OPTION'...which links to an Associated Press story that opens by saying...
President Barack Obama's administration signaled on Sunday it is ready to abandon the idea of giving Americans the option of government-run health insurance as part of his ambitious health care proposal.As Drudge himself would say, developing...
August 14, 2009
Before Voting on a 1,000-Page Bill, Shouldn't We Understand the Problem We're Trying to Fix?
In his defense of a Canadian-style single payer system for health insurance appearing in today's Projo, Dr. Michael M. Rachlis either makes a case that President Barack Obama is badly misguided in his belief that government has to get more heavily involved with medical decision-making as a part of healthcare reform, or else he calls his own basic assumptions into question…
On costs, Canada spends 10 percent of its economy on health care; the U.S. spends 16 percent. The extra 6 percent of GDP amounts to more than $800 billion per year. The spending gap between the two nations is almost entirely because of higher overhead. Canadians don’t need thousands of actuaries to set premiums or thousands of lawyers to deny care. Even the U.S. Medicare program has 80 percent to 90 percent lower administrative costs than private Medicare Advantage policies. And providers and suppliers can’t charge as much when they have to deal with a single payer….If the problem of runaway costs is driven mostly by administration and overhead -- as Dr. Rachlis plainly asserts -- then by what rationale have government-commissioned effectiveness panels that will "bend the cost curve" by determining treatments to be denied (i.e., we've decided we'll pay for the red pill, but not for the blue pill) become so central to the President's discussion of healthcare reform?Because most of the difference in spending is for nonpatient care, Canadians actually get more of most services. We see the doctor more often and take more drugs.…
Whitehouse Responds About Reading
Senator Sheldon Whitehouse's office has sent a response to my inquiry as to the senator's knowledge of the complexities of the healthcare bill:
Thank you for your interest in the important work of reforming our health care system. As a temporary member of the Health, Education, Labor and Pensions Committee over the last several months, I read the Committee's health reform bill closely and participated in the drafting and markup process. Indeed, the Committee's markup of the Affordable Health Choices Act was the longest and most deliberative in the Committee's history. We considered the legislation for 56 hours and 23 separate sessions.During the markup, Chairman Dodd led an open, bipartisan debate in which we
considered about 300 amendments. 161 amendments offered by our Republican
colleagues were accepted and incorporated into the bill.I believe this transparent and thorough process produced excellent legislation,
and I look forward to its consideration by the full Senate.
It appears to have been rash of me to make my initial quip, although I will say that, in this particular case, ignorance of the bill's provisions might have been the charitable assumption when it comes to the legislation's advocates.
August 12, 2009
Challenging Those Fishy Healthcare Claims
So far, the best e-mail sent to the White House tip line on health care discussions has got to be former National Economic Council Director Keith Hennessey's…
I call to your attention several fishy statements about health care reform legislation made by a gentleman named Dr. Douglas Elmendorf. He claims to be Director of the “Congressional Budget Office” and has posted frequently about health care reform on his website, cbo.gov....Elmendorf appears to have several hundred followers in his organization, which has extraordinary influence over many in Congress. I understand that some right-wing Members of Congress support and even vote for his annual funding source.CBO and Elmendorf make extraordinary claims about bills moving through Congress that attempt to implement the President’s plans for health care reform. I bring them to your attention so that you can refute them....
- The House bill would increase the budget deficit by $239 B over the next ten years. This conflicts with the President’s goal of not increasing short-term deficits.
- Ten years from now the House bill would add $65 B to the budget deficit. This conflicts with the President’s insistence that legislation must not increase the deficit in that year.
- The House bill would increase long-term budget deficits by ever-increasing amounts, making our long-term debt problem worse than under current law. This of course conflicts with the President’s statements that “health care reform is entitlement reform,” and that health care reform is essential to addressing America’s long-term budget problems.
- Rather than “bending the cost curve down” as the President has laudably insisted, Dr. Elmendorf said the Senate HELP Committee bill would “raise the cost curve.”
- Under the House bill, in the year 2015 about 8 million uninsured Americans would remain uninsured and pay higher taxes. This would violate the President’s pledge not to raise taxes on anyone earning less than $250,000 per year.
- Under the House bill, about 3 million people who now have employer-sponsored health insurance would lose that coverage because their employer drops it, violating the President’s bold promise that no one will lose the health plan they have now.
- The President’s Medicare Commission proposal would probably save only $2 billion over ten years, and there is a high probability it would save no taxpayer money. In the long run the saving would be “modest.”
Challenging Those Fishy Healthcare Claims
So far, the best e-mail sent to the White House tip line on health care discussions has got to be former National Economic Council Director Keith Hennessey's…
I call to your attention several fishy statements about health care reform legislation made by a gentleman named Dr. Douglas Elmendorf. He claims to be Director of the “Congressional Budget Office” and has posted frequently about health care reform on his website, cbo.gov....Elmendorf appears to have several hundred followers in his organization, which has extraordinary influence over many in Congress. I understand that some right-wing Members of Congress support and even vote for his annual funding source.CBO and Elmendorf make extraordinary claims about bills moving through Congress that attempt to implement the President’s plans for health care reform. I bring them to your attention so that you can refute them....
- The House bill would increase the budget deficit by $239 B over the next ten years. This conflicts with the President’s goal of not increasing short-term deficits.
- Ten years from now the House bill would add $65 B to the budget deficit. This conflicts with the President’s insistence that legislation must not increase the deficit in that year.
- The House bill would increase long-term budget deficits by ever-increasing amounts, making our long-term debt problem worse than under current law. This of course conflicts with the President’s statements that “health care reform is entitlement reform,” and that health care reform is essential to addressing America’s long-term budget problems.
- Rather than “bending the cost curve down” as the President has laudably insisted, Dr. Elmendorf said the Senate HELP Committee bill would “raise the cost curve.”
- Under the House bill, in the year 2015 about 8 million uninsured Americans would remain uninsured and pay higher taxes. This would violate the President’s pledge not to raise taxes on anyone earning less than $250,000 per year.
- Under the House bill, about 3 million people who now have employer-sponsored health insurance would lose that coverage because their employer drops it, violating the President’s bold promise that no one will lose the health plan they have now.
- The President’s Medicare Commission proposal would probably save only $2 billion over ten years, and there is a high probability it would save no taxpayer money. In the long run the saving would be “modest.”
Facing the Healthcare Committee
Sure, it would take a few stolen bases to present the thought in the form of an argument, but watching the Tiverton School Committee stand firm against requests from parents for permission to move their children out-of-district to be better served (they believe) elsewhere, I couldn't help but flash forward to some similar plea within the structure of public health insurance.
"Ma'am, we understand that you feel you've had horrible results with our local doctors and that you think your son would have a better chance of a healthy life if he had access to the children's facility across the state, but if we make this exception for you, the precedent would bankrupt us. According to these statistics, the doctors participating in our program are just as competent under various criteria as the doctors in that facility, so we really can't justify the cost."
To be sure, there's already too much of such decision-making in our system based on insurance companies typically contracted through the workplace, but that's an argument for deregulation, not omniregulation.
August 11, 2009
Unions Sowing Fear in the Streets
As a follow-up on the subject of organized labor stoking civil violence, it turns out that one of the Service Employees International Union (SEIU) members who crossed into physical violence in St. Louis wasn't just a overexcited layman:
Elston K. McCowan is a former organizer - now the Public Service Director of SEIU Local 2000 - and board member of the Walbridge Community Education Center, and is a Baptist minister, has been a community organizer for more than 23 years, and now, he is running for Mayor of the City of St. Louis under the Green Party.
As Clarice Feldman observes, McCowan "is the union"; he's one of the guys who "issues the cards."
Join that with an SEIU memo in Connecticut that explicitly instructs supporters to "drown out" those who oppose the healthcare power grab. The line between "being heard" and "making not heard" is not so subtle. The former is an expression of democratic process. The latter indicates an intention to bully the opposition into simply staying home in the interest of their own safety.
In Michigan, a man who confronted Rep. John Dingell (D., Michigan) about the availability of resources, under Obamacare, for his son's cerebral palsy subsequently received a visit in the middle of the night. Welcome to hope and change.
August 10, 2009
Healthcare Makes for a Dog's Life
The ever-worth-reading Theodore Dalrymple, himself a doctor, compares international — and inter-species — healthcare programs and comes to some insightful conclusions, including this one:
Across the Channel, there is very little that can be said in favor of a health system which is the most ideologically egalitarian in the western world. It supposedly allots health care independently of the ability to pay, and solely on the basis of clinical need; but not only are differences in the health of the rich and poor in Britain among the greatest in the western world, they are as great as they were in 1948, when health care was de facto nationalized precisely to bring about equalization. There are parts of Glasgow that have almost Russian levels of premature male death. Britain’s hospitals have vastly higher rates of methicillin-resistant Staphylococcus aureus (a measurement of the cleanliness of hospitals) than those of any other European country; and survival rates from cancer and cardiovascular disease are the lowest in the western world, and lower even than among the worst-off Americans.Even here, though, there is a slight paradox. About three quarters of people die of cardiovascular diseases and cancer, and therefore seriously inferior rates of survival ought to affect life expectancy overall. And yet Britons do not have a lower life expectancy than all other Europeans; their life expectancy is very slightly higher than that of Americans, and higher than that of Danes, for example, who might be expected to have a very superior health-care system. Certainly, I would much rather be ill in Denmark than in Britain, whatever the life expectancy statistics.
Perhaps this suggests that there is less at stake in the way health-care systems are organized and funded, at least as far as life expectancy is concerned (not an unimportant measure, after all), than is sometimes supposed. Or perhaps it suggests that the relationship of the health-care system to the actual health of people in societies numbering many millions is so complex that it is difficult to identify factors with any degree of certainty.
Mr. Dalrymple also seconds a point that I've made several times: that the United States' current healthcare is disproportionately expensive, compared with the rest of the world, in part because we're carrying some of the load for those other countries, particularly in continuing innovation. The healthcare "reforms" currently in discussion within the federal government will begin the process of retarding technical development.
You Don't Get to Decide About Keeping Your Current Healthcare Coverage, Unless You are One with Your Employer
A number of analysts have begun to note that, under current Democratic healthcare proposals, President Barack Obama's promise that "if you like your health care plan, you’ll be able to keep your health care plan" is not reality-based. Under the Democratic plans, "you" don't get any choice in whether to keep your existing coverage if your employer decides to discontinue coverage under the new rules.
If the President and Congressional Democrats were serious about helping "you" keep the coverage you have now, they would support two basic reforms…
- They would give individuals who purchase health insurance directly from an insurance company the same tax-breaks that are given to corporate-provided health plans. Presently, corporate-purchased health plans qualify for tax-breaks that individually-purchased plans do not; the proposals favored by the President continue this disparity.
- They would end the disparate legal treatment of insurance-company coverage decisions that is an unintended consequence of the Employee Retirement Income Security Act of 1974. ERISA has driven insurers towards offering their products only through employers, because a wide-range protections from lawsuits over improper coverage decisions is granted to employer-based plans, but not to individually-purchased ones. The effect of ERISA is an important underdiscussed factor in creating the unsatisfying health insurance system we have today.
p.s. Does the fact that this post illustrates that the claim made in today's USA Today by Speaker of the House Nancy Pelosi and Majority Leader Steny Hoyer...
[The proposals passed by Committees in the House] will allow every American who likes his or her current plan to keep it.…requires some very heavy qualification mean that I am un-American for posting it?
August 8, 2009
Sit Down, Community, and Be Organized!
If anything, Mark Steyn's latest lays on the wordplay a bit too thick, but apart from his usual humor, this one's worth reading if only to sow the last four sentences of this block quote into the conservative repartee:
"The right-wing extremist Republican base is back!" warns the Democratic National Committee. These right-wing extremists have been given their marching orders by their masters: They've been directed to show up at "thousands of events," told to "organize," "knock on doors" ...No, wait. My mistake. That's the e-mail I got from Mitch Stewart, Director of "Organizing for America" at BarackObama.com. But that's the good kind of "organizing." Obama's a community organizer. We're the community. He organizes us. What part of that don't you get?
August 7, 2009
The First Murmurs of Political Ugliness
John Loughlin, the presumed Republican candidate for Patrick Kennedy's seat in Congress, has issued a press release stating that "the Congressman has a basic obligation to share his in-depth knowledge" about healthcare legislation at three to five town-hall-style meetings. As a matter of an elected representative's responsibility, Loughlin is absolutely correct, but constituents might have cause to worry that the ordeal of such meetings might send Patrick back into preventive rehab. The "debate" is getting ugly.
After a few instances of citizens' displaying their passion about the Democrats' federal powergrab in a porcine "healthcare reform" costume, party figures have been striving to prove that nobody does divisiveness as well as they do:
Democrats and the White House are claiming that the sometimes rowdy protests that have disrupted Democratic lawmakers' meetings and health care events around the country are largely orchestrated from afar by insurers, lobbyists, Republican Party activists and others.
Jonah Goldberg goes into further detail about the Democrats' attacks on American citizens. Peggy Noonan took up the topic for the must-read piece to which Marc linked earlier. Noonan highlights the looks of shock that have been characteristic of the Democrats who've been experiencing Americans' frustration. "They had no idea how people were feeling," she writes, and she ends on a note of concern that their leaders and allies see more need for forehead-to-forehead response than for the much-invoked empathy:
Absent [President Obama calling for a pause in the debate], and let's assume that won't happen, the health-care protesters have to make sure they don’t get too hot, or get out of hand. They haven’t so far, they’ve been burly and full of debate, with plenty of booing. This is democracy’s great barbaric yawp. But every day the meetings seem just a little angrier, and people who are afraid—who have been made afraid, and left to be afraid—can get swept up. As this column is written, there comes word that John Sweeney of the AFL-CIO has announced he’ll be sending in union members to the meetings to counter health care’s critics.
If, like me, you've come across news of a beating that apparent members of the Service Employees International Union (SEIU) delivered to a grassroots activist in Missouri, and watched the video of the aftermath, Noonan's final chord is chilling.
To be sure, meeting constituent unrest with union thuggery is probably not what White House Deputy Chief of Staff Jim Messina meant when he told Senate Democrats, "If you get hit, we will punch back twice as hard," but the imagery is telling. And dangerous. Citizen ire is going to turn into bloodsport politics, in part because ostensible leaders prefer to battle than to listen.
Here Are Yer Angry Mobs!!!
Dana Loesch has some pictures of the "angry mobs" showing up at the Health Care Town Halls (you know, where there is supposed to be an open discussion, yada yada yada). Here's an example:

Scary!
The leftosphere and the liberal commentariat charged that the town hall meetings weren’t authentic, the crowds were ginned up by insurance companies, lobbyists and the Republican National Committee. But you can’t get people to leave their homes and go to a meeting with a congressman (of all people) unless they are engaged to the point of passion. And what tends to agitate people most is the idea of loss—loss of money hard earned, loss of autonomy, loss of the few things that work in a great sweeping away of those that don’t.People are not automatons. They show up only if they care.
What the town-hall meetings represent is a feeling of rebellion, an uprising against change they do not believe in. And the Democratic response has been stunningly crude and aggressive. It has been to attack. Nancy Pelosi, the speaker of the United States House of Representatives, accused the people at the meetings of “carrying swastikas and symbols like that.” (Apparently one protester held a hand-lettered sign with a “no” slash over a swastika.) But they are not Nazis, they’re Americans. Some of them looked like they’d actually spent some time fighting Nazis.
August 6, 2009
Well-Dressed Grass Roots? Just can't be!
Polls continue to indicate President Obama's and the Democrats' health care reform is in serious trouble. And the Dems are worried...and paranoid. They haven't been able to drum up support with their much-touted netroots apparatus and are instead encountering protests against their proposals. But it couldn't be that their grand plan is wrong...instead, the Democrats are claiming this opposition is nothing more than "astroturf." (Kinda like the Tea Parties, I guess). California Senator Barbara Boxer thinks that well-dressed protesters to Obamacare must be put-ups. Local progressives theorize that the media is conspiring ("which side are you on"?) against President Obama. And, as Michael Barone summarizes:
So now we have the spectacle of the White House trying to demonize the health insurers which it was not so long ago romancing and trying to label as “mobs” and “astroturf” voters who show up at town meetings and voice opposition to Democratic health care proposals—this from a president who during his campaign urged his supporters to respond to those opposing him by “get[ting] in their faces.” These seem like desperation tactics to me. Most Americans are pretty happy with their health insurance because, for one reason, they can choose a different plan every year. It's not irrational for them to fear getting shoved into a government plan which, to save money, will ration care.Barone acknowledges that, usually, there is more enthusiasm by those on the outside looking in, but he thinks there's something more going on, too.
One of the less commented on features of our politics in this decade has been the huge expansion of voter turnout, from 105 million in 2000 to 122 million in 2004 and 131 million in 2008. These increases were generated by campaign organizations (including the brilliantly targeted efforts of the Obama campaign) but were also a spontaneous expression of enthusiasm—both for and against George W. Bush in 2004, for Barack Obama and against Bush in 2008.Democrats/Progressives are projecting their organizational model onto the average citizen. Believe it or not, folks can get upset enough all on their own: we all don't require "community activists" to identify our problems for us. When asked the generic question if health care needs to be reformed, the majority of Americans say "yes" (myself included). But this isn't what we have in mind. Instead, keep it simple by focusing on two words: portability and competition. Then work from there.You don’t do an unnatural thing like going to a congressman’s town hall meeting to express opposition to a health care proposal just because you got a robocall from someone from Cigna or Aetna. They don’t dragoon poor people into buses the way Acorn does. You go because you feel really, really strongly about some issue. There are, after all, organizers on both sides. The organizers favoring the Democratic health care plans aren’t able to generate any significant. The organizers opposing the Democratic health care plans are. And, as in the 2008 Obama campaign, a lot of people are turning out of their own spontaneous accord.
Blame the Government for Healthcare Foolishness
The government (abstractly speaking) has somehow wiggled its way into a comfortable position in which, as an entity, it need never take blame. Consider a letter from Ben Jones, in Providence:
When my wife and I moved to Rhode Island, my wife's employer-provided insurance plan increased its pricing to over twice the cost, with fewer benefits, than rates for me as an individual. Unfortunately, I discovered that I could not buy insurance in Rhode Island as a sole proprietor, since I had rejected my spouse's employer's plan. Being forced to choose a group plan that cost us more and delivered less didn’t seem like much of a choice to me.A public health-insurance plan might have offered a true choice, or at least kept the private insurers' rates competitive. In Rhode Island, two insurers cover 95 percent of people with health insurance, limiting our choices further.
Tracing the history of Rhode Island healthcare — of which there is no helpful summary for the immigrant — one observes that the General Assembly created Blue Cross as a non-profit. Apart from that, the state has layered on sufficient mandates and regulations, some microspecific in scope, that we arguably have experience with a "public option."
Take Jones's specific complaint: His lack of eligibility for health insurance as a sole proprietor is a statutory allowance created as part of legislation with the following purpose:
The purpose and intent of this chapter are to enhance the availability of health insurance coverage to small employers regardless of their health status or claims experience, to prevent abusive rating practices, to prevent segmentation of the health insurance market based upon health risk, to spread health insurance risk more broadly, to require disclosure of rating practices to purchasers, to establish rules regarding renewability of coverage, to limit the use of preexisting condition exclusions, to provide for development of "economy", "standard" and "basic" health benefit plans to be offered to all small employers, and to improve the overall fairness and efficiency of the small group health insurance market.
This is what it looks like when a government imposes "options." The only difference under the regime that Jones advocates is that the government would not be forcing distinct (or semi-distinct) entities to operate its preferred plan; it would just regulate and mandate directly as a definition of its offering.
August 4, 2009
Flagging the Fish
Apparently, the White House has set up an email account to gather inconvenient rhetoric about healthcare reform:
There is a lot of disinformation about health insurance reform out there, spanning from control of personal finances to end of life care. These rumors often travel just below the surface via chain emails or through casual conversation. Since we can’t keep track of all of them here at the White House, we’re asking for your help. If you get an email or see something on the web about health insurance reform that seems fishy, send it to flag@whitehouse.gov.
I agree with Tevi Troy that the "flag" idea is inspired and have forwarded Sen. Sheldon Whitehouse's recent op-ed to the email address. I just know that he hasn't read the bill with sufficient attention to justify his professed "confidence" about its effects and his entire op-ed is consequently "fishy."
By Their Rhinestone Ban You May Know Them
Walter Olson, of Overlawyered, highlights Rhode Island as the base of "America’s costume jewelry industry" in his coverage of the Consumer Product Safety Commission's ban on rhinestones and crystals and has collected multiple telling details, including this one:
It doesn’t even matter whether a kid’s health is at more risk (by way of traffic accidents) from being driven to the mall to buy a substitute garment than from going ahead and wearing the rhinestone-bedecked tiara or camisole in question.
The crux of the issue, of course, is this:
To a large extent the Commission's hands were tied by the absolutist, not to say fanatical, prescription of CPSIA itself, which directs that exemptions be turned down if they could lead to "any" — not "infinitesimal", not "too small to worry about" — absorption of lead or public health risk.
Which makes consumer protection legislation a "practice exam" for healthcare overhaul, in Hugh Hewitt's words:
In short, the CPSIA is a perfect example of Congress's inability to write reasonable, coherent legislation free of devastating though unintended side-effects even in a relatively simple area of legislative endeavor.Imagine what havoc it will unleash when Congress turns to the massive and massively complicated area of health care and begins to mandate that all or almost all businesses in America adopt certain policies and make obligatory choices. It has done so in the past with regard to important matters such as retirement savings programs and union elections, and always the roll-out of such undertakings has been difficult and marked by uncertainty and difficult questions of legislative intent. ...
... The refusal of Congress to move to clean up the mess it made with CPSIA also announces what will happen after Congress passes its magic wand over health care and blows up who knows what: nothing. Tough luck. Deal with it. They will all have campaigns to run which won't want to focus on the new laws failures and shortfalls.
August 3, 2009
En Route to a Single-Payer
Just in case there's anybody who still believes that the "public option" is intended as anything other than a catalyst for a fully single-payer system:
Out of Touch Every Which Way
Something's curious about Mark Barabak and Faye Fiore's presentation of the lack of street creds in Congress when it comes to healthcare:
Too much, too fast, too expensive. Those are some of the objections lawmakers have voiced against the healthcare overhaul Democrats are attempting on Capitol Hill.But many Americans think Congress is out of touch. How, they wonder, can lawmakers empathize with the underinsured or those lacking insurance when they receive a benefits package -- heavily subsidized by taxpayers -- that most of us can only envy?
It isn't the editorializing that's striking; at this point, that's expected. What's odd is the one-sided insinuation that comfy legislators can't empathize with a public that lacks a "public option." Put aside the reality that there isn't anything fundamentally more secure about Congress's benefits than those of Americans in the private sector. They can lose their jobs, and sufficient pressure from the public would ultimately succeed in decreasing the benefit.
Most peculiar is the implicit notion that, even as legislators cannot empathize with the healthcare realities of their countrymen, they ought to take upon themselves the responsibility of rewriting those realities.
The End Game of a "Public Option"
Given the political philosophies of some of the strongest supporters of a "public healthcare option," it would be reasonable to suspect that this sort of invasion is a desired outcome, not an unfortunate development, in the quest to engineer a healthcare and well-being system for the people's own good:
The Children's Secretary set out £400million plans to put 20,000 problem families under 24-hour CCTV super-vision in their own homes.They will be monitored to ensure that children attend school, go to bed on time and eat proper meals.
Private security guards will also be sent round to carry out home checks, while parents will be given help to combat drug and alcohol addiction.
Targeting root causes is a productive principle for organizing a social response, but the unavoidable conclusion is that people very often turn out, themselves, to be the root causes of their own problems. Two routes around that reality exist: claim an ever-more-invasive right of public manipulation of their lives to force them to live by an imposed definition of "correctly," or guide them philosophically toward a worldview that tends to contribute to the desired conclusions and behaviors. The latter is a much more extensive project, and typically requires that public coercion not be central to implementation — the exceptions coming only when government inaction is tantamount to favoring the other side and to be indulged only to the most minimal degree possible.
Unfortunately, the latter approach has been systematically targeted and decried as "oppressive" by movements that (surprise, surprise) wind up advocating for the former approach.
(via Mark Steyn in the Corner)
August 2, 2009
Comparative Feelings About Healthcare
Before yesterday's RISC meeting, somebody of my general political philosophy mentioned that she'd just returned from Canada, and her associates in that country were well satisfied with their healthcare. Such testimonies are worth considering, of course, but anybody who feels anything other than utter bewilderment at the Mac v. PC spats, in either direction, should understand their subjective nature. If the techie analogy doesn't work for you, just about any product type will do — cars, game systems, shampoos, comic book publishers, sports franchises, or, directly to the point, nations. We human beings tend toward chauvinism, broadly speaking, on matters large and small.
The United States of America has long been the global superpower. The grand economy. The military giant. The entertainment king. The innovator. Being more a philosophical individualist than a nationalist, I see that mainly in functional terms; our system of society has gotten something important right (amidst all of the many things that our culture has undeniably gotten wrong). But as with other components of identity, folks the world 'round evince a natural affinity for their own countries and a desire to defend them on qualitative grounds.
One gets the impression, reading around, that it's a point of pride for foreign nationals that their governments "are able" to provide universal healthcare, and ours is not. In the presence of an American guest, therefore, it would be natural for them to, well, downplay the bad and emphasize the good. Pervasive horror-story propaganda about non-government healthcare systems likely stoke that subtle nationalism.
From amidst my vast internal archive of high-end cultural memories, an example emerges: During an episode of MTV's Real World, London, which aired in 1994, Sharon became ill and had to be whisked to the hospital, where the doctors were able to remedy her potentially fatal (if usually benign) ailment. Neil, who was pursuing a career as a rock star during his hiatus from Ph.D. studies in experimental psychology, berated his American flatmates (too clueless to have a response) that their friend would absolutely have died had she been uninsured in their home country.
His passionate vitriol was patently odd. In retrospect, though, it was understandable. Sure, his country has long been waning — and in a manner bound up with cultural insecurity and guilt — but at least his countrymen had the good hearts to save each others' lives.
It would be interesting to get a reaction from Neil, or from my acquaintance's Canadian friends, to this list that's been making its way around the right-wing blogosphere:
- Americans have better survival rates than Europeans for common cancers.
- Americans have lower cancer mortality rates than Canadians.
- Americans have better access to treatment for chronic diseases than patients in other developed countries.
- Americans have better access to preventive cancer screening than Canadians.
- Lower income Americans are in better health than comparable Canadians.
- Americans spend less time waiting for care than patients in Canada and the U.K.
- People in countries with more government control of health care are highly dissatisfied and believe reform is needed.
- Americans are more satisfied with the care they receive than Canadians.
- Americans have much better access to important new technologies like medical imaging than patients in Canada or the U.K.
- Americans are responsible for the vast majority of all health care innovations.
Number 10 pops up in various contexts. For example, over the course of decades, other developed nations have been able to spend a lower percentage of their budgets on military forces, because they've fallen under the protective umbrella of the United States. Just so, the (somewhat) free-market system in the U.S. has kept incentives alive for continued medical innovations and technologies. The page from which I took the above list also has a table of ten critical medical innovations, and the prominence of our country is conspicuous.
In that regard, however much they may be inclined to extol the approach of their own nations to the provision of healthcare, our fellows across the border and across the sea should keep their fingers crossed that Americans aren't so persuaded as to emulate them.
July 31, 2009
Abortion Insinuates Itself in a Leftward Government
Barth Bracy, executive director of the Rhode Island Right to Life Committee, makes an interesting observation in the current issue of the Rhode Island Catholic:
In less than six months Obama has appointed dozens of extreme pro-abortion ideologues to key positions in government, nullified the Mexico City Policy, and authorized taxpayer funding for embryo-killing experimentation, for abortion-on-demand in the District of Columbia, and for the United Nations Population Fund, which supports China’s population-control program with its coerced abortions. While speaking of safeguarding conscience rights for health care professionals, his administration is dismantling protections they already enjoy. Meanwhile, authentic common ground proposals, like the Pregnant Women Support Act, languish with no support from his administration. And while it may appear that he has backed off from [Freedom of Choice Act (FOCA)], his campaign pledge to the abortion industry, the reality is that he is stealthily inserting the provisions of FOCA into other bills. Indeed his allies in Congress are even now pushing health care bills that would establish federal funding for abortion on demand, override state abortion laws, and vastly expand access to abortion.
Bracy's commentary comes in the form of a response to George Cardinal Cottier's expressed support for President Obama in relation to his appearance at Notre Dame, so it's context that places the focus on the president. The reality is that devoting federal dollars for the killing of unborn children — American as well as across the globe — is a Democrat project. Regarding abortion slipped into the healthcare bill, here's the latest:
Last night, the House Energy and Commerce Committee narrowly passed the Stupak-Pitts amendment to prevent the bill from mandating that private insurance plans cover abortions, but when Chairman Henry Waxman brought the amendment up for reconsideration, Rep. Bart Gordon of Tennessee flipped his vote to 'no', defeating the Stupak-Pitts amendment 30 to 29. "I misunderstood it the first time," Gordon said of his flip-flop, according to The Hill. Gordon and Zack Space of Ohio were the only Blue Dogs on the committee to vote against the amendment to ban mandates for abortion.Instead of the Stupak-Pitts amendment, the committee passed an amendment that is being billed by some Democrats as a "common ground" measure on abortion. The amendment--sponsored by Lois Capps (D-Calif.), whose National Right to Life Committee vote-scorecard is 0 for 74--would allow the "public option" to provide coverage for elective abortions and would allow federally subsidized private plans to provide abortion coverage as well. How exactly could this be construed as "common ground"? Congress isn't requiring the public option to cover abortion--merely allowing it. And through some nifty bookkeeping, abortions will supposedly be paid for out of private funds rather than tax dollars.
The silver lining may be that Democrats' unwillingness to let go of taxpayer dollars for fetal slaughter could be decisive in killing the final bill. It's a cosmic travesty, though, that the end game could be such a close thing, once again seeming to pit the lives of the youngest human beings against the health of their older brothers, sisters, and parents.
July 30, 2009
A Debacle in Healthcare
The Lenin-era cliché that Capitalists would sell Communists the rope with which to hang them comes to mind, only in this case, it involves voters allowing their representatives to get to the point of not even reading the legislation by which they're taking our freedoms away.
Such was the conversation last night, on the Matt Allen Show, during which I had the pleasure of checking in with Tony Cornetta, who was covering for Matt, who was covering for Dan Yorke. I mentioned, to Tony, a line in Senator Sheldon Whitehouse's recent Projo op-ed, in which he declares that he's "confident that with the landmark bill our committee has passed, we're on the right track." In light of the quip from Representative John Conyers (D-MI) that reading such legislation is temporally impossible (and therefore an unreasonable expectation), I've contacted the senator's office to inquire as to his own accomplishments with respect to the text of the bill. It would be discouraging to learn that his confidence in the legislation is based mainly on faith.
Stream by clicking here, or download it.
July 29, 2009
Kennedy Opening the Door to Subjugation
Writing on RIFuture, last week, Rep. Patrick Kennedy presented a frightening intention with an ease suggestive of an ignorance about its implications:
I am also proud to have successfully worked on an amendment with my colleagues to ensure that screening for mental health and substance-use disorders are covered as a preventive service under this bill. Addiction, just like cancer, diabetes, and heart disease, is a preventable and treatable chronic disease. Utilizing screening as a preventive, pro-active tool of medicine to detect mental illness and drug and alcohol use helps identify at-risk populations so we can intervene early and thereby significantly reduce the incidence of these diseases among Americans. Screening is an effective way to alleviate needless suffering while saving health care dollars.
I called Kennedy's Washington office on Friday to get the specific language of which the Congressman is so proud but have not heard back, and on my last check, amendments to the healthcare bill were not available online. It's still possible, though, to marvel at danger of the general concept. What could it possibly mean to screen for "mental illness" in order to "reduce the incidence" and save "health care dollars"? It sounds to me as if people who might be prone to, say, depression would be screened and then, assuming government control of healthcare and its costs, pressured to take the appropriate medication. At the very least, they would be monitored. Now expand the possible mental illnesses; would people prone to aggression be drugged or watched?
Readers who think the periodic debate over the diagnostic standards of the psychiatric profession are ridiculously politicized already should shake in their manacles over the industry's power should the Democrats' preferred future come to pass.
July 28, 2009
Obesity: One Arm of the Healthcare Clamp on Freedom
The question is who should pay the premium for lifestyles that increase healthcare costs because of obesity?
Obesity's not just dangerous, it's expensive. New research shows medical spending averages $1,400 more a year for an obese person than for someone who's normal weight. Overall obesity-related health spending reaches $147 billion, double what it was nearly a decade ago, says the study published Monday by the journal Health Affairs.
To some extent, the cost is currently spread out across insurance products, although the amount of the patient's contribution varies hugely depending on their coverage. Since the average is pulled up by ailments that tend to increase in prevalence later in life, lifelong obesity is surely a factor in Medicare costs, as well.
As government officials ratchet up the hard sell for their healthcare-based power grab, we should consider that mandates preventing providers and insurance companies from adjusting prices based on preexisting conditions ensure that more of the cost of obesity is borne by other people than the patient and that a government-run system would take the responsibility entirely upon itself. Of course, being the government, it will then translate that responsibility into authority to dictate behavior.
RTI health economist Eric Finkelstein offers a blunt message for lawmakers trying to revamp the health care system: "Unless you address obesity, you're never going to address rising health care costs." ...It's not an individual problem but a societal problem — as the nation's health bill illustrates — that will take society-wide efforts to reverse, [Centers for Disease Control and Prevention Director Thomas] Frieden stressed. His agency last week released a list of strategies it wants communities to try. They include: increasing healthy foods and drinks in schools and other public venues; building more supermarkets in poor neighborhoods; encouraging more mothers to breast-feed, which protects against childhood obesity; and discouraging consumption of sodas and other sweetened beverages.
If you allow the government to take responsibility for your health, then any activity affecting your health becomes a public act. The consequence of this shift will take decades to work its way through the culture, but its metastasis through the organs of our freedom will be inexorable.
July 23, 2009
Health... of the Nation, of the State, and of the Town
On last night's Matt Allen Show, Monique and Matt covered the travesty that is healthcare "reform," the travesty that is underage exotic dancers in Rhode Island, and the travesty that is the Caruolo lawsuit in Woonsocket. (If I may interject: perhaps there's a solution to be found, among these three issues, if the government requires strip clubs to pay for family health insurance for their dancers and applies an additional payroll tax for those in-demand minors, which money would be cycled back to school districts to cover unwise contractual agreements. Sure, such a plan would represent an exploitation twofer, but the teachers' unions might have something to teach us about maximizing the value of the resource of communities' children.) Stream by clicking here, or download it.
July 22, 2009
The Disclaimers Are Always the Thing
It is definitely not our practice to run political ads for political reasons (or only for political reasons), but this one from the Republican National Committee on the healthcare legislation is funny enough to merit a few minutes of your time.
As one might expect, the "side effects" disclaimer is the key.
America's Elected Geniuses
John Stossel shows that it doesn't take but a little of that common sense of the right-wing variety to produce an "oh" moment:
It's crazy for a group of mere mortals to try to design 15 percent of the U.S. economy. It's even crazier to do it by August.Yet that is what some members of Congress presume to do. They intend, as the New York Times puts it, "to reinvent the nation's health care system".
Let that sink in. A handful of people who probably never even ran a small business actually think they can reinvent the health care system.
Expressing fear that Americans will fail to be sufficiently incensed to put a stop to the lunacy, Stossel quotes some of his blog commenters who offer the predictable retorts, which one may paraphrase as "we've got to do something for the uninsured" and "you're just backing rich interests." The first is open ended, and the second is irrelevant.
When building a particular system, as part of a larger society, we begin with a goal and seek the most direct path. But when we come upon a principle that, if ignored, would inherently corrupt our design, we must turn to alternate routes. The decisions at each intersection are what ultimately constitute our divided political philosophies, and on this particular issue, too many people wish to march straight through the warning signs, ensuring that we'll arrive at our destination bloodied and infected (and with the availability of treatment severely curtailed).
It would be wonderful if we could simply hand our elected representatives the directive to just "make it so" and trust that they would manage a workable solution. That isn't reality.
July 19, 2009
Preventive Totalitarianism
Stated in passing — as an inarguable truism — is the most eerie part of President Obama's recent healthcare remarks (video, at about minute two):
We're now at a point where most everyone agrees that we need to invest in preventive and wellness programs that can save us money and help lead healthier lives.
Put aside that some folks — John Stossel among them — do question the "preventive care" shibboleth. One gets the sense that what Obama is saying and what many Americans will hear are two different things. To my ear — and I offer this without intending to express favor for any particular policy — an "investment" in such programs means funding to make them available, with the option of whether to partake left up to the individual. General experience suggests that, when government officials use the term "investment" in this context, they mean at the very least some form of compulsion, as in: "We'll subsidize your healthcare, but you must do X and must not do Y."
Let's be clear about what's going on conceptually. The premises on which the debate is being framed are that private healthcare is en route to pricing itself out of the reach of a broad swath of our society and that the portions of the industry directed by the government are finding costs unsustainable. By "investing" in "wellness programs" as a means of lowering costs, the government would be putting the weight of the nation's entire healthcare system on individual citizens' behavior. What couldn't be declared intolerable with such a consequence as the collapse of everybody's medical care?
The national and state governments have already instituted the practice of disincentive taxes (as on cigarettes), they regulate what plans must cover, and so on. Imagine what political leaders will do when they can dictate health-related behavior directly, especially if it remains a commonplace that preventive care is key to affordability. With the passage of Rep. Patrick Kennedy's healthcare "parity" bill, eliding the distinction between mental and physical ailments, "health-related behavior" would be tautological. We can only imagine what behaviors and life decisions will qualify a person to be locked out of the healthcare system.
President Obama illustrated his perspective on the ownership rights of a government "investor" when he changed the leadership of GM. In like fashion, healthcare "reforms" that entail greater involvement of the government and greater reliance on its "investments" will inevitably prove to be about the very ownership of individual Americans. One already reads stories from other nations of rationing based on habits like smoking, but the principle needn't halt there.
It's certainly objectionable enough that mandatory coverage of abortions appears now to be a component of the Senate bill. What begins as a "medically appropriate" option could easily make the transition to classification as "most appropriate" — say for one of those inspiring mothers who, under the current system, accept the risk of their own lives for their children's births or for those who choose not to kill their unborn offspring despite known disabilities. When a centralized government becomes a "single payer," those risks and those offspring are a burden to the whole system. One can hear the argument that they're free to do so, but that society cannot be expected to pay for "excessive" procedures during birth, let alone a lifetime of specialty care.
We daren't even contemplate the possibility that women with psychological problems (religious views considered to be extreme, for example) may be deemed ineligible to bring children into the world. We further daren't consider that a government empowered to tell its healthcare dependents what risks they are not permitted to take may, given circumstances, quickly decide that it also holds the prerogative to place risks before them — whether of a martial or occupational character. For the time being, it is enough simply to acknowledge that the party that pays is the party that controls and that to control a person's health is to control the person.
July 18, 2009
Wasn't This Guy Supposed to Be Smart, Moderate, and Temperate?
This bit of cynicism should be beneath the cool-headed genius whom we elected president:
Obama countered yesterday that "if we step back from this challenge at this moment, we are consigning our children to a future of skyrocketing premiums and crushing deficits. If we don't achieve health-care reform, we cannot control the costs of Medicare and Medicaid, and we cannot control our long-term debt and our long-term deficits."
"Our children" (in this cliché) have years before adulthood and will not be consigned to anything by some months of research and debate. There is no milestone pending in the next few weeks or months that will lock in costs. Unless, that is, the federal government does act and institutes a mess of an oppressive power grab like the plans that are on the table.
July 15, 2009
The Depression Is Coming! The Depression Is Coming!
It really is astonishing. With the economy flailing and the trends in job losses disappointing even the whiz kids of the Obama administration, despite its having whipped out the "stimulus" credit card, with "cap and trade" energy policy seeking to raise the cost of doing business (and of simply living), the Democrats are hitting the accelerator pedal on their hybrid healthcare suicide car:
The liberal-leaning plan lacked figures on total costs, but a House Democratic aide said the total bill would add up to about $1.5 trillion over 10 years. The aide spoke on condition of anonymity to discuss the private calculations. Most of the bill's costs come in the last five years after the 2012 presidential election.The legislation calls for a 5.4 percent tax increase on individuals making more than $1 million a year, with a gradual tax beginning at $280,000 for individuals. Employers who don't provide coverage would be hit with a penalty equal to 8 percent of workers' wages with an exemption for small businesses. Individuals who decline an offer of affordable coverage would pay 2.5 percent of their incomes as a penalty, up to the average cost of a health insurance plan.
Pay down. Employment down. Prices up.
Note that admission that the legislation's cost structure attempts to move the bill past the next presidential election. Consider also that the bulk of the stimulus money is scheduled for dispersal next year — an election year. One doesn't have to be partisan to wonder whether economic hardship and civic anxiety are being tolerated in the service of a planned political script. A few eggs must be broken, after all, in order for the Left to make the governmental omelet that the country doesn't yet know it needs.
July 14, 2009
When the Last Bastion Falls
On healthcare, as on several other issues, it's long been my contention that the touted (but debatable) successes of other nations are heavily dependent about the United States of America being its different self. That's one of the points worth taking from Peter Morici's op-ed on healthcare reform:
Americans subsidize health care globally by paying most of the costs for developing new drugs. Single payers in Canada and elsewhere force drug companies to charge little more than manufacturing and marketing costs, and they must recoup all their development costs by charging Americans oppressive prices.
And what should we expect to happen if the U.S.A. no longer stands as a revenue opportunity for drug developers? Correct: They'll develop fewer cutting-edge drugs. As much as doctors and scientists may want to develop new treatments, everybody's got to make a living, and the profit motive has brought them the funding they require.
A second point of Morici's touches on another common theme of mine:
Unlike U.S. health-insurance companies, single-payer systems abroad don't pay executives salaries in the millions, impose multiple systems of private rationing second guessed by buccaneering lawyers, and create massive paperwork burdens to justify high rates.Americans have created a "competitive market" for private insurance that is less efficient than the French bureaucracy. What a triumph of free enterprise!
What healthcare needs is not more regulation — even unto the extent of making the entire industry a government enterprise — but deregulation. The higher the hurdles, the more advantage those with the resources to jump them will have.
The third point I'll leave directly quoted, without comment:
My very expensive education in economics tells me: When prices are too high for an essential service, subsidizing purchases for those who can’t afford it increases demand and pushes prices up even more.Americans will be stuck paying both higher health premiums and new taxes.
An Image and a Corrective on Healthcare and the Economy
Ben Stein presents an excellent image:
True, by many metrics, the economy has stopped falling drastically, but we are still in a painful recession, large by postwar standards. The bank crises seem to have abated for now and Wall Street is paying itself fantastically well again, thank heavens, after being rescued with taxpayer money. But housing is still extremely weak, profits are miserable and, most important, far too many Americans are unemployed — roughly 9.5 percent, by the latest data.Just as basic, far too many Americans are living in fear.
What is President Obama doing about it? Perhaps too much. And, possibly, his efforts are too diffuse. When I think about the economy I think about a plump man who has just been hit by a truck while crossing a street and is in severely critical condition with internal bleeding. Instead of just stabilizing his hemorrhaging, the doctor decides that while the patient is unconscious, he might as well also do a face lift, some coronary bypasses and a stomach-stapling to keep him from gaining weight while he is recovering (if he does recover). After all, a crisis is not to be wasted.
The problem is that all these ambitious operations create too much of a burden for the human body to bear.
It's an old truism that one shouldn't go grocery shopping while hungry. Similarly, one shouldn't make dramatic financial decisions while panicked about paying a surprise bill. With the amped up call for extreme healthcare changes to be pushed through Congress with a minimum of deliberation, one can't help but wonder what makes the matter so dire that it must be forced through Congress in the distracted days of summer immediately before a recess. Are masses dying in the street for lack of a "public option"? It isn't unreasonable to suggest that such an outcome is much more likely if unemployment continues to mount — especially if new healthcare requirements increase the cost of employment for employers.
No, in theory, the urgency derives from a series of jumbled abstractions:
"The status quo on health care is no longer an option for the United States of America," the president said. "This is no longer a problem we can wait to fix. This is about who we are as a country. Health care reform is about every family's health, but it's also about the health of the economy."
In actuality, the urgency derives from a political necessity to rope Americans into a framework of dependency on government while we're susceptible to panic, under the thrall of a charismatic political celebrity, and as yet unable to assert regained senses through an electoral correction.
July 13, 2009
Who Isn't Covered?
Here's an interesting paragraph from a Mark Steyn piece in the current print edition of National Review:
There have been two trends in U.S. health care over the last decade. On one hand, a lot of Americans have become, by any rational standard, overinsured: They get tested for things they'll never get. On the other, there has been an abandonment of health insurance by the rich. If you peel the Census Bureau and DHHS figures, of those alleged "45 million uninsured Americans," one-fifth aren't Americans; another fifth aren't uninsured but are covered by Medicare; another two-fifths are the young and mobile (they don't have health insurance, but they don't have life insurance or home insurance, either — they're 22 and immortal and life's a party); and the remaining fifth are wealthier than the insured population. Really. According to a 2006 Census Bureau report, 19 percent of the uninsured have household income of over $75,000. Since the last round of government "reform" in the Nineties, wealthy Americans have been fleeing insurance and opting to bring health care back to being a normal market transaction. And if you look at the "uninsured discount" offered by doctors, one can appreciate that, for everything but chronic disability, it's not an irrational decision to say I'll get a better deal on my broken leg or my colonoscopy or my heavy cold if I just write a check for it.
That last fifth points in the direction that we ought to head: insurance for catastrophe, and a pay-as-you-go system for regular care. No employer involvement. No broad-based "public option," except to assist those who cannot afford catastrophic coverage.
The entire structure of the industry would change. Consider, for example, that the majority of procedures and expenses would no longer be tied to negotiated pools, because the emphasis would no longer be on distributing risk for the great bulk of procedures. Those with preexisting conditions would have less fear of losing their coverage, because their conditions would be partly what the catastrophic coverage is for (and independent from unrelated aspects of life, such as employment) and partly under the umbrella of regular care.
(If the above link doesn't work for you, try here.)
July 8, 2009
A Cost to Racial Denial
Race is not purely a matter of hue. Evidence from sports aptitude to facial bone structure proves it to be so, and denying that fact in the name of racial harmony makes it more difficult to solidify the cultural holding that the differences don't matter in a philosophical or legal context. It may also make it more difficult to analyze and eliminate differing success rates of medical treatment:
African-Americans are less likely than whites to survive breast, prostate and ovarian cancer even when they receive equal treatment, according to a large study that offers provocative evidence that biological factors play a role in at least some racial disparities.The first-of-its-kind study, involving nearly 20,000 cancer patients nationwide, found that the gap in survival between blacks and whites disappeared for lung, colon and several other cancers when they received identical care as part of federally funded clinical trials. But disparities persisted for prostate, breast and ovarian cancer, suggesting that other factors must be playing a role in the tendency of blacks to fare more poorly.
Astonishingly, even the chief medical officer of the American Cancer Society is quick to validate concerns not about the research's results, but its being publicized in the first place:
"When I hear scientists talking about racial differences, I worry that it starts to harken back to arguments about genetic inferiority," said Otis Brawley, chief medical officer of the American Cancer Society.
The message that we all ought to hammer home repeatedly is that even genetic differences don't mean inferiority when it comes to our individual value as human beings.
July 1, 2009
Preparing to Stick It to Doctors
Listening to the federal conversation about healthcare "reform" as it takes shape, one notices that some of the problem, specifically with the shortage of primary care doctors, appears to have been the government's handling of its own piece of the industry:
The disparity results from Medicare-driven compensation that pays more to doctors who do procedures than to those who diagnose illness and dispense prescriptions. In 2005, for example, Medicare paid $89.64 for a half-hour visit to a primary-care doctor in Chicago, according to a Government Accountability Office report. It paid $422.90 to a gastroenterologist who spent about the same amount of time performing a colonoscopy in a private office. The colonoscopy, specialists point out, requires more equipment, specialized skills and higher malpractice premiums.
Given the proclaimed movement of most doctors toward specialties, one would expect the law of supply and demand to make up some of that 472% difference all on its own. Instead, the government looks intent on fighting that economic law:
In the various legislative proposals under debate, Congress and the administration have moved toward providing incentives for doctors entering residency programs to pursue careers in primary care. Most residency slots are funded through Medicare, giving the government a stick to wield over residency administrators, and changes in Medicare reimbursement alluded to by Obama on Monday could be the carrot that makes primary care more attractive.
The promise is to increase both the supply and the pay of primary care doctors. We don't have to perform extensive analysis to suspect that there might be market repercussions to that sort of distortion. (That assumes, of course, that the government doesn't try to cover all of the increased remuneration with new money for the industry.)
Here's the general shape of what I would suggest: Decouple health insurance from employment, remove coverage mandates, reform tort law, and require catastrophic coverage. Some consumers will use the increased money from their employers to finance similar plans to what they currently have, while others will go for the minimum coverage. Competing for those dollars, insurance companies will design plans to attract individuals, with healthier individuals being especially desirable; one aspect may be a certain number of routine visits (i.e., primary care) for free, or for low cost. The focus will shift from insurers' catering to payers to their having to address the desires of consumers and accommodate the doctors whom consumers wish to see.
At the same time, since insurance will become insurance again (rather than something more resembling a healthcare financial management service, as it is now), some portion of consumers will need or want to pay directly for routine visits. Doctors will have more responsibility, therefore, for setting their own fees, and they'll develop a base of clients whom neither insurers nor government payers can use as a stick to dictate payments or behavior.
More people will leverage primary care service, driving up the demand and, therefore, the doctor's fee. Increased demand, pay, and regularity will give primary care doctors more control over their practices and their lifestyles and will attract more practitioners.
Meanwhile, demand for the services of specialists will go down because people will catch more during primary care visits. They'll also have a more direct sense of how their health affects the cost of their healthcare. They'll also be less inclined to turn to specialists at every possibility.
June 30, 2009
Something Not to Forget on Rising Healthcare Costs
There are more problems with our healthcare system than this allows, but Thomas Sowell's point is well worth remembering:
Just as medical care, houses, and cars were all cheaper when they lacked things that they have today, so medical care in other countries is cheaper when it lacks many things that are more readily available in the United States.There are more than four times as many Magnetic Resonance Imaging units (MRIs) per capita in the United States as in Britain or Canada, where there are government-run medical systems. There are more than twice as many CT scanners per capita in the United States as in Canada and more than four times as many per capita as in Britain.
Is it surprising that such things cost money?
The cost of developing a new pharmaceutical is now about a billion dollars. Neither political rhetoric nor government bureaucracies will make those costs go away.
We can, of course, refuse to pay these and other medical costs, just as we can refuse to buy air-conditioned homes with built-in microwave ovens. But that just means we pay attention only to prices and not to the value of what we get for those prices.
June 28, 2009
Taxing Health Care
One idea that has been floated as part of comprehensive health care reform is to tax health care benefits as income. I recall Senator McCain's plan contained such a provision for example. Well, it looks like the Senate is considering going with it, too. Except for union workers.
The exception, which could make the proposal more politically palatable to Democrats from heavily unionized states such as Michigan, is adding controversy to an already contentious debate. It would shield the 12.4 percent of American workers who belong to unions from being taxed while exposing some other middle-income workers to the levy.Sheesh. There's no way to see this as other than fundamentally unfair. But some unions think it's fine:“I can’t think of any other aspect of the individual income tax that treats benefits of different people differently because of who they work for,” said Chris Edwards, director of tax policy studies at the Cato Institute, a Washington research group that often criticizes Democrats’ economic proposals. Edwards said the carve-out “smacks of political favoritism.”
Gerald Shea, an AFL-CIO official lobbying for health-care reform, said grandfathering benefits negotiated in a collective bargaining agreement is a “common thing when there is a big change in federal law.”We're quite familiar with that mindset, aren't we? However, there are some unions who do oppose the idea:“Once a collective bargaining agreement is set, employer’s budgets are set, workers expectations are set. It doesn’t make sense to go back in the middle of the contract and change it,” he said.
Union groups and workers said Congress shouldn’t target contractually negotiated benefits.
Anna Burger, secretary-treasurer of the Service Employees International Union, said in an interview that workers have often traded salary increases for better benefits in agreements.
Taxes “shouldn’t be taken from the backs of workers who have bargained away wages and other things for their benefits over the years,” Burger said.
Other unions say they’re opposed to a tax on some employer- provided benefits, regardless of whether collective bargaining agreements are exempt.Interesting.“Either way, we are against a tax on health-care benefits in whatever form it takes,” said Jacob Hay, spokesman for the Laborers’ International Union of North America. The union represents 500,000 workers, largely in the construction industry.
June 27, 2009
When the Government Faces Healthcare Reality
Put aside aspersions against health insurers, whether for-profit or (ahem) non-profit, because it simply isn't credible to assume that government bureaucrats won't be corrupt and selfish. What, then, will the government response be when it faces these forces as a (or the) national healthcare financier:
"We understand that many of our members are suffering in the current economic conditions, but the fact is that rising medical costs and increased utilization of services are climbing faster than our rates," James E. Purcell, president and CEO, said in a statement. "Quite frankly, the OHIC [Office of the Health Insurance Commissioner] is putting the state's oldest nonprofit health insurer at financial risk by denying our filing. We simply cannot afford to lose $125 million."
Cost controls. Service limitations. Tax increases. The government can't make human nature what it is not, and it cannot mandate an end to market forces. What it can do is jail those who don't follow its instructions, so people will try to play along, no matter how detrimental certain policies are.
June 17, 2009
Who's the Boss of Primary-Care Doctors?
I've read the editorial several times, and it still isn't clear to me how or why the Projo writers avoided mentioning the problem of liability insurance for primary-care doctors.
Shortly after I moved to Tiverton and found a nice local doctor to visit, he packed up and left the state for sunnier climes. My understanding is that the cost of insurance and the threat of being sued in Rhode Island were motivating factors. (It worked out, though, because it got me on the list of the practice's senior doctor, who hadn't been accepting patients when I inquired.)
Primary-care physicians seem to mirror a small-business model more than specialists do. People will travel farther for specialists, and their work is more likely to come to them via the referrals of other professionals. I'm sure there are other distinctions (such as the closeness of relationships with hospitals), but I don't want to delve too deeply into guesswork. The point is that, as our society considers healthcare policy, we ought to think of primary-care providers in the same way that we think of other self-employed professionals.
Market and deregulatory incentives can encourage the occupation without bureaucracies meddling, as the Projo winds up suggesting:
Alan Sager, a health-policy expert at the Boston University School of Public Health, has suggested paying primary-care doctors $250,000 a year to work under a capitation system. The doctors would be earning considerably more than they do now. And because they would treat a set number of patients at a fixed yearly cost, adjusted for medical risks, the doctors would have no financial reason to offer more care than necessary.
Question number one is who will set and process the numbers of patients and income? By default, it would have to be the government, which means that doctors will no longer work for themselves, but for the folks who can give them raises and who can cut their pay or increase their work burden. I'd worry about the sorts of practitioners such an arrangement would attract, as well as the institutional focus that would shift to lobbying the authorities for more.
Question number two is what would provide incentive — given the rigid quota and salary deal — for doctors to resist the human urge to do as little as possible? If the five patients whom I have to see in an afternoon (hypothetically) don't pay me and their return is not really my problem, I might just take the opportunity of a sunny day like today to rush through my itinerary and get out of the office. (Of course, for a reality check, I get to be outside all day anyway... digging post holes and mixing concrete.)
As I said, the editors don't provide the "who," but what they propose amounts to another increment of socialization, and in that respect, it provides another instance of the plain inadvisability of such a system.
June 16, 2009
"The Federal Government ... Is the Health Care Equivalent of Bigfoot"
Fred Thompson pointed out this afternoon that even the Chicago Tribune has doubts about President Obama's proposed expansion of the federal government as a health care insurer.
But we do know a few things about government-run health plans. We draw upon decades of experience with Medicare, the government's plan for the elderly, and Medicaid, which provides coverage for the poor.We know those plans pay bare-bones rates and yet still are busting the federal budget. One part of Medicare will be insolvent in 2018 if nothing is done. States are staggering under Medicaid costs. We know, as the president said in his AMA speech, Medicare and Medicaid spending will "grow over the coming decades by an amount almost equal to the amount our government currently spends on our nation's defense." And that "it will eventually grow larger than what our government spends on anything else today."
That's scary. Costs clearly need to be controlled. But the Democrats' solution to all this government excess is to create . . . another government-run health plan.
The Worms Come Out When It Rains on Healthcare
These people aren't fit to lead:
[A citizen] opposed the [health insurance] rate hikes, as did other speakers including Lt. Gov. Elizabeth Roberts and state Rep. Edwin Pacheco, D-Burillville. Roberts, who has been working with business leaders, opposed any hikes until the state can develop a plan for affordable health care. Pacheco and Assistant Attorney General Genevieve Martin, speaking on behalf of Attorney General Patrick C. Lynch, both criticized Koller for not holding a formal rate hearing, in which evidence for and against the rate hikes is presented and witnesses testify and face cross-examination. The lack of such a hearing, said Martin, "is an injustice to the people of this state."
Her suggestion of explicitly freezing hikes until Rhode Island legislators institute significant reform is perhaps the strongest argument that Roberts has made against her candidacy for governor. If anything, such a policy would delay reform, as unrest fizzles in the face of steady rates.
More important, however, is the utter lack of leaders with a clue as to the appropriate shape of reform. Why not suspend policies that are contributing to escalating costs? Why not investigate the reason that Rhode Island has as many branches of government as healthcare insurers?
Every week it becomes more incomprehensible that Rhode Islanders continue to vote the way they do.
June 15, 2009
The Only Reason to Put Government in Healthcare Is to Put Government in Healthcare.
A healthcare reform suggested by Sen. Kent Conrad (D, ND) sounds reasonable, but I'm not sure why it should be so limited:
The Conrad proposal is modeled after rural electricity, farming and telephone cooperatives that are owned and organized by members. The entities would negotiate rates with health-care providers and would have to meet the same licensing and regulatory requirements as private insurance companies, the senator said."I tried to come up with something that is not government-controlled, is a competitive delivery model, but nonprofit," Conrad said in an interview. "It would be on a level playing field with everybody else with, with a different ownership structure."
Sen. Charles E. Grassley (Iowa), the ranking Republican on the finance panel, said he likes the Conrad plan, and said Obama raised no objections when the issue surfaced at the Wednesday White House meeting. Sen. Mike Enzi (Wyo.), the ranking Republican on the Senate health committee, the other panel with jurisdiction over reform legislation, said he is seeking more details. He said the co-op approach could "increase the level of competition, if it were done right."
We're over-thinking this. Sure, let such co-ops form. Let insurance companies develop ready-made products for them, if they like. More broadly, though, we should open up healthcare beyond employers (largely by repealing or adjusting ERISA) and allow any group that wishes to offer health coverage do so. Churches, charities, social groups, whomever — if it serves a group's mission to help its members or others to procure health coverage, let them do so.
There's no need to involve the government in medical services beyond a mild regulatory hand — unless, of course, expanding government is actually the first priority.
A "Safeway" Towards Health Care Reform?
Safeway CEO Stephen Burd explains:
While comprehensive health-care reform needs to address a number of other key issues, we believe that personal responsibility and financial incentives are the path to a healthier America. By our calculation, if the nation had adopted our approach in 2005, the nation's direct health-care bill would be $550 billion less than it is today. This is almost four times the $150 billion that most experts estimate to be the cost of covering today's 47 million uninsured. The implication is that we can achieve health-care reform with universal coverage and declining per capita health-care costs.What was the "Safeway"? First, they focused on encouraging healthy behavior:
Safeway's plan capitalizes on two key insights gained in 2005. The first is that 70% of all health-care costs are the direct result of behavior. The second insight, which is well understood by the providers of health care, is that 74% of all costs are confined to four chronic conditions (cardiovascular disease, cancer, diabetes and obesity). Furthermore, 80% of cardiovascular disease and diabetes is preventable, 60% of cancers are preventable, and more than 90% of obesity is preventable.Thus, they designed a voluntary "Healthy Measures" program, which requires employees to be tested for the aforementioned chronic conditions. If they "pass" all four tests--the information is not shared with management--they receive a rebate. If they don't pass, they can make adjustments and retake the test (so to speak) in a year. According to Burd, "the numbers speak for themselves."
Our obesity and smoking rates are roughly 70% of the national average and our health-care costs for four years have been held constant. When surveyed, 78% of our employees rated our plan good, very good or excellent. In addition, 76% asked for more financial incentives to reward healthy behaviors. We have heard from dozens of employees who lost weight, lowered their blood-pressure and cholesterol levels, and are enjoying better health because of this program. Many discovered for the first time that they have high blood pressure, and others have been told by their doctor that they have added years to their life.Sounds like a win all around.
June 14, 2009
Healthcare Reform: Easy as One, Two, Minus Three
Who knew finding twelve digits of savings in the healthcare industry would be this easy?
The administration expects to achieve the lowered hospital payments in two major ways. First, said Obama's budget director, Peter Orszag, payments to hospitals will be reduced to try to encourage them to work more productively and efficiently.Orszag said hospitals could figure out ways of treating patients "more effectively, through health information technology, a nurse coordinator instead of an unnecessary specialist," for example. These "productivity adjustments" would account for $110 billion in savings.
If you cut it, they will innovate! Or maybe cease to provide, but we won't dwell on that. We also won't consider why price controls on hospitals will spur desirable efficiencies, but reducing the burden on patients to pay more directly for the services that they use won't exacerbate waste on their part. (The key, we can imagine, is in the consumption controls that are visible a few more steps along the process.)
June 12, 2009
"We're From the Government and We're Here to Help"
James Poulus observes:
I’ve said elsewhere that our vision of politics is being corrupted by a well-meaning but misguided epistemology of compassion: increasingly, we consider the person or group demanding a right to be the most trustworthy source of information about whether they deserve it. Anyone aggrieved, we think, must really be suffering grief, and since suffering is the worst thing and cruel is the worst we can be, justice is served when the law — that is, judges — fast-track the claims of the aggrieved and grant them instant — that is, legislature-circumventing — relief.This leads into an observation by Keith Hennessey on private industry competing with government (ie; as proposed in the proposed health care reform):This is pretty transparently a medical way of viewing social relations. But our big medical brains are wired into big therapeutic hearts. And so what is happening in ‘politics’, which is actually the evacuation of politics by law on the one hand and desire on the other, is happening in medicine itself.
I think that government cannot compete on a level playing field with the private sector. Government always has advantages because of its sovereign power. I also think that in most markets there is a range of private health insurance plans competing for business, and so the addition of one more plan is not worth the downsides of government involvement. (I believe that competition is flawed because for most people their employer shops for health plans. I prefer a system in which individuals are shopping for health plans.)In other words, when government is involved--whether as a service provider itself or with a vested interest in particular entities within a given business sector--private companies without government help are at a disadvantage. Yet, some may welcome government intervention, according to Poulos:The government cannot compete on a level playing field with private firms:
* Fannie Mae and Freddie Mac had competitive advantages relative to their purely private counterparts. They leveraged those advantages to the gain of their management and shareholders until they collapsed and jeopardized the entire financial system.
* Ford Motor Company was not bailed out. It is now disadvantaged relative to GM and Chrysler, which benefited from government oversight, funding, and effective rewriting of bankruptcy rules.
* Government-provided terrorism reinsurance is preventing private reinsurance from returning to the marketplace.
* Most physician- and hospital-reimbursement structures are based on the methodologies of the largest payor in the market, Medicare.
* Government-run direct student loans are now crowding out the guaranteed student loan program, in which private banks and financing firms offer loans. The government advantage comes from control over small details of the program that give direct loans a competitive advantage.The ultimate fear of having a government-run “public” option is that it will crowd out private health insurance, and that ultimately most Americans will be getting their insurance from the government.
Big Pharma has a vested interest in comprehensive government regulation, too, you know — the better to squeeze out competition, get institutionalized with an unkillable monster of market share, and permanently hedge, by way of unremittant lobbying and revolving-doorism, against market risk or corporate accountability.What both illustrate is that the while government doesn't always actively pick winners, its insertion into markets results in preferred policies and "suggestions" that ultimately lead to losers: Either businesses that don't benefit from government largesse (Ford) or consumers who are affected as services are adjusted to comport with the new business model.
A Prescription for Me Time
That's being a Congressman, for ya. Patrick Kennedy hopes to get back to work from a mental health retreat "in time for the... debate on a national health-care overhaul later in the summer." Presumably, he needn't expend any hope on whether the checks from his $174,000 salary will keep arriving, whether or not he manages to participate in the healthcare debate.
Look, without any information about what inspired Kennedy's decision, one can still say that it was probably the intelligent one to make. A person's health is paramount. The idea that somebody who holds an ostensibly important job can just "step away" like this raises questions about what they do, and who should be doing it.
Frankly, having stood on the incisors of alcohol abuse and stared into a dark psychological gullet, I see far too much permissiveness in this prescription explained by Kennedy friend Ronald Smith:
Smith said medical research has found increasing evidence that in early recovery, which he defined as two to three years, it is essential for addicts to recognize when they face "stressors" such as fatigue or illness or family problems. "You have to go back, take a couple of days off and renew your sobriety," he said.
As a matter of principle, I don't believe a solution calling for the avoidance of problems fosters the necessary change in outlook. Moreover, to the extent that a person is in the precarious position of having to avoid "stressors," his first step should be away from a high-stakes job like U.S. legislator.
June 10, 2009
Analyzing the Healthcare Reform Proposals
Blogger Keith Hennessey, a former White House Senior Economic advisor, has been providing details of the various Federal healthcare reform proposals under consideration, as they become available.
His summary of what he's seen so far is…
- The government would mandate not only that you must buy health insurance, but what health insurance counts as “qualifying.”
- Health insurance premiums would rise as a result of the law, meaning lower wages.
- A government-appointed board would determine what items and services are “essential benefits” that your qualifying plan must cover.
- You would find a tremendous new disincentive to switch jobs, because your new health insurance may be subject to the new rules and would therefore be significantly more expensive.
- Those who keep themselves healthy would be subsidizing premiums for those with risky or unhealthy behaviors.
- Far more than half of all Americans would be eligible for subsidies, but we have not yet been told who would pay the bill.
- The Secretaries of Treasury and HHS would have unlimited discretion to impose new taxes on individuals and employers who do not comply with the new mandates.
- The Secretary of HHS could mandate that you provide him or her with “any such other information as [he/she] may prescribe.”
The Coming Healthcare Monster
It isn't difficult to predict the effects of this. On one side:
A first-ever tax on employer-provided health benefits also figures prominently among options under consideration in Congress, but Obama campaigned against that last year and its inclusion in the bill would require him to reverse course. ...... Private companies would be barred from denying coverage or charging higher premiums because of pre-existing conditions.
Both bills would require individuals to purchase insurance if they could afford it, with waivers available in hardship cases. The Senate measure provides for an unspecified penalty for anyone refusing to obey the so-called mandate, and House Democrats are considering a similar approach. ...
... the House approach would require employers to purchase insurance for their workers or pay a penalty. ...
To cut down on the ranks of the uninsured, the Senate bill stipulates that children up to the age of 26 could remain on their parents' insurance policies.
And filling in the other:
Individuals would be able to purchase insurance from new exchanges operated by the states or federal government. ...On a hotly contested issue, the emerging House plan would give individuals the option of buying insurance provided by the federal government.
The president's assertion that the healthcare plan will be "revenue neutral" is an Orwellian kind of insulting. The tax on employer health benefits and all these penalties (paid to whom?) for failure to provide or to procure mean that the plan is — by design — not "revenue neutral" for anybody but the regime in Washington. Apart from the direct confiscation of money, they will lead to decreases in pay (as employers compensate for the greater cost of benefits) and increases in the price of goods and services (as companies try to make up for costs of producing them).
Moreover, the inability of insurance companies to adjust prices to account for pre-existing conditions and the ability of young adults to remain on parents' plans to the age of twenty-six are only two predictable ways in which this legislation will drive up the cost of insurance. Since the aforementioned penalties will hardly keep up with inflation, an increasing number of companies will opt to pay them rather than to provide the benefit, and an increasing number of individuals will have no plausible option but government care. So, the government program will grow, and if it remains "revenue neutral" by desire or by fiscal reality, price controls will be ramped up and rationing will begin. If it does not remain "revenue neutral," it will drive Americans into the ground.
Those who've pined for government healthcare are going to get a good look at it within the next decade, and I doubt they'll like what they see... at least when they find themselves needing to rely on it.
June 5, 2009
A Taste of the Future of Medicine?
Long wait times will likely be more characteristic than lotteries, but somehow this strikes me as an extreme vision of the future of healthcare for the average American in a government-run system:
At 4 p.m., volunteers from the clinic came out with a roll of carnival-style paper tickets. They handed each person a ticket and asked them to put their name and number on the stub.Someone else handed out sheets of paper with the rules in English and Spanish: the Free Clinic is only for people who have no health insurance. They must prove that their income is less that 150 percent of the federal poverty level — that is, less than $2,200 a month for a family of three. The Free Clinic does not care for children 18 and younger, nor does it provide obstetrical care to pregnant women.
Lynne Urbani, the president and chief executive officer of the Rhode Island Free Clinic, addressed the group, saying she would be drawing 14 names in a few minutes, about half as many as usual because there were fewer volunteer doctors available this night. With a translator, she asked them to affirm that they have no insurance and have a ticket in their hand. They nod in agreement. Those whose names are pulled should expect to stay till 9 p.m. Those who aren’t chosen will get a call offering them an appointment; the next opening is in July.
If prices are set, the medical industry will attract fewer professionals. If tax dollars (in one form or another) are the method of payment — filtered through the government bureaucracy — there will be rationing and long delays as financing and demand fail to balance.
In healthcare, we've got a product that people tend to see as an inconvenience when they're healthy and as a dire necessity when they're not. The more the system separates those who pay from those who receive, the more effort paid employees will have to allocate for determining priorities or the more they'll disregard that responsibility and rely on cold process and chance.
June 3, 2009
Government Doesn't Count as a Monopolist?
What's vexing is that Herchell Talan of North Kingstown has the basic principle right but comes to a statist conclusion anyway:
In the past 13 years, health-insurance companies have merged with each other at a frightening rate, and now a small number of companies dominate local markets. Rhode Island basically has two insurers: Blue Cross and Blue Shield of Rhode Island and United HealthCare. The data in the report show how much of states' markets are controlled by one insurance company. Indeed, 94 percent of insurance markets in America are controlled by one or two companies, a near-monopoly under Department of Justice definitions.We need more competition. By giving us a choice of a public health-insurance plan that's available to everyone, Congress can break the insurance industry's monopoly.
A choice of public health-insurance plans is good for consumers. It will let us choose the plan that meets our needs the best. More competition and choice means more efficiency as insurance plans compete and prices go down.
The government doesn't operate like a private company; competitive forces don't affect it the same way, and neither does its activity affect those forces in the same way. For one thing, a given activity of government doesn't have to be profitable to persist, which is why statists like it so much, because it enables the perpetuation of favored policies even when those policies prove a drain.
The remedy for monopolies (as we've seen in other industries) is to break them up, not to introduce a larger player that doesn't have to meet basic competitive standards. It is all but inevitable that government healthcare will draw the market toward itself until it is a true monopolist. Somehow, I suspect that's not an outcome that Talan fears.
June 2, 2009
John J. Loughlin II: Socialized Medicine - Let’s Look Before We Leap
Our healthcare system is on life support. While the career politicians in Washington have done little, too many Rhode Islanders remain underinsured or uninsured. The system is characterized by rising costs, quality concerns and a lack of patient control. These problems hit the poor and the elderly hardest.
One of the chief reasons is that our healthcare system is governed by a complicated system of laws and regulations forcing patients and doctors through a maze of red tape. You’ll hear a lot in the coming weeks about a new administration socialized medicine program supported by Congressman Kennedy. More government can’t solve this problem because government is the problem.
Socialized medicine resulting in government-run healthcare is exactly the wrong direction for Rhode Islanders. If you think a government-run health system would be easy to use and efficient, I would encourage you to stop by the Registry of Motor Vehicles to see what a government-run system to deliver services would look like. Not a pretty picture. Socialized medicine would bring on more red tape, healthcare rationing and your medical decisions made by Washington bureaucrats rather than doctors. This would all come at an enormous cost in higher taxes and even more money borrowed from foreign governments on the backs of our children and grandchildren.
There are some common sense alternatives that I would encourage Congressman Kennedy to seriously consider as an alternative to government run socialized medicine. One such alternative is called the Patient’s Choice Act. This proposal would allow patients, not government bureaucrats, to choose their health insurance plans and their doctors. Patient’s Choice features preventative measures rewarding Rhode Islanders for choosing healthy lifestyles, with real incentives for states to reduce rates of chronic ailments such as heart disease and diabetes.
Our healthcare system should be easy to navigate and provide integrated care. The best way to achieve this is to create a vibrant health insurance market that is consistent, fair and affordable. New consumer protections would ensure that every Rhode Islander has access to the same benefits that have been enjoyed by Congressman Kennedy for the past 15 years.
The Patient’s Choice Act would protect the most vulnerable Rhode Islanders and ensure that no individual would be turned down based on health or age. Allowing states to pool their healthcare resources and creating reinsurance markets and risk adjustment mechanisms would provide coverage for those Rhode Islanders most at risk. By modernizing Medicaid and Medicare we would give low-income families the same access to high-quality care through direct assistance.
Creating Medicare Accountability Care organizations would also improve payment to our physicians, hospitals, pharmacists and nurses for demonstrable improvements in quality and patient satisfaction while reducing costs at the same time.
Our current legal system does a poor job at compensating patients for medical mistakes in a fair and efficient manner. Instead of creating an environment where medical professionals can openly learn from their mistakes, our legal system often forces doctors and patients into contentious and expensive courtroom disputes. This drives up the costs of health care with staggering costs for medical malpractice insurance we all pay for. Why not put in place a panel of medical experts, patients and healthcare providers to resolve disputes without costly legal fights?
Lastly, our current tax system is stacked in favor of the wealthy and those who get their health coverage through their employers. This discriminates against the self-employed, the unemployed, and small businesses. We need to provide advanced and refundable tax credits in order to increase the amount of money Rhode Islanders can contribute to their health savings accounts.
In short, we need to be very cautious about jumping headlong into a costly and infective socialized medicine government-run system like the one Congressman Kennedy is proposing. Let’s look before we leap and build an affordable system that makes the most of the doctor-patient relationship. We can craft a system to provide universal access to affordable and effective health care, without allowing our well being to be rationed by Washington bureaucrats.
State Representative John J. Loughlin II (R) represents District 71 (Little Compton, Portsmouth, and Tiverton).
May 17, 2009
Oops - Cancel that Projected $2 Trillion in Health Care Savings
Remember that big announcement by President Obama earlier this week that got a ton of coverage?
Barack Obama praised the health care industry's promise to cut $2 trillion in costs over 10 years Monday, taking a sharply different course than President Bill Clinton did 16 years ago in an opening bid to overhaul the U.S. health system.Drawing skepticism from lawmakers, Obama summoned representatives of the insurance industry, doctors, hospitals, pharmaceutical companies and labor groups to the White House for what he called "a watershed event in the long and elusive quest for health care reform."
Actually, not quite. Will the correction get the same widespread coverage?
From Politico via Thursday's Charleston Gazette; h/t Kathryn Jean Lopez at The Corner, National Review Online.
The president of the American Hospital Association said Thursday that a deal with the White House to cut the growth in health care spending has been “spun way away from the original intent.”* * *
... in a conference call Thursday, President Richard Umbdenstock told 230 member organizations that the agreement had been misrepresented. The groups, he said, had agreed to gradually ramp up to the 1.5 percentage-point target over 10 years – not to reduce spending by that much in each of the 10 years, .
So what went wrong? It seems that someone wanted to rush the announcement before the details of what is clearly a difficult, complicated goal had been ironed out.
The comments from Umbdenstock cap a week in which some in the Washington health care world struggled to make sense of the surprise White House announcement Monday. The group of six organizations with a major stake in health care – the Service Employees International Union, the American Medical Association, America’s Health Insurance Plan, Pharmaceutical Research and Manufacturers Association, the American Hospital Association and Advanced Medical Technology Association – had been working in secret for several weeks on a savings plan.But they learned late last week that the White House wanted to go public with the coalition. One health care insider said: “It came together more quickly than it should have." A health-care lobbyist said the participants weren’t prepared to go live with the news over the weekend, when the news of a deal, including the $2 trillion savings claim, was announced by White House officials to reporters. The fact sheet they distributed at the time offered general categories from which the savings would come, but few specifics on how they would be achieved.
May 10, 2009
The First Murmurs of a Healthcare Debacle
It's all very hush-hush, at this point, but our nation's brightest minds — those in the U.S. Senate, of course — are set to point their considerable intellectual prowess in the direction of universal healthcare. Currently, three general plans are on the table:
_Create a plan that resembles Medicare, administered by the Health and Human Services department._Adopt a Medicare-like plan, but pick an outside party to run it. That way government officials would not directly control the day-to-day operations.
_Leave it up to individual states to set up a public insurance plan for their residents.
The Medicare for all discussion has been ongoing for quite some time. Roland Benjamin took a look at it, for example, about a year and a half ago on Anchor Rising. The first link above provides a couple of scenarios that ought to enable any rational person to begin to see the fatal flaws of such plan:
If the public plan were open to all employers and individuals — and if it paid doctors and hospitals the same as Medicare — it would quickly grow to 131 million members, while enrollment in private insurance plans would plummet, the study found.By paying Medicare rates the government plan would be able to set premiums well below what private plans charge. Employers and individuals would rush to sign up.
But the results would be far different if the government plan was limited to small employers, individuals and the self-employed.
In that smaller-scale scenario, the public plan would get from 17 million to 43 million members, the study said. It found that a government plan could be effective in reducing number of uninsured.
In either case, the system would lower incentives and motivation among healthcare providers and surely diminish services and quality. Insurance companies would begin struggling, and folks who maintain private plans will see prices float right past affordability, pushing them into the government net.
If the government outsources administration of this same plan, it achieves no end but creating an additional layer in the process and generating the friction inherent in a system that leaves one group (politicians) to set rules and standards and another to make the numbers work. In other words, it would exacerbate trends that are already too prevalent. And if the feds punt the issue to the states, it would do what big government does best and find the worst of all worlds in the name of expediency.
April 30, 2009
What to Make of the Swine Flu?
It's difficult to know how to react to the swine flu news blitz. Cases around the globe are broadly scattered, but not extensive. The death rate in Mexico, while certainly concerning and, moreover, tragic for those who've lost loved ones, doesn't seem all that high. Yet, the World Health Organization (WHO) has raised its warning level to one step below doom, the story's been on the front page of the Providence Journal for two days in a row (today including a map of the disease's reach), North Kingstown high school has shut down, and several cases have emerged across New England.
Reasonableness would seem to suggest that people not take more extreme precautions than increased hand-washing and such until those maps begin showing hundreds of cases where there are currently a few, but at that point, it could be too late if we're looking at a deadly pandemic. (Although, again, the fact that the peak seems to have been reached in Mexico suggests that it's not a doomsday virus.) We're certainly fortunate, however, to live in a time during which news can spread more quickly than the disease that is its topic.
Without delving into partisan criticism, I will say that this logic, which the president has echoed, strikes me as odd (from the first link above):
"Closing our nation's borders is not merited here," said Homeland Security Secretary Janet Napolitano at a mid-afternoon briefing, echoing comments she made earlier in the day while being pressed by senators at a hearing.She said closing borders or U.S. ports would have enormous adverse economic consequences and would have "no impact or very little" to help stop the spread of the virus.
"This virus is already in the United States. Any containment theory ... is really moot at this time," Napolitano said.
That doesn't really jibe with my notion of containment. Fewer than a hundred people spread across a nation of more than 300 million is substantially less of a threat than travel to a country in which thousands of cases have been confirmed. It's not as if we're a single body that has been infected.
April 23, 2009
A Typical RI Solution for "Solving" a Nursing "Shortage"
Our state is in dire financial trouble based on structural deficits, is on the wrong end of just about every state-by-state comparative list, and is losing its "productive class" by the thousands every year, but the matter of concern for a special legislative commission is, in the words of its Co-chairman Sen. James Doyle (D., Pawtucket):
Even if there are nurses without jobs now, the shortage of nurses, Doyle said, "is going to be a serious issue some day."
Some day. Okay. Let's take that as a plausible reason for at least strategizing methods of increasing the state's supply of nurses. What are some of the problems that must be addressed? Well, there's a reluctance to work more comfortable shifts and in more prestigious locations:
But many graduates want to work only the day shift in a hospital or don't want the less-prestigious nursing-home and home health-care jobs.
Meanwhile, employers are wary of investing in the training of young new hires:
In the hospitals where there are jobs, officials don't want to hire new graduates because they can be expensive to train and there is a fear that, once trained, they will leave to take another job, said commission Co-chair Lynne M. Dunphy, of the University of Rhode Island's College of Nursing.
Perhaps Ms. Dunphy's profession partially explains why the commission contrived such a peculiar means of addressing these specific problems:
A special legislative commission formally unveiled its proposal to give educators in the state's nursing schools an annual $3,500 tax credit, an attempt to keep them teaching so they can make a dent in what the panel said is a looming shortage of nurses in the state.
So, if there's a problem in the nursing profession life cycle, it has to do with matching candidates with difficult-to-fill positions; there's no indication that nursing schools are suffering a lack of students for whose educations they are unable to find teachers; and a legislative commission co-chaired by a nursing educator thinks shaving another "half-million dollars" out of the annual budget to benefit this extremely select class of citizens is the solution.
Yup. That's Rhode Island for ya.
April 22, 2009
The Energy and Healthcare Issues Come Together
Throw in environmentalism, too, because William Tucker's thoughts on windmilled energy bring some possibilities to mind:
The major limitation, of course, is wind's intermittency -- its lack of "dispatchability." Quite simply, you can never count on it. You can't even predict it from hour to hour with 100 percent accuracy and the windiest sites can go calm for days. On a national electrical grid, where supply and demand must be kept within 5 percent or each other in order to maintain voltage balances, this becomes very disruptive. ...The utilities' generating capacity, as McCracken points out, generally falls into two categories -- base load and peaking. Base load runs day-and-night, week after week, to meet the underlying demand. It is almost universally provided by coal plants, which run for weeks at a time before shutting down for maintenance, and nuclear reactors, which can go almost two years between refueling. Peak loads, on the other hand, are generally met with natural gas turbines, which do not boil water and can be started and stopped almost instantaneously.
Unfortunately, as McCracken notes, wind falls into neithercategory. "As wind provides neither baseload nor peaking plant it has no impact on reserve capacity," he writes. ...
In other words, thanks to government mandates and subsidies, wind will be there to throw power onto the market any time the wind blows. This will not replace base load plants but will only drive down prices, cutting into their revenues. Nonetheless, base-load nuclear plants will have to remain in operation, both because they will be needed as back-ups in case the wind doesn't blow or -- in the case of nuclear -- because it doesn't make sense to keep stopping and starting a plant that runs best for two years at a time.
For some reason, this problem joined, for me, with Senator Sheldon Whitehouse's suggestion on Newsmakers that one of the healthcare issues that government must address is obesity. If government takes ultimate responsibility for the healthcare of its citizens, it will gain some right to regulate individual health. What if we put overweight Americans to work generating energy?
Perhaps when the wind dies down, human treadmills could be hooked up to the generator to keep it going. Or, for an even more cartoonish suggestion, perhaps those in need of exercise could turn the wind propellers themselves by dangling off the edge.
March 25, 2009
Healthcare Controls Can Be Natural or Unnatural
In the abstract, there's a dollar amount at which our healthcare system would hum along, factoring in how much employees would demand to do their jobs, how much supplies and operations cost, the expectations and requirements of consumers, their willingess to conserve, and so on. The more we drift from that ideal, the more we'll hear this sort of news:
The study for the Robert Wood Johnson Foundation found that nearly 1 in 5 workers is uninsured, a statistically significant increase from fewer than 1 in 7 during the mid-1990s. The problem is cost. Total premiums for employer plans have risen six to eight times faster than wages, depending on whether individual or family coverage is picked, the study found. ...About 20.7 million workers were uninsured in the mid-1990s. A decade later, it was 26.9 million, an increase of about 6 million, the study found.
In the 1990s, there were eight states with 20 percent or more of the working age population uninsured. Now there are 14.
The article notes that workers ultimately fund the health insurance of the elderly, the young, and all of those who receive subsidized healthcare, and it doesn't take extensive consideration to understand that increasing costs make it less likely that employers will offer the benefit and increasing coshares lead fewer employees to accept it. The more the system removes natural incentives to conserve and price shop for select groups, the higher the price will go for the rest.
A fiat that mandates the removal of risks and benefit-cost-cutting will skew the system further. The excesses and waste will come out somewhere — probably in rationed services and reduced quality.
March 21, 2009
Tying Workers to Their Employers
The other day, a coworker and I had a discussion — while we worked, of course — about the many ways the law seems intended to lash us to our employers, in turn providing them with a measure of protection from competition. If they go out on their own, carpenters in Rhode Island must register with the state, which requires an application and fee as well as proof of liability coverage. Also on the form is a requirement of proof of continuing education, although that requirement is currently waived pending somebody's figuring out what carpenters could possibly need to know that they don't learn on the job.
Then there's the tax side. The self employed must pay income tax and self-employment tax, for which (as I understand) they are required to make quarterly estimated payments, all of which begins to make the hiring of an accountant an advisable option.
Then there's hiring employees. With a single hire, the new business must adjust for thousands of dollars in insurance and various payments, which leads many small players in the construction industry to hire employees as subcontractors.
And then there's health insurance, with which Congress looks likely to cinch employees a bit tighter:
Three powerful House committee chairmen have agreed to work together on legislation to overhaul the health care system, starting with the view that most employers should help finance coverage and that the government should offer a public health insurance plan as an alternative to private insurance. ...Many issues, including the question of how to pay for it, are unresolved. But the House chairmen said they had informally agreed to plow ahead on the assumptions that individuals would be required to carry insurance and that most employers would be required to help pay for it.
Of course, that required "healthcare assistance" will come right out of employees pay, yet it will create that much less incentive for employees to take educated risks to break out on their own, and providing it will create one more barrier to growth for the striving entrepreneur. All of which will increase employers' power over their employees, while increasing the financial benefit to most employees not at all.
Furthermore, as regulations seek to provide workers protection, they create incentive for employers to behave in ways that would leverage loopholes. With Rhode Island's unemployment insurance system, employers have reason to motivate employees to quit (or to trick them into doing so, as I have seen done).
Eventually, we can hope, Americans will figure out — and elect representatives who appreciate — that freedom and opportunity are the best protections against abuse, poverty, and healthcarelessness.
March 12, 2009
Corderre Opens the Socialist Umbrella Wide on Healthcare
In a healthy political state, a legislator would be scared for her political life to propose such policies in a high tax state during a painful downturn:
Legislation introduced by Representative Coderre, (2009-H5519), would extend the reach of the RIte Track program, and establish a new "All Kids Health Insurance Program" to provide access to health insurance for an additional 1,000 to 2,000 or more children in the state.The bill, which is before the House Committee on Finance, would extend RIte Care eligibility to children from families earning 300 percent of the federal poverty level, an increase from the current 250 percent. There are approximately 1,900 uninsured children in this income bracket, and the legislation would enable these children to enroll in RIte Care for an annual monthly premium of $135.
The bill also implements a buy-in program for children living in families with incomes over 300 percent FPL. Families taking advantage of the buy-in option would pay the full cost of the premium (which would include administrative and medical costs), to be determined by the Department of Human Services. It is estimated that 4,900 children in Rhode Island live in families with incomes above 300 percent FPL who don't have health insurance.
The legislation also reinstates coverage for immigrant children under age 10 who are lawful permanent residents in Rhode Island, restoring eligibility for about 1,100 legal permanent resident children who lost coverage during under last year's state budget, and including an anticipated 200 children per year in the future.
Three times the poverty level would be $52,800 for a family of three, $63,600 for a family of four, and $74,400 for a family of five. I've got the personal perspective that this legislation would bring my family within the coverage umbrella, and I'll admit that the only reason I'm struggling is a burden of debt, and my preferred solution to solving that problem would be to increase the opportunities for advancement available to my wife and me. Growing government would do the opposite, as the government seeks somebody to pay the expanding bill.
If we really want universal healthcare coverage, the solution is to decouple insurance from employment, chip away at the growing body of mandates and regulations, and make base-line coverage mandatory. Solutions like Coderre's will push us all closer to the pit.
March 9, 2009
Ken Block: A Painful Lesson in Rhode Island Health Insurance
My dermatologist dumped me this past Monday.
I was fairly new to her practice. Due to too many sunburns as a youngster, I need to see a dermatologist every three months. My previous dermatologist of many years had left the state, leaving me scrambling to find a doc who could take me right away. Many dermatologists don't take new patients or make you wait a year for your first appointment.
My dermatologist dumped me because my health insurance carrier changed from Blue Cross/Blue Shield of RI (BCBSRI) to United Health Care (UHC). On the day of my appointment, the receptionist took one look at my sparkling new health card and snarkily informed me that her office does not accept UHC coverage.
The fact that a doctor's office accepts insurance coverage from one carrier and not another is understandable. It is a bit bewildering that a doctor's office would not accept coverage from one of the largest insurance carriers in the United States — one of only three operating in the state.
As an employer, I was forced to change from BCBSRI to UHC due to cost; my annual renewal premium jumped almost 25% with BCBSRI. I asked for quotes from three carriers for my eight employees. Tufts is newly returned to the market after an absence of many years and came in 5% higher than BCBSRI, which in turn came in 5% higher than UHC.
How is it possible that a state-chartered non-profit like BCBSRI comes in higher for annual premiums than a for-profit carrier? You have to figure that the for-profit outfit is looking for 20% margins or so, which should translate into a significant rate advantage for the non-profit, and therefore a far less expensive cost for the purchaser of the insurance. Is the brand new skyscraper being constructed in downtown Providence for BCBSRI being financed by what I can only call over-charging for their services?
A large chunk of this year's premium increase was courtesy of our General Assembly, which decided to abolish the "healthy company" discount given to companies that used their health insurance less frequently than "less healthy" companies.
Isn't the whole point of insurance to price a policy based on the likelihood of that policy being used or not? Now, the pricing for all small businesses in RI, regardless of carrier, is determined based on the entire pool of covered employees of small businesses. Call this semi-socialized health insurance — whose net effect was a monster price hike for my company's coverage.
The General Assembly has passed mountains of health insurance regulations, many of which directly interfere with an insurance company's ability to operate profitably in the state. This is one of the main reasons that Rhode Island has such a lack of competition among carriers. This lack of competition leads to uncompetitive pricing and heavy-handed doctor tactics like refusing the insurance coverage of a large percentage of the population.
Our system of health coverage in this state is extraordinarily broken and is yet another disincentive for companies investigating moving to our state. The beaches aren't the only place to be burned in Rhode Island.
Ken Block is the chairman of the Moderate Party of RI
March 6, 2009
The latest example of Obama's disdain for liberty
On Obama:
More on Obama's support for socialized medicine.
The Healthcare Trojan Horse in the Porkulus Bill.
On healthcare policy issues:
How government created the problem in the first place.
More on drug costs and government allocation of healthcare services.
So drug costs - the frequent target - are roughly 10-12% of total healthcare costs. The socialists want to reduce their costs when they are only a small portion of the total cost of delivering healthcare services. Not only is that an action which will stifle new drug innovation, thereby adversely impacting the health of future generations, but the lesser/non-use of drugs will often result in more and longer hospitalizations when the symptoms managed by drugs are under less clinical control.
Hey, Obama's historically ignorant and, at a minimum, economically illiterate. So why not add foolish about healthcare services to the growing list?
Get that man a Tele-prompter quickly so he will know what to say!
February 13, 2009
The Public/Private Disconnect
What takes up 10% of my weekly paycheck? Family health care, that's what. And that's just my share. My employer kicks in some, too.
Like so many other employees of small businesses, my company had to health-plan shop again this year to find a way of keeping costs down. In our case, the health care costs went up, just not as much as they would have if we hadn't switched plans. So now, like so many others, I take home a little less than I used to. That's just the way it is.
I'm not alone. You see, in the private sector, yearly reassessment of benefits is the norm. There's no locking in with contracts, no long term "promises." Be flexible or be out of business. Right now, tens of thousands of Rhode Islanders who work in the private sector are taking the hits, sucking it up and living with a little less. In many cases, it is necessary that employees recognize that they can either make a little sacrifice or say goodbye to their job or that of some of their co-workers and friends. I know of a few cases where people have taken pay cuts to stay employed. Or companies that have instituted mandatory furloughs to keep their doors open and avoid further layoffs. Imagine that? That's the simple reality in today's economy.
This is why the compassion meter is just about pegged at "0" when we hear public employees complaining about deals "made in good faith" being broken because they may have to endure reductions in their generous benefit packages or increases in their relatively minuscule co-pays and co-shares. There is no money. And politicians, wisely, are reticent to go to taxpayers asking for more. Everyone else is making sacrifices, now it's their turn.
Small-business owners and their employees are used to cinching their belts and spreading the hardship amongst themselves. That way, hopefully, we can help keep more people employed. Making a little less is better than none at all. The question we keep asking is, how come the public sector isn't willing to do the same for their "brothers and sisters" or the communities they serve?
February 10, 2009
The Healthcare Trojan Horse in the Porkulus Bill
Betsy McCaughey writes:
...Tragically, no one from either party is objecting to the health provisions slipped in without discussion. These provisions reflect the handiwork of Tom Daschle, until recently the nominee to head the Health and Human Services Department.Senators should read these provisions and vote against them because they are dangerous to your health. (Page numbers refer to H.R. 1 EH, pdf version).
The bill’s health rules will affect “every individual in the United States” (445, 454, 479). Your medical treatments will be tracked electronically by a federal system. Having electronic medical records at your fingertips, easily transferred to a hospital, is beneficial. It will help avoid duplicate tests and errors.
But the bill goes further. One new bureaucracy, the National Coordinator of Health Information Technology, will monitor treatments to make sure your doctor is doing what the federal government deems appropriate and cost effective. The goal is to reduce costs and “guide” your doctor’s decisions (442, 446). These provisions in the stimulus bill are virtually identical to what Daschle prescribed in his 2008 book, “Critical: What We Can Do About the Health-Care Crisis.” According to Daschle, doctors have to give up autonomy and “learn to operate less like solo practitioners.”
Keeping doctors informed of the newest medical findings is important, but enforcing uniformity goes too far.
New Penalties
Hospitals and doctors that are not “meaningful users” of the new system will face penalties. “Meaningful user” isn’t defined in the bill. That will be left to the HHS secretary, who will be empowered to impose “more stringent measures of meaningful use over time” (511, 518, 540-541)
What penalties will deter your doctor from going beyond the electronically delivered protocols when your condition is atypical or you need an experimental treatment? The vagueness is intentional. In his book, Daschle proposed an appointed body with vast powers to make the “tough” decisions elected politicians won’t make.
The stimulus bill does that, and calls it the Federal Coordinating Council for Comparative Effectiveness Research (190-192). The goal, Daschle’s book explained, is to slow the development and use of new medications and technologies because they are driving up costs. He praises Europeans for being more willing to accept “hopeless diagnoses” and “forgo experimental treatments,” and he chastises Americans for expecting too much from the health-care system.
Elderly Hardest Hit
Daschle says health-care reform “will not be pain free.” Seniors should be more accepting of the conditions that come with age instead of treating them. That means the elderly will bear the brunt.
Medicare now pays for treatments deemed safe and effective. The stimulus bill would change that and apply a cost- effectiveness standard set by the Federal Council (464).
The Federal Council is modeled after a U.K. board discussed in Daschle’s book. This board approves or rejects treatments using a formula that divides the cost of the treatment by the number of years the patient is likely to benefit. Treatments for younger patients are more often approved than treatments for diseases that affect the elderly, such as osteoporosis.
In 2006, a U.K. health board decreed that elderly patients with macular degeneration had to wait until they went blind in one eye before they could get a costly new drug to save the other eye. It took almost three years of public protests before the board reversed its decision.
Hidden Provisions
If the Obama administration’s economic stimulus bill passes the Senate in its current form, seniors in the U.S. will face similar rationing. Defenders of the system say that individuals benefit in younger years and sacrifice later.
The stimulus bill will affect every part of health care, from medical and nursing education, to how patients are treated and how much hospitals get paid. The bill allocates more funding for this bureaucracy than for the Army, Navy, Marines, and Air Force combined (90-92, 174-177, 181).
Hiding health legislation in a stimulus bill is intentional. Daschle supported the Clinton administration’s health-care overhaul in 1994, and attributed its failure to debate and delay. A year ago, Daschle wrote that the next president should act quickly before critics mount an opposition. “If that means attaching a health-care plan to the federal budget, so be it,” he said. “The issue is too important to be stalled by Senate protocol.”
More Scrutiny Needed
On Friday, President Obama called it “inexcusable and irresponsible” for senators to delay passing the stimulus bill. In truth, this bill needs more scrutiny.
The health-care industry is the largest employer in the U.S. It produces almost 17 percent of the nation’s gross domestic product. Yet the bill treats health care the way European governments do: as a cost problem instead of a growth industry. Imagine limiting growth and innovation in the electronics or auto industry during this downturn. This stimulus is dangerous to your health and the economy.
The actual article has all the links.
Welcome to the beginnings of socialistic medicine in the United States. Brought to you by your favorite community organizer. It's not like he didn't tell us his intentions in advance.
Think about it: If you oppose the porkulus, Obama says you are a partisan. And if you don't cave to these terms asap, Obama says it will turn into a catastrophe.
Isn't hope and change simply wonderful?
January 23, 2009
A Taste of the Healthcare Future
Quite apart from the question of whether Governor Carcieri's Medicaid waver plan is the right move for Rhode Island at this time, it certainly provides evidence of the future of government-funded healthcare:
To save $200,000 in the 5 1/2 months remaining in this budget year, the Department of Human Services intends to seek bids to determine where a patient can go for the cheapest non-emergency surgery, a tonsillectomy being just one example cited by DHS Director Gary Alexander yesterday. A hospital? A surgical center? A doctor’s office?The "selective contracting" of surgical services was just one of several money-saving plans that came to light yesterday after a second day of hearings on legislation to require General Assembly approval before the administration can use its new powers to limit, redesign or raise the patient share of the cost for any medical service covered by Medicaid.
Governor Carcieri is banking on at least $2 million in Medicaid savings this year to help avert a massive state deficit, and Alexander acknowledged this is also hinged on "selective contracting" with companies willing to provide the least expensive prescription drugs and medical equipment; a previously disclosed $10,000 liquid-assets maximum for adults to qualify for the state-subsidized RIte Care health-insurance program, and the "diversion" of 196 nursing home patients to alternative settings.
For some, there's no thinking beyond the immediate desire to make healthcare "fair"; they'll turn a blind eye to the water flowing onto the deck as they decry changes to government programs. They're willing both to let the state sink and to shove greater and greater numbers of the population a lifeboat that's already proven to have holes (probably because their whining can have some effect on a handful of politicians, whereas the market does what it does).
January 21, 2009
Just So Will Healthcare Fall
It amazes me that we can watch these things, which should have been entirely foreseeable, and never return to our initial premises:
Some of the big-name Boston teaching hospitals that have managed to extract higher insurance payments include Children's Hospital and the members of Partners HealthCare, a group including Massachusetts General and Brigham and Women's. As a result, they may be paid two or three times more than a community hospital for the same procedure. ...In addition to helping raise the average Massachusetts family's premiums by 78 percent since 2000, the 800-pound-gorilla hospitals are using their enhanced profits to expand into the suburbs and take business from smaller hospitals. For example, Partners has built a $43 million outpatient clinic in Foxboro, not far from Caritas Norwood Hospital. The objective is to drain day-surgery patients from Caritas, which because of its lower insurance reimbursements, is $4 million in debt. Caritas asserts that were it paid the same rate for delivering babies as the Partners hospitals, it would have lost no money in the third quarter.
Ensure funding for anything, and prices will go up. Increase the distance between the customer and the payment, and advantaged suppliers and middlemen will leverage their power for even greater dominance. And then comes the predictable reaction:
In response to these revelations, Governor Patrick has proposed having state insurance regulators stop excessive premiums. And he has convened a panel to embark on cost-containment steps in Massachusetts, something that is long overdue.
So now prices will ultimately be determined by a government whose interest is more directly in the payments than the service provided, conducted by a panel whose power is appointed, overseen by politicians whose underlying job is to raise money and be reelected.
What do you suppose will happen next?
January 18, 2009
When Sin Trumps Conscience
Rhode Island is one of seven states that would prefer that citizens with moral reservations about procreation-related procedures and drugs have fewer rights:
Seven states sued the federal government Thursday over a new rule that expands protections for doctors and other health care workers who refuse to participate in abortions and other medical procedures because of religious or moral objections.Connecticut Attorney General Richard Blumenthal filed the lawsuit in federal court in Hartford on behalf of the states.
They claim the federal rule, issued by the Bush administration last month and set to take effect Tuesday, would trump state laws protecting women's access to birth control, reproductive health services and emergency contraception.
Blumenthal said the regulations "are flawed and defective" and would "unconstitutionally and unconscionably interfere with women's health care rights."
Note that the rule does not ban any procedures. It merely gives the individual provider the right to choose what he or she provides.
The end of rights and freedom will come proclaiming the sanctity of both.
January 16, 2009
The Benefit of a Word
It's may be a small thing, but it always bothers me when the word "benefit" is used to describe welfare-type payments and services, as in:
"This is to make the system better," [Governor Carcieri] said yesterday, noting that nursing home residents could more easily use Medicaid funds to live with family or friends under the new plan. But when asked about a separate proposal to limit the "benefit package" for thousands of low-income health-care recipients, Carcieri referred questions to a department head.
The connotation of one's "benefit package" at work seems to me to be that it is an extra benefit of doing something — namely, helping to move the company forward. In the case of insurance (not necessarily of the healthcare kind), one receives "benefits" for having invested in the plan.
If language matters, and I believe that it does, we ought to come up with a new term for receiving public largess, taken under penalty of legal repercussions, based purely on perceived need. Maybe "graft."
December 21, 2008
When Doctors Define Health
Such arguments become deep precipitously, but there remains something disconcerting about the method by which society determines the behaviors that are considered within the bounds of normality and those that justify treatment:
The book is at least three years away from publication, but it is already stirring bitter debates over a new set of possible psychiatric disorders.Is compulsive shopping a mental problem? Do children who continually recoil from sights and sounds suffer from sensory problems — or just need extra attention? Should a fetish be considered a mental disorder, as many now are?
Panels of psychiatrists are hashing out just such questions, and their answers — to be published in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders — will have consequences for insurance reimbursement, research and individuals' psychological identity for years to come.
The process has become such a contentious social and scientific exercise that for the first time the book’s publisher, the American Psychiatric Association, has required its contributors to sign a nondisclosure agreement.
The debate is particularly intense because the manual is both a medical guidebook and a cultural institution. It helps doctors make a diagnosis and provides insurance companies with diagnostic codes without which the insurers will not reimburse patients’ claims for treatment.
The judgment of normality and disorder ultimately falls to the individual and to those who interact with him or her. The difficulty (and political jockeying) increases in proportion to the compulsory assistance of those whom consensus acknowledges as having problems — and compulsory acceptance of those whom "consensus" denies as having problems.
We are called, I believe, to help those who need help and to accept those whose challenges do not bear directly on our specific relationships with them. The current structure for psychological diagnoses, however, seems to be drifting toward ever more infringement on our own ability and right to judge those around us for ourselves.
December 18, 2008
Wagner v. Taylor
Michael Barone of U.S News and World Report has an interesting capsule history of how labor/management relations through the 20th Century have brought the U.S. auto industry to where it is today…
Mickey Kaus, pretty much alone among the commentators I've been reading, indicts "Wagner Act unionism" for the decline and fall of the U.S. auto industry. The problem, he argues, is not just the high level of benefits that the United Auto Workers has secured for its members but the work rules—some 5,000 pages of them—it has imposed on the automakers. As Kaus points out, unionism as established by the Wagner Act is inherently adversarial. The union once certified as bargaining agent has a duty not only to negotiate wages and fringe benefits but also to negotiate work rules and to represent workers in constant disputes about work procedures.It is interesting to note that "Taylorism" was a part of the general trend occurring in the first half of the twentieth century, where the old classically liberal ideas were considered passé and the idea that the common folk needed strong management by an elite, in every area of their lives that mattered held a strong foothold.The plight of the Detroit Three auto companies raises the question of why people ever thought this was a good idea. The answer, I think, is that unionism was seen as the necessary antidote to Taylorism. That's not a familiar term today, but it was when the Wagner Act was passed in 1935. Frederick Winslow Taylor was a Philadelphia businessman who pioneered time and motion studies. As Robert Kanigal sets out in The One Best Way, his biography of Taylor, he believed that there was "one best way" to do every job. Industrial workers, he believed, should be required to do their job in this one best way, over and over again. He believed workers should be treated like dumb animals and should be allowed no initiative whatever, lest they perform with less than perfect efficiency.
We should be trying to move past Taylorist attitudes, the collateral damage they've caused in the past, and a possible revival of them in the near future, in as many places as possible.
December 7, 2008
Healthcare Shouldn't Work This Way
Tied to employment, that is:
As jobless numbers reach levels not seen in 25 years, another crisis is unfolding for millions of people who lost their health insurance along with their jobs, joining the ranks of the uninsured. ...About 10.3 million Americans were unemployed in November, according to the Bureau of Labor Statistics. The number of unemployed has increased by 2.8 million, or 36 percent, since January of this year, and by 4.3 million, or 71 percent, since January 2001.
Most people are covered through the workplace, so when they lose their jobs, they lose their health benefits. On average, for each jobless worker who has lost insurance, at least one child or spouse covered under the same policy has also lost protection, public health experts said.
Most people who are unemployed for a time manage to continue making payments for cars and auto insurance, houses and home-owner's insurance, and so on. There is no reason that employers ought to have the power of life and death over their employees. And there's no reason that we should take that power from them and give it to the government.
December 2, 2008
Why Should Their Moral Rights Be Trampled?
The Bush administration is entirely right to permit healthcare providers to refuse tasks that they find objectionable:
The outgoing Bush administration is planning to announce a broad new "right of conscience" rule permitting medical facilities, doctors, nurses, pharmacists and other healthcare workers to refuse to participate in any procedure they find morally objectionable, including abortion and possibly even artificial insemination and birth control. ...Health and Human Services Department officials said the rule would apply to "any entity" that receives federal funds. It estimated 584,000 entities could be covered, including 4,800 hospitals, 234,000 doctor's offices and 58,000 pharmacies.
If private organizations wish to require particular procedures to be done, that's within their purview, but the government's position should be in line with the rights and freedoms that it guarantees to its citizens.
October 30, 2008
Common Ground: I Don't Want David Cicilline Making Decisions About My Healthcare Either
To the members of the six Providence municipal unions who, in the words of Philip Marcelo of the Projo, “[oppose] the city’s decision to change its health care benefits manager”, let me one more time pitch the most obvious solution to your dilemma…
- Your health insurance should be separated from any direct employer involvement; David Cicilline should have zero say who any individual has as their health insurer.
- The money now going to pay for a city-negotiated healthcare plan would then be distributed to the individual employees, in the form of increased salary. It’s your money anyway.
- Employees could then pool their money together and have their union negotiate directly with the insurer or insurers of their choice, to get the deal they want.
October 21, 2008
Work and Health Should Be Only Indirectly Linked
I'm with Jeff Jacoby:
De-linking medical insurance from employment is the key to reforming healthcare in the United States. McCain proposes to accomplish that by taking the tax deduction away from employers and giving it to employees. With a $5,000 refundable healthcare tax credit, Americans would have a strong inducement to buy their own, more affordable, insurance, rather than relying on their employer's plan. As millions of empowered consumers began focusing on price, price competition would flourish. And as employers' healthcare costs declined, most of the savings would return to employees as higher wages.For 60-plus years, a misguided tax preference for employer-sponsored health insurance has distorted America's healthcare market. The price of that distortion has been paid in higher costs, fewer choices, and mounting anxiety. The solution is to restore market forces by fixing the tax code, and liberating Americans from an employer-based system that has made everything worse.
October 17, 2008
Healthcare Intrigue
Granted, they devoted some time to debate talk, but it says something encouraging that Andrew and Matt Allen actually pushed past the time slot on Wednesday to further discuss healthcare. I, for one, would have liked a whole hour of that conversation. Stream by clicking here, or download it.
October 15, 2008
Emulating Fannie Mae in the Health Insurance Industry; Yes We Can!
Democratic Presidential nominee Barack Obama’s health plan has the Federal government getting directly into the health insurance business. He wants the government to create "a new public plan" for health insurance that would compete with existing private insurers. Senator Obama also wants the administrators of this new plan, or some other government-created insurer, to assume nationwide responsibility for catastrophic health insurance -- creating a government monopoly over one segment of America's healthcare economy.
If the idea of a targeted, government-backed monopoly sounds vaguely familiar, it's because another government created monopoly, the Federal National Mortgage Association (Fannie Mae, for short) has been in the news lately, and not in a good way. Fannie Mae was the "government sponsored enterprise" that held a virtual monopoly in the secondary mortgage industry whose mismanagement and collapse helped trigger the current worldwide financial crisis.
Fannie Mae collapsed because it was allowed to take risks that regulators would have quashed had they been attempted by a company identical in every way to Fannie Mae, save for the government backing. As blogger Mickey Kaus has noted, the unsound financial practices were accepted because of Fannie Mae’s aggressive advocacy of its social agenda -- increasing the rate of homeownership -- when challenged and because Congress and executive branch regulators responded to Fannie Mae's lobbying with a collective cognitive non-sequitur: because the organization’s intentions were good, no one needed to pay serious attention to its financial situation. Enmeshed in a culture that denied the need for oversight, warning signs were missed and Fannie Mae’s problems built up until a multi-hundred billion dollar bailout (separate from the much publicized $700B bailout of private institutions) became necessary to keep it and the mortgage industry which it dominated functioning.
Here’s the question for the future: why, in the long run, should the public expect the fate of Barack Obama's government created insurer to be any different than that of Fannie Mae? Like Fannie Mae, Barack Obama's new insurance company will be created in pursuit of a social goal (expanding access to health insurance). Like Fannie Mae, the government created insurer will be inextricably tied to the Federal government. And like Fannie Mae, the government created insurer will almost certainly be given regulatory advantages over its private competitors -- which may or may not make fiscal sense -- to help it achieve its social goal.
If you view government entities as organizations created and staffed by the same flawed humans that exist in every other walk of life, the potential danger here is obvious; allowing an organization, in this case, the Federal government, to create and run a national scale monopoly and then expect it to effectively regulate itself is an invitation to more Fannie Mae levels of mischief.
Will government remember this lesson by the time it takes up an Obama healthcare plan? Or is an assumption the government-does-it-better, no need to think this through, all that Democrats need to know when formulating their health plans?
October 13, 2008
On Obama's healthcare policies
From The Corner:
Obama says we shouldn't allow people to shop for insurance across state lines because some states allow health insurers to exploit nefarious loopholes.Doesn't this argue for, not against, letting people in shop across state lines to get more favorable coverage?
In other words, if you are trapped in a state where these dubious entities are duping innocent policy holders, shouldn't you have the freedom to get on the Internet and escape to another plan?
Obama is in effect saying no. We have to be trapped in the tangle of our state's regulatory mess even if there is a better deal just over the fence.
I would ask Obama if he supports generic prescription-drug importation. I suspect the answer is yes, in which case he is saying we can get our drugs from Mexico, but we can't get our health insurance from Michigan. Pills from Canada "yes." Policies from Connecticut "no." Does that make any sense?
More:
The Cabinet of Dr. Obama: Dissecting the health care proposals of Obama and McCain
The Dems’ Health-Care Distortions: Seeing through the Obama smokescreen
Obama’s Glass House: It’s his health-care plan that would push people out of job-based coverage
ADDENDUM
By contrast, McCain in today's Daily Standard:
McCain's remarks on health care in his speech today are worth highlighting: "I will provide every single American family with a $5000 refundable tax credit to help them purchase insurance. Workers who already have health care insurance from their employers will keep it and have more money to cover costs. Workers who don't have health insurance can use it to find a policy anywhere in this country to meet their basic needs."
Few know how ironic it is that post-WWII government actions created the problem in the first place where health insurance was "owned" by your employer instead of the insured person.
Meanwhile, Don Boudreaux shreds E. J. Dionne's equally stupid thinking on healthcare policy.
September 18, 2008
The "Advantage" of Universal Healthcare
In response to my question on the Medicaid waiver being sought by the Carcieri administration, commenter "mrh" responded…
I'd say that in general, "liberal Democratic" plans for universal health care don't promise to "put people on waiting lists for treatment, and limit the duration and scope of services."…to which commenter "bobc" responded…
You're right they don't "promise" to "put people on waiting lists for treatment, and limit the duration and scope of services." But of course they will!Let me further Bobc's point with a few examples…
1. This is from New York Times columnist Paul Krugman, who I believe is considered mainstream (maybe even a centrist!) by most liberals…
A national health care system will also be better at rationing when the time comes, but that hardly seems like the prime argument for adopting such a system today.Krugman is for having government limit access to medical care, as he says, "when the time comes", but doesn't want people to know about this rationale for getting government into the healthcare business until it's too late. Many problems here.
2. A little more locally, Froma Harrop of the Projo recently wrote this about the Massachusetts universal healthcare mandate…
There have been glitches, the main one being that the plan will cost $129 million more than projected. That sounds like a lot of money, but bingo, the state could save $160 million simply by enrolling all its Medicaid members in managed-care plans. Shortfall averted with $30 million left over.If the point of "managed care" in this setting isn't to give government bureaucrats the power to deny treatment, then how exactly does it work to control costs? (And remember, specifically for this example, Froma Harrop doesn't believe that preventative medicine does anything to lower costs, so that can't be the answer).
3. Moving out a bit towards the fringes, William Saletan of Slate Magazine believes the government-run healthcare should be used to reduce age inequality, i.e. the fact that genetics allow some people to live longer lives than others. I don't think this is mainstream thinking, but that doesn't mean that someone who believes as Saletan does couldn't end up in charge of a rationing or managed care system, once one was constructed.
We can always argue how much any subset of liberals is speaking for all liberals, if it's possible to speak for all liberals, etc. However, it is abundantly clear that an intersection does exist of people who 1) vote "Democrat" on a regular basis 2) want government to be more strongly involved in setting an individual's range of healthcare options and 3) want that stronger influence to be there to control costs by denying care.
If this is truly fringe thinking (even beyond Saletan), the wider world of liberalism should be more vocal about it.
September 15, 2008
The Times and the Medicaid Waiver
The New York Times editorial board says the Carcieri administration's plan to redesign Rhode Island's Medicaid program is risky…
Under the proposed waiver, the federal government would contribute a fixed annual amount for the next five years (roughly what it was projected to spend anyway), but Rhode Island would limit its contribution to 23 percent of its general revenue budget….My question is, perhaps with the exception of the higher co-payments, how are the actions cited in the Times editorial substantively different from standard liberal Democratic plans for implementing universal healthcare?The state is hoping to make up the difference, without harming patients, by providing health care more cheaply. It wants to require most long-term care patients to get treatment at home or from community-based services rather than in expensive nursing homes and would put virtually all beneficiaries in managed care.
If that isn’t enough, it wants flexibility to charge higher co-payments, put people on waiting lists for treatment, and limit the duration and scope of services.
September 5, 2008
There Is a Right Path
Just a pause to affirm that one doesn't have to push the boundaries of ethics to extend the boundaries of medical science:
The cell identity switch turned ordinary pancreas cells into the rarer type that churns out insulin, essential for preventing diabetes. But its implications go beyond diabetes to a host of possibilities, scientists said.It's the second advance in about a year that suggests that doctors might be able to use a patient's own cells to treat disease or injury without turning to stem cells taken from embryos.
Of course, some folks give the impression that, deep down, they believe that ethical absolutes are the greatest disease facing humanity, with all mere ailments as subsequent considerations.
August 29, 2008
Obama's Healthcare Detailing
Supposedly, this was "detail" offered by Barack Obama, in his nomination acceptance speech, on his plans for reforming healthcare…
Now is the time to finally keep the promise of affordable, accessible health care for every single American. If you have health care, my plan will lower your premiums. If you don't, you'll be able to get the same kind of coverage that members of Congress give themselves. And as someone who watched my mother argue with insurance companies while she lay in bed dying of cancer, I will make certain those companies stop discriminating against those who are sick and need care the most.So an Obama administration is going to lower premiums for people who currently have health insurance without altering the scope of their coverage and create a massive new entitlement program for people who currently don't have insurance -- all without raising taxes on anybody but "big" business and the top 5% of the working population.
Going beyond the speech, Senator Obama claims he can achieve his goals through increased regulation and through something called the "National Health Insurance Exchange"…
The Obama plan will create a National Health Insurance Exchange to help individuals who wish to purchase a private insurance plan. The Exchange will act as a watchdog group and help reform the private insurance market by creating rules and standards for participating insurance plans to ensure fairness and to make individual coverage more affordable and accessible.It's not economically possible for anyone, even Barack Obama, to lower prices and expand access to healthcare through increased regulation, without reducing the range of medicine covered by insurance. And while a "National Health Insurance Exchange" could, in theory, help expand access by allowing people who are self-employed or who work for companies that don't offer health insurance to get the same tax-benefits that people who work for companies with health insurance currently get, it's doubtful that such a program can help lower prices, unless policies sold through the exchange are given regulatory exemptions that non-exchange programs don't get, which is the kind of thing that a government does when it's trying to run non-government endeavors out of business. This is all pretty straightforward economics, unless there's some major detail about what a "National Health Insurance Exchange" would do that I'm missing.
Related: I thought this part of Senator Obama's speech was blatantly dishonest…
How else could [John McCain] offer a health care plan that would actually tax people's benefits, or an education plan that would do nothing to help families pay for college, or a plan that would privatize Social Security and gamble your retirement?John McCain supports a universal tax credit for health insurance, regardless of who your employer is…
While still having the option of employer-based coverage, every family will receive a direct refundable tax credit - effectively cash - of $2,500 for individuals and $5,000 for families to offset the cost of insurance. Families will be able to choose the insurance provider that suits them best and the money would be sent directly to the insurance provider. Those obtaining innovative insurance that costs less than the credit can deposit the remainder in expanded Health Savings Accounts.How exactly is that "taxing benefits"?
August 26, 2008
Evidence of the Problem Is Not Always Proof of One's Solution
I'm sure there are examples on the Right, as well, and taking my own biases into consideration, I wouldn't be confident declaring an imbalance. But it does seem as if the Left has a habit of assuming the soundness of its solutions and seeing any evidence of the initial problem as explicit proof for its assumption. Consider Ian Donnis:
Speaking of Carcieri, our governor has been an energetic supporter of what proponents call medical malpractice reform. Yet those who believe the medical system is plagued by unwarranted lawsuits might want to watch a segment aired last night on 60 Minutes, featuring actor Dennis Quaid.
The interview with Quaid is certainly chilling. In brief, his newborn twins were given adult dosages of a blood thinner, resulting in a thousandfold overdose that nearly killed them. The reason was that, at three steps between the receipt and administration of the drug, nobody read the label on the vials carefully enough, and the different shades of blue on the two versions' packaging were not sufficient to raise alarms.
A few details worth noting: According to 60 Minutes, there have been two similar incidents over a span of several years, one before and one after Quaid's experience. After the first, the pharmaceutical company that manufactures the drugs "issued a nationwide safety alert" and modified the packaging. Curiously, Quaid is suing the drug company (for failure to recall), but not the hospital, because:
"I'd like to see Cedar Sinai take the lead in doing something to change what's going on in what I consider to, in the end, a broken healthcare system in patient medical care."
All of which leads one back to Donnis's curious insertion of our governor into the story, which requires him to ignore the fact that the agent for dramatic change in the 60 Minutes report wasn't litigation, but the involvement of a wealthy and famous man. Moreover, of the five components of Carcieri's favored tort reform that Ian cites, only one — limits on non-economic damages and reimbursable attorneys' fees — would have any implications whatsoever for legitimate complaints in the service of rapid change. To insist on the necessity of eye-popping awards from lawsuits, one must imagine that some millions of dollars would add substantial motivation on top of the possibility of killing children to avoid the decisions and mistakes that ushered the wrong drug into Quaid's newborns. One must imagine, in other words, that the packaging designers, pharmacy technicians, nurses, and managers along the line understood, on some level, the possibility of being responsible for deaths and shattered lives and still took less care than they would have in the face of financial liability.
Keep in mind, too, that the financial liability is mostly borne by others: insurance companies, proximately, and policy holders and their clients, ultimately. Therein lies the cognitive dissonance of Donnis's juxtaposition. Malpractice insurance is driving up costs and driving out doctors, and as fewer medical providers are available — working in an environment of ever-tighter margins — mistakes will likely become more common, not less.
Then, true to form, the Left will up its rhetoric in the push for government healthcare... without questioning government workers' capacity for mistakes or government leaders' tolerance for high-profile, high-price-tag litigation, let alone taxpayers' ability to absorb new costs that come with the backing of police power.
August 21, 2008
Just Because It's the Rational Solution Doesn't Mean I'm Going to Stop Talking About It
AFSCME Council 94's President, as reported by Katherine Gregg in the Projo, has named his union's immediate goal in the wake of Judge Patricia's Hurst's decision allowing the Governor's imposition of contract terms to go forward, as least as far as executive branch employees are concerned…
Our number-one goal is to stop the administration from taking money out of the paychecks of the people we represent without negotiations,” Council 94 president J. Michael Downey said.Just keep in mind, if healthcare were decoupled from employment, the administration wouldn't be able to take money out of anyone's paycheck without "negotiation" to pay for insurance or most anything else, just like they can't take money out to make house payments or rent payments or car payments on your behalf.
July 30, 2008
How RI's State Employee Unions And Everyone Else Would Be Helped By a More Rational Healthcare System
If there are any union folks still reading this site, let me use the Council 94 situation as the basis for explaining to you how conservatives would like to reform healthcare. Non-union folks might be interested in this too!
1. Instead of negotiating a plan and spending money with a health insurer, your employer would take the thousands of dollars currently spent per employee on health insurance, and give that money directly to the employees. In operational terms, every employee gets a multi-thousand dollar bump in their paycheck.
2. The employee can then use that money to buy an insurance plan directly from an insurance company. The laws would be changed so that people would be free to purchase insurance plans from any insurer in any state, and so that other government-created factors that artificially increase the price of non-employer health insurance would be removed.
2A. Most importantly, the tax-code would be changed so that individuals who purchase health insurance would get the same tax-break that companies who purchase health insurance for their employees currently get. Right now, businesses that buy health insurance for their employees are allowed to deduct that money from their corporate income tax calculations, but individuals who spend money directly from their paychecks on the exact same plans are not allowed to deduct from their personal income taxes.
(I'm not sure how the current employer tax-break works in the case where the state is the employer, but that only helps make my point: In the reformed system, the self-employed, the corporate-employed, and the state-employed will all be treated the same, which makes sense, as people's health needs don't fundamentally vary based on who their employer is.)
3. Finally, in this new system, a union like AFSCME could still use its negotiating prowess to go out and secure a preferred deal from a health insurance company for its members. AFSCME would bargain directly with the health insurers, choosing whatever health insurer in the country offered them the best deal, and not having to rely on the Governor to negotiate the details of its deal.
The night that Council 94 rejected the current contract offer, WJAR-TV (NBC 10) reporter Bill Rappleye interviewed state employee Sharon Moreno, who expressed a reasonable position about what she would like from the new contract...
Leave me where I am right now [in salary, but] don't touch my coverage.The strength of the plan outlined above is not only that the state wouldn't have to touch health-coverage benefits during contract negotiations, but that the state would not be able to touch health-coverage benefits during negotiations. Unions and employees would talk salary with their employers, and talk health coverage with their health insurers.
I know it's too late for this kind of plan to help with the current situation, but this is the system that makes the most economic sense, the most political sense, and that gives workers the most direct control over their futures. This is the kind of system we need to be looking at moving towards for everyone.
How RI's State Employee Unions And Everyone Else Would Be Helped By a More Rational Healthcare System
If there are any union folks still reading this site, let me use the Council 94 situation as the basis for explaining to you how conservatives would like to reform healthcare. Non-union folks might be interested in this too!
1. Instead of negotiating a plan and spending money with a health insurer, your employer would take the thousands of dollars currently spent per employee on health insurance, and give that money directly to the employees. In operational terms, every employee gets a multi-thousand dollar bump in their paycheck.
2. The employee can then use that money to buy an insurance plan directly from an insurance company. The laws would be changed so that people would be free to purchase insurance plans from any insurer in any state, and so that other government-created factors that artificially increase the price of non-employer health insurance would be removed.
2A. Most importantly, the tax-code would be changed so that individuals who purchase health insurance would get the same tax-break that companies who purchase health insurance for their employees currently get. Right now, businesses that buy health insurance for their employees are allowed to deduct that money from their corporate income tax calculations, but individuals who spend money directly from their paychecks on the exact same plans are not allowed to deduct from their personal income taxes.
(I'm not sure how the current employer tax-break works in the case where the state is the employer, but that only helps make my point: In the reformed system, the self-employed, the corporate-employed, and the state-employed will all be treated the same, which makes sense, as people's health needs don't fundamentally vary based on who their employer is.)
3. Finally, in this new system, a union like AFSCME could still use its negotiating prowess to go out and secure a preferred deal from a health insurance company for its members. AFSCME would bargain directly with the health insurers, choosing whatever health insurer in the country offered them the best deal, and not having to rely on the Governor to negotiate the details of its deal.
The night that Council 94 rejected the current contract offer, WJAR-TV (NBC 10) reporter Bill Rappleye interviewed state employee Sharon Moreno, who expressed a reasonable position about what she would like from the new contract...
Leave me where I am right now [in salary, but] don't touch my coverage.The strength of the plan outlined above is not only that the state wouldn't have to touch health-coverage benefits during contract negotiations, but that the state would not be able to touch health-coverage benefits during negotiations. Unions and employees would talk salary with their employers, and talk health coverage with their health insurers.
I know it's too late for this kind of plan to help with the current situation, but this is the system that makes the most economic sense, the most political sense, and that gives workers the most direct control over their futures. This is the kind of system we need to be looking at moving towards for everyone.
July 24, 2008
Using Government-Run Healthcare to End Age Inequality
William Saletan of Slate Magazine's Human Nature Blog says one of the purposes of government run health care system should be to reduce age inequality. And he's not just talking about making people with shorter lives live longer (h/t Mona Charen)…
Isn't health, like wealth, an unequally distributed asset? Isn't it, in fact, the ultimate asset? And if that's the case, should we means-test people on Medicare not just for wealth, but for age?Remember, if you ever get stuck in a Medicare-for-all or other fully socialized type of healthcare system, the people who have ultimate control over your healthcare access could end up being people like William Saletan, who believe that it is a function of government to decide how much life is too much.Actually, means testing is the wrong term. Age isn't really a means; it's more like an end. So let's call it an ends test. The theory is that just as some people have enough money, others have had enough time.
If you make it to 100 and can fund your own surgery, that's terrific. But Medicare should focus its resources on people who haven't been as lucky as you. Living to 99 is no tragedy. It's a blessing.
One of the reasons I chose healthcare as the topic for Anchor Rising's most recent appearance on the Matt Allen Show is that regular people need to start thinking about these kinds of arguments right now, as there is a very high probability that the next President of the United States is going to put some kind of major healthcare before Congress, and people need to be aware of how much "if there are fewer people living shorter lives, the people who are left will be better off"-type thinking is influencing American policy makers -- and whether that thinking needs to be vigorously challenged.
Finally, it is my sincere hope that Saletan's item makes a few people on the left ponder, even if just for a few moments, whether it is a good idea to always uncritically accept "ending inequality" as a legitimate goal for government policy.
Healthcare on the Radio
Andrew brought the healthcare conversation to the Matt Allen Show, last night; stream the discussion by clicking here or download it.
July 23, 2008
Confront Healthcare Inflation or Die: A Broad View of Healthcare Reform
This past Sunday, the Projo ran a contrarian Froma Harrop column, where she questioned the conventional healthcare reform wisdom that a focus on preventative care will lower costs in the long run…
The word “prevention” has a nice ring in any health-care discussion. Thus, many politicians argue that programs to stop smoking, improve diets and otherwise promote wholesome living save money in the long run. A healthier population at less cost. Sounds like a win-win situation.There is fodder for many important discussions here, but for now, I want to focus on just one aspect -- the costs of those extra CT scans.Unfortunately, that formulation is a pleasant fantasy…
Let’s put it bluntly: Longer lives cost money. Those who make it to 90 thanks to exercise and six daily servings of vegetables are more likely to suffer the expensive ravages of old age. Everyone dies of something. So he who avoids a fatal heart attack at 70 is more at risk of cancer at 80. Those extra 10 years can mean extra CT scans, hip replacements and physical therapy, even for those in relative good health.
Later in her op-ed, Harrop makes reference to the exorbitant rate of medical inflation…
Rapidly rising prices for health-care also add to the expense of moving big-ticket medical procedures into later years, explains [Arthur Garson Jr., provost at the University of Virginia Medical School]. “In today’s world, where the rate of medical-care inflation is twice the rate of regular inflation, anything done 10 years from now is, in real dollars, 25 percent more expensive.”But why should hyper-inflation in healthcare prices, for decades at a time, be accepted as some unalterable force of nature? As technologies mature, why shouldn't the costs of producing and using medical hardware come down in exactly the same way that hardware costs in other economic sectors do; for example, think of cell phones or printers, which were once expensive luxury items, but are now affordable to nearly everyone. And then consider the CT-scans. A medical facility that has recently purchased CT equipment should be able to charge a lower price to each patient while paying off the costs of the equipment off just as quickly if they can treat 100 more of Froma Harrop's longer-living people per year than they would have if people were dying off more quickly. Why aren't these kinds of effects bringing the rate of healthcare inflation down to reasonable levels?There are two ways to deal with that problem, according to Garson. Get medical costs down, and “keep people as healthy as possible as long as possible so that they don’t spend as much money being sick.”
It is not possible to improve the combination of healthcare quality and access in the U.S. without grappling with the economic irrationality of continuing, runaway medical inflation. If policy makers involved in healthcare reform ignore the inflation question, declaring it to be some kind of iron law of modern society, the "best" they are going to be able to come up with is -- by definition -- a permanent regimen of forcing people to pay more for less, aka a program of rationing.
Of course, to do the right and effective thing, healthcare policy makers are going to have to confront the problems that have been created by poorly thought out government interference with individual medical choices. Health and Human Services Secretary Michael Leavitt wrote about a particularly egregious example earlier this month in the Wall Street Journal…
For years, the Government Accountability Office and the Department of Health and Human Services' inspector general have been saying Medicare is paying too much for Durable Medical Equipment (DME). Just compare what Medicare pays to the prices of equipment for sale on the Internet.Do you think this is the only case where the cost of medical hardware has been grossly inflated by strange government priorities, or just the worst?DME prices are based on a fee-schedule established by law in the 1980s and subsequently updated for inflation. But the fee-schedules weren't based on competitively determined market prices. It is a price-fixing program, and the equipment suppliers like it because they get overpaid and don't have to compete.
An oxygen concentrator, for example, is a device that delivers oxygen through a tube to patients, and it costs about $600 on the open market. Medicare beneficiaries typically rent the machines. The rental period, set by statute, is up to 36 months. The monthly rental payment, also set by statute, is $198.40. So renting an oxygen concentrator for 36 months costs $7,142.
As with most items and services in Medicare Part B, beneficiaries pay 20% of the costs, and Medicare pays the remaining 80%. The government, therefore, pays $5,714 – almost 10 times the free-market price of purchasing a concentrator outright. The patient pays $1,428 – more than twice the free-market price of purchase. Even allowing for the costs of setting up equipment, training and fitting the beneficiary, and other things, the rental fee is way out of line.
June 23, 2008
What Hospitals Want Isn't Necessarily Good For Everyone Else
I don't find anything persuasive in Charles Kinney and Fred Allardyce's Sunday Projo op-ed arguing in favor of legislation that would make insurance companies responsible for the uncollected debt related to the unmet deductibles and co-payments of their subscribers. Mr. Kinney and Mr. Allardyce begin by immediately linking uncollected debt to preventative care...
Our health-care system is undeniably broken. Insurance premiums are soaring, putting preventive health care out of reach for many. Employers and insurers are shifting costs to others by turning to plans with higher deductibles and co-payments. The result is a physically unhealthy society and a fiscally challenged health-care system overburdened by increasing numbers of people facing health-care crises with no means to pay.But in any rational economic analysis, preventative care is an odd area to single out if you are concerned about "dangers" of consumer driven healthcare. As we've gone through in detail before here at Anchor Rising, it does not make fiscal sense to use an insurance-style system to pay for preventative medicine; it never has and never will. If you are really interested in seeing everyone be able to take advantage of preventative care opportunities, paying for them through the insurance system is an especially bad idea, as insurance programs can only increase costs to consumers when they include services that are widely used.One of the major issues hospitals are facing is the increase in bad debt — patients who do not pay their bills. For patients who do not have the means to pay, we provide free care.
By linking uncollected debt and preventative care, Mr. Kinney and Mr. Allardyce are functioning as standard-issue, risk-averse big-business executives in search of ways to separate individuals from their money as quickly and as predictably as possible. The most efficient way for a hospital to do this is to force people to pre-pay for the services most likely to be used. That's good for organizational financial planning and good for the cash-flow and balance sheet of a hospital, but has nothing to do with controlling health care costs or making healthcare affordable.
What is especially egregious about Mr. Kinney and Mr. Allardyce's argument is that, at the same time they are pursuing a government-created fiscal advantage of dubious (and probably negative) value to the healthcare consumer, they are also advocating for their organizations to be insulated, by law, from the practical financial realities of their business…
If a patient has private insurance, such as United Healthcare or Blue Cross, and he or she doesn’t respond to reasonable collection efforts for co-payments and/or deductibles, we have to write off 100 percent of that loss at the present time. The role of the hospital turns from caregiver to debt collector. This burden should not be placed on the shoulders of non-profit hospitals; debt collection should be the responsibility of the commercial insurance companies.The fundamental flaw in this argument is that hospitals aren't caregivers; nurses and doctors are. Contrary to Mr. Kinney and Mr. Allardyce, it is precisely the primary job of a hospital and its administrative staff to do the mundane, daily things that need to get done so that the primary caregivers have an environment where they can function with maximum effectiveness. The hospital worries about keeping the lights on and the water running and making sure that supplies are delivered to the right places, while the nurses and doctors worry about the caregiving. A hospital administrator who says he shouldn't have to worry about collecting the money to pay the bills makes about as much sense as one who says that he should be given land for free, because hospitals shouldn't have to worry about the details of financing and mortgage payments when deciding how best to expand their facilities to provide improved care.
Healthcare is a people business. If you don't want to deal with people, you should be in a different business.
ADDITIONAL INFORMATION
Roland Benjamin, who knows as much about the relationship between employers and insurance companies as anyone in Rhode Island, offers more detail on why making insurers responsible for uncollected hospital debts is a bad idea, in the form of a letter he sent on this issue to the House Corporations Committee...
Relieving hospitals from the most fundamental of business processes (collecting fees from users) is simply continuing the trend of requiring more from our insurance carriers and the employers that pay them. In effect, House Bill 7057 and Senate Bill 2414 referred to House Corporations on 3/18 will require insurance carriers that currently have no direct financial relationship with individuals to establish one from the ground up. The cost of doing so will present in premiums passed through to employersOf particular note are three concerns:
As a studied buyer of insurance products for more than 100 participants in my plan, I simply do not want to pay for this coverage. I urge that the House Corporations Committee not recommend passage of this bill.
- Assuming the carriers can seamlessly transition to a broad financial arrangement with members, the costs of administering these relationships will be born more heavily by Consumer Directed Plans. While these plans are the subject of contention from the provider side, they represent the most viable means of applying consumer dynamics to the health care economy.
- Should a patient fail to pay a bill from a hospital, the hospital will go after the carrier, who in turn will go after the employer, since they will have a statutory obligation to keep insuring the individual and thus no collection effort leverage. The result, should an employer refuse to make this payment on behalf of an employee (and due to privacy requirements will not know for whom or what they would be paying), the employer's account could be affected, thus leaving the entire employment base without insurance.
- There is no indication that failure to collect payment from privately insured individuals represents a significant burden to hospitals as a percentage of total operating expenses. Thus, a solution attempting to solve this issue, at the expense of a massive administrative restructuring in the industry, will only serve to escalate overall costs.
June 11, 2008
What?
This component of the RI House budget plan is nuts:
he plan also includes funding for 100 of 400 slots slated to be eliminated from the early childhood education program, Head Start. In addition, the budget restores health care coverage for all but 1,000 of more than 7,000 adults slated to lose coverage under a plan released by Governor Carcieri earlier in the year. ...... it generates $5.6 million in new revenue by increasing the health insurer tax on medical premiums from 1.1 percent to 1.4 percent. Costantino said he hoped the increase wouldn't be passed on to health care consumers, although that's what happened when the tax was expanded last year. The tax, previously only applied to health insurers, would now apply to Delta Dental as well.
So the budget will continue to pay for the healthcare of a few thousand adults who can't afford it, but it most definitely increase the price paid by everybody else. It would seem that the state's budget is not constructed with much by way of strategy — instead by picking and choosing various numbers to call the result "balanced."
June 10, 2008
Stacking the Healthcare Deck
The state of Rhode Island likes monopolists, it would seem:
The other condition that Tufts needs to change is a state law that says only health plans that did business in Rhode Island in 2001 can take the health status of members into account in setting rates for small groups. As a result, only Blue Cross and United can increase premiums for groups whose members are less healthy.
Changing that rule ought to be an obvious step.
Readers should note that such regulations — questions of bias in their application aside — are one of the reasons that healthcare costs so much.
June 5, 2008
Toward Universal Healthcare
In a comment to my recent post about being a doctor in Rhode Island, Old Time Lefty asked (among some insults, statements seeped in common spin, and other junk that I'll ignore):
Health insurance should not be joined to employment. It should be a right. If it’s not a right, do you think it’s a worthwhile endeavor to establish program or programs to cover them all? What program to do this are you espousing?
I'm always hesitant to assent to calling something "a right" in the presence of left-wingers, because the definition of what a given right might entail is generally more expansive and fluid than I believe to be appropriate. However, I'll express general agreement with the proposition that access to healthcare is a right, mainly in order to draw attention to my disagreement with the proposition that health insurance is a right.
Plainly put, "healthcare" and "health insurance" shouldn't be considered synonymous in this discussion. There's a reason you don't use your auto insurance card every time you get an oil change, buy new seat covers, and have your car detailed. Insurance ought to be bought against that which is rare and harmful, not that which is habitual and foreseeable.
So, with this distinction made, how would I provide everybody with access to healthcare?
The first step would be to end price-raising regulations and mandates. That would include all laws that push health insurance into the employee agreement. (Ask Andrew about ERISA.) It would also include requirements that insurance cover viagra, sex-change operation, and a whole medicine cabinet of more common procedures and drugs. Make it possible, in short, for the average citizen to purchase his or her own catastrophic coverage, for use in such illnesses and injuries as ought to bring one to the emergency room or the life-saving surgeon.
The second step would be to make that insurance mandatory. Once we've agreed upon a bare minimum of coverage (taking into consideration severity as well as cost to the public of uncovered treatment). The price really shouldn't be that much, considering the rarity of the use, and perhaps those who still cannot afford it could be covered under a government-negotiated plan with a private provider.
The third step would be to create health savings accounts for every American, created upon birth or naturalization. Each citizen (or his or her parents) would select a firm to administer the account, with the government's role being mainly in establishing the account number and other minor start-up requirements. (The administration would be more akin to bank practices, as opposed to investment practices.) Over a person's lifetime, the individual, employers, charities, and so on could put money into the individual's account (tax free), and he or she could use it solely for medical expenses, including doctor visits, medicine, perhaps even plastic surgery and other electives.
At a certain age, the money could be withdrawn to enhance retirement income, and the full remaining dollar amount could be bequeathed to others, placed in their accounts.
This is just a summary, with some debatable points and specifics to be added for a full-throated policy discussion, and there are a variety of costs and benefits (notably an increase in pay when employers are no longer "responsible" for insurance costs) to such a program that would require more time than a lunch half-hour provides.
June 2, 2008
Lack of Freedom a Threat to Health
Periodically, somebody on the Left will throw in some anti-corporate rhetoric and sneer about the "free market." Mark Patinkin's column on the state's difficulty attracting doctors provides yet another example illustrating that one can hardly point to our problems in condemnation of economic freedom:
I began by asking where he’d rank us nationally in fees paid for medical procedures."In many if not most areas," he said, "it's 49th or 50th in the country."
The reasons are complicated, he said — one factor being restrictive laws.
What kind of laws?
He mentioned several typical procedures for which Medicare will pay a doctor around $300, almost below cost, he said. In some states, top doctors can charge an extra few hundred for patients happy to pay for their expertise. Here, as in Massachusetts, the law forbids that.
"In other businesses," he said, "when you get seniority and experience, you raise your prices. I make the exact same fees as the doctor fresh out of residency. The only way I make more money than that doctor is by seeing more patients. I'm not allowed to charge more for procedures."
Here's a stunning bottom line for doctors:
He gave the real example of a 30-something cancer doctor who recently finished his training. His offer in Rhode Island was $125,000 with three weeks vacation and being on call every third night — being available for patient calls or going to the hospital. On the West Coast, The Doctor said, this same candidate was offered $250,000, eight weeks vacation and "call" every 10th night.
Rhode Island's much touted (but selectively described) "quality of life" is surely threatened if our battle against the free market drives away high-end professionals.
May 2, 2008
The McCain Healthcare Plan
Presumptive Republican Presidential Nominee John McCain has sketched out his healthcare reform plan in the (electronic) pages of National Review Online…
I believe the key to real reform is to restore control over our health-care system to the patients themselves. To that end, my reforms are built on the pursuit of three goals: paying only for quality medical care, having insurance choices that are diverse and responsive to individual needs, and restoring our sense of personal responsibility.American families know quality when they see it, so their dollars should be in their hands. When families are informed about medical choices, they are more capable of making their own decisions, less likely to choose the most expensive and often unnecessary options, and are more satisfied with their choices. Health Savings Accounts are tax-preferred accounts used to pay insurance premiums and other health costs. They put the family in charge of what they pay for, and should be expanded and encouraged.
Americans also need new choices beyond those offered in employment-based coverage. They want a reformed system so that wherever you go and wherever you work, your health plan goes with you. And there is a very straightforward way to achieve this.
Under current law, the federal government gives a tax benefit when employers provide health-insurance coverage to American workers and their families. This benefit doesn’t cover the total cost of the health plan, and in reality each worker and family absorbs the rest of the cost in lower wages and diminished benefits. But it provides essential support for insurance coverage. Many workers are perfectly content with this arrangement, and under my reform plan they would be able to keep that coverage. Their employer-provided health plans would be largely untouched and unchanged.
But for every American who wanted it, another option would be available: Every year, they would receive a tax credit directly, with the same cash value of the credits for employees in big companies, in a small business, or self-employed. You simply choose the insurance provider that suits you best. By mail or online, you would then inform the government of your selection. And the money to help pay for your health care would be sent straight to that insurance provider. The health plan you chose would be as good as any that an employer could choose for you. And if a church or professional organization wishes to sponsor insurance for its members, they should be able to do so. The bottom line: Health insurance would be yours and your family’s health-care plan to keep without worrying that it will go away along with your job.
April 4, 2008
The Other Problem with the Roberts Healthcare Plan
There is very little chance that the core of Lieutenant Governor Elizabeth Roberts' healthcare plan, if passed into law, would survive a court challenge. The doomed element, described by Cynthia Needham of the Projo, is the requirement that...
Businesses with more than 10 employees would be expected to purchase insurance for their workers, or face fines.Here's the technical description of the employer mandate from the legislation itself...
28-43-8.7. Health security assessment. -- (a) Each employer, except those employers employ ten (10) or fewer employees, subject to the provisions of this chapter shall be required to pay, in the same manner and at the same times as the director prescribes for the other required by this chapter, in addition to any other contributions required under this chapter, a health security assessment of each employee of eight percent (8%) of the taxable wage as defined in section 28-43-7, in addition to any other payment which that employer is to make under any other provisions of this chapter...The problem is that the Federal courts have consistently struck down state attempts to mandate health insurance by private employers for conflicting with the Employee Retirement Income Security Act of 1974 (ERISA), which makes it illegal for states to regulate employee benefits any more stringently than the Federal government does. Last year, the Fourth Circuit Court of Appeals nullified a Maryland law that would have required employers bigger than a certain size to pay a certain percentage of their payroll towards health benefits. The Fourth Circuit's ruling did not depend on the details of the mandate, who was affected or how much they had to pay. Just the fact that Maryland was trying to require a particular employee benefit was enough to run afoul of Federal law...(b) An employer may deduct from the amount owed for each employee under subsection (a) its average expenses per employee for providing health insurance coverage or other health care benefits for its employees, allowable for the current quarter by the Internal Revenue Service as a deductible business expense;
Because Maryland's Fair Share Health Care Fund Act effectively requires employers in Maryland covered by the Act to restructure their employee health insurance plans, it conflicts with ERISA's goal of permitting uniform nationwide administration of these plans. We conclude therefore that the Maryland Act is preempted by ERISA and accordingly affirm [the lower-court decision to strike it down].Bottom line: because of ERISA, whether you like it or not, states are not allowed under current Federal to mandate any employee health benefits.
The Roberts Paradox
Cynthia Needham reports in today's Projo on the beginning of Lieutenant Governor Elizabeth Roberts' statewide tour to promote her proposed new healthcare mandates…
Lt. Gov. Elizabeth Roberts last night kicked off a statewide tour in South Providence to promote her health-care plan, making the first of 15 stops…With respect to the illegal immigration issue mentioned by Ms. Needham, Lieutenant Governor Roberts has adopted the position that it is out-of-bounds for the state of Rhode Island to verify the citizenship/legal residency status of its new hires, believing it either to be too big a job for the government to handle, or maybe just unreasonable to ask. Yet at the same time, according to her healthcare legislation, Lt. Governor Roberts also believes that state government is ready and able to take on the burden of verifying the health insurance coverage status of every Rhode Islander...Similar to the Massachusetts system, the Roberts plan would require nearly all Rhode Islanders to have health coverage. Businesses with more than 10 employees would be expected to purchase insurance for their workers, or face fines. Individuals making at least $40,840 and families making $82,600 would be asked to purchase their own health care. The plan would also create a HealthHub, a quasi-public agency to help coordinate purchasing and regulate plans…
Roberts made only brief mention of the immigration issue. “This week I’ve been discouraged with how we do things in this state. But I still have confidence we can work together,” she said, segueing back to the evening’s conversation.
44-30-101. Qualified coverage required -- (c) Every person required to file an individual income tax return as a resident of the state of Rhode Island, either separately or jointly with a spouse, shall indicate on the return, in a manner prescribed by the tax administrator, whether such person, as of the last day for the taxable year for which the return is filed:Tell me, which sounds like an easier job to do, verifying the health insurance status of every Rhode Islander every year, or verifying the citizenship status of new state employees, one time, at the time of hire? The contrast emphasizes an obvious reality, that enforcing immigration law is something that certain politicians don't want to do, not something they believe can't be done.
(i) has qualified coverage in force as required under subsection 44-30-101(a) whether covered as an individual or as a named beneficiary of a policy covering multiple individuals; or
(ii) claims an exemption under section 44-30-102.(d) If a person required to obtain and maintain qualified coverage under subsection 44-30-101(a) above who files a tax return in Rhode Island does not indicate on the return that he or she had such coverage in force, or if the person indicates that he or she had such coverage in force but the tax administrator determines, based on the information available to him or her, that such requirement of subsection 44-30-101(a) was not met, then the tax administrator shall compute the tax for the taxable year based on one less personal exemption, as set forth in section 44-30-2.6, than would otherwise be allowed….
44-30-103. Review -- An individual subject to section 44-30-101 who disputes the determination of applicability, as enforced by the department of revenue, may seek a review of this determination through an appeal established by the division of taxation under section 44-30-89; provided, however, that no additional penalties shall be enforced against an individual seeking review until the review is complete and any subsequent appeals have been exhausted.
I suppose that you might reach the conclusion that government doesn't have the time or resources to take the steps to prevent foreign nationals from breaking the law, as Lt. Governor Roberts apparently has, if you subscribe to the idea that the most important function of government is managing as tightly as possible the lives of law-abiding, gainfully employed citizens and residents. Still, it is legitimate to ask the Lt. Governor why she believes that government is competent enough to track the health insurance coverage of 1,000,000 Rhode Island residents on a year-to-year basis, but unable to reasonably determine the citizenship status of new state hires one-time.
Or does she just believe that illegal aliens are entitled to state jobs?
April 3, 2008
What the Numbers Show
Unfortunately, neither Community Catalyst nor RIte Care Works, the author and promoter respectively, seem interested in providing the full details behind a press release from The Clarendon Group that appears to support the conclusion that every dollar of RI government money taken from RIte Care comes with a 12¢ cost in economic activity but save Rhode Island — overall, not just its government — 14¢:
The report from the national non-profit advocacy organization Community Catalyst, broke down where the dollars cut from the RIte Care program would go:
- 52-cents of each dollar stays with the federal government rather than making it to Rhode Island in the form of federal matching funds.
- 35-cents of each dollar is shifted to the private sector in the form of high-cost uncompensated care that’s ultimately left to hospitals, insurers, and premium payers to pay.
- 6-cents of each dollar is lost in reduced state tax revenue that is no longer being collected on the economic activity associated with the lost federal matching funds.
- ONLY 7-CENTS REMAINS AT THE DISPOSAL OF THE STATE AS "SAVINGS."
Clearly, the authors are measuring "the state" more broadly than just its government, because they include the cost "shifted to the private sector," and surely a failure to merit matching funds doesn't shift to the expense column (for the government) in addition to being erased from the revenue column. What's notable about the findings is that money is saved even with this broad analysis.
On the other hand, they don't give the cost of lost economic activity, just the taxes on it, so the proper interpretation is probably that our analysts stirred a bunch of quick calculations in an activist pot until they arrived at a mixture that they thought to be salable.
March 25, 2008
The Behavior Gap
Let me say right up front that access to healthcare must be improved and expanded, although it goes beyond the scope of this post to delve into the different understandings of the whats and hows of that mandate. Even were that goal to be achieved quickly, however, I suspect that the life expectancy gap between rich and poor would continue to increase, because I think the behavioral explanations play a large role and would bleed into matters of access:
While researchers do not agree on an explanation for the widening gap, they have suggested many reasons, including these:¶Doctors can detect and treat many forms of cancer and heart disease because of advances in medical science and technology. People who are affluent and better educated are more likely to take advantage of these discoveries.
¶Smoking has declined more rapidly among people with greater education and income.
¶Lower-income people are more likely to live in unsafe neighborhoods, to engage in risky or unhealthy behavior and to eat unhealthy food.
¶Lower-income people are less likely to have health insurance, so they are less likely to receive checkups, screenings, diagnostic tests, prescription drugs and other types of care.
As you can see, New York Times reporter Robert Pear offers four examples, evenly split between behavior and "the system," but the former can be as numerous as the attributes of life. Here's another, which touches on an area about which I've written copiously (from an article to which I linked yesterday):
Hymowitz points out that all classes of Americans once followed the same life script of marriage before children. When divorce rates started soaring in the 1970s, everyone was fleeing their marriages. But then the classes started diverging. The Economist cites statistics that show among college-educated women married between 1990 and 1994, only 16.5 percent were divorced 10 years later. Among those with a high-school education or less who married in those same years, about 40 percent were divorced after a decade.
Advocates for government-propelled fixes tend to believe that forcing an expansion of access to a service will yield equal gains across groups, but that's certainly not true. Ask yourself: Would a class with a higher percentage of smokers, poor diets, and divorce be more or less likely, on average, to make full use of even completely prepaid medical services?
As I said, our healthcare system is most definitely in trouble, but change must begin with the culture.
March 13, 2008
Speaking of Illegal Immigration...
... and other budget draining policies in Rhode Island, I'd suggest that most of the solutions for this problem are of an indirect nature:
The heads of four Rhode Island hospitals testified yesterday that their medical institutions are teetering on the brink of financial disaster.And they pleaded with key lawmakers to help — or at least not hurt — their hospitals in the 2008-09 state budget being debated before the House Finance Committee.
Governor Carcieri's proposed budget would force hospitals to pay $32.7 million more for their licenses in the coming year, a move his office said is necessary to help close a deficit of at least $348 million. The proposal, along with the rest of the governor's cost-cutting plans, now rest with the General Assembly.
"We need your help. The budget that we're looking for is a life preserver. The one that's out there now is made out of concrete," Charles S. Kinney, president and chief executive officer of Westerly Hospital, told the committee. "The entire budget ... is just going to have a further denigration on the finances of the hospitals, which are precarious."
We will never achieve the right formula for providing affordable healthcare unless we retune our overall policies to decrease the number of people who are a drag on the system and increase the number of people who are not.
March 12, 2008
Healthcare Consumer Question of the Day
Here is a question for the sage and practical-minded readers of Anchor Rising:
Recently, a friend of mine had an appointment with a doctor who has a policy requiring a $40 payment for appointments cancelled on the same day. Said friend arrived on time. Said doctor did not, not seeing the patient until 45 minutes after the scheduled appointment time.
The question is: in a completely fair universe, shouldn't the patient get $40 knocked off of the bill in circumstances like these?
February 28, 2008
Just Stop It!
Why do our legislators have such difficulty seeing the problem with bills like this:
Already successful in securing enactment of legislation to increase the level of hearing aid coverage in health insurance policies, Rep. Robert B. Jacquard (D-Dist. 17, Cranston) has introduced a bill aimed at assisting more hearing-impaired citizens.Under Representative Jacquard’s bill, health insurance providers in Rhode Island would be required to provide coverage for cochlear implant surgery. A cochlear implant is a small electronic device that is used by individuals who are severely hard-of-hearing. Rather than amplifying sounds as a hearing aid does, cochlear implants bypass damaged portions of the ear and stimulate the auditory nerve, which sends a signal to the brain, enabling deaf people to hear speech more clearly. More than 35,000 children and adults in the United States have received a cochlear implant, and the number of surgeries performed grows each year by about 30 percent. ...
Costs for the implantation procedure have a price tag of between $45,000 and $55,000. If there are complications with the surgery or the patient requires extensive rehabilitation, the total costs can amount to over $80,000. Although many health insurance companies cover the surgery in their policies, some are reluctant to pay for the procedure due to the high up-front cost.
From where does Jacquard think the reluctant insurance companies will get the money to pay for these expensive procedures? They'll tack it on to everybody's premiums, and if they can't get away with that, they'll stop providing health insurance in Rhode Island.
Perhaps the point isn't simple enough for members of the General Assembly to comprehend: what we need in healthcare more than anything is competition. We need more providers, and to manage that, we may need to allow for a non-cochlear-inclusive program or two.
February 20, 2008
First, the Stick
Amazingly, even as they stumble into understanding of that which is making it hard to breathe in Rhode Island, they continue to tighten the noose:
In an effort to slow down the steep rise of health insurance costs in Rhode Island, Sen. Joshua Miller has introduced legislation that would prohibit health insurers in the state from increasing subscribers' premiums by more than 10 percent a year."Huge increases in premiums are pushing health insurance out of reach for more Rhode Islanders every year. Even people who have good jobs and decent salaries are struggling to pay their share of it, let alone those who aren't insured through their employers and have to pay the whole cost on their own," said Senator Miller, a Democrat who represents District 28 in Cranston and Warwick. "Of course insurers have to be able to raise their prices to cover costs, but average Rhode Islanders simply can't afford the size of some of the increases that have been proposed. There has to be a limit on them." ...
He says those experiences have made him aware of the pressures on the insurance industry, and also of the possible solutions that are available to make rates more reasonable.
"We've been examining both sides of this issue, and there are many underlying components that contribute to increased costs for health insurers. There are a wide range of solutions available, but until consensus has been reached within the industry about implementing them, the state should step in with some limits. In fact, these limits may accelerate the implementation of those reforms," said Senator Miller.
So, the legislator understands that there are "solutions" that we ought to pursue, but in the meantime, he's just gonna go ahead and continue with the approach that has had such wonderful results in Rhode Island thus far. Do these people think that if they mix a bit of "I know we shouldn't be so demanding" into their rhetoric, then folks will cease to be concerned about the increasing demands?
(Let whining about "right-wingers on the side of corporations" begin.)
February 15, 2008
Cross-Purpose Reform
Lt. Governor Elizabeth Roberts's healthcare proposal (PDF) strikes me as a hodgepodge with components at odds with each other. There doesn't appear to be a guiding principle, creating the risk that the good points of the program would put a reform-like light on the bad parts, potentially without even passing themselves.
New representative Frank Ferri (D, Warwick) today put forward a bill advancing one of the better suggestions:
The legislation (2008-H 7493) — which Representative Ferri is submitting in conjunction with Lt. Gov. Elizabeth H. Roberts as part of her "Healthy Rhode Island" health reform act — would allow health insurers licensed in Massachusetts and Connecticut to offer insurance products in Rhode Island without having to get any additional licenses.This reciprocal licensing would make Rhode Island a more inviting market to insurers, and could increase the number of insurers in the state. Currently, Blue Cross & Blue Shield of Rhode Island and United HealthCare of New England are the only insurers licensed in Rhode Island.
But other parts of Healthy RI increase state government involvement, fine employers that don't provide health insurance coverage $1,000 per employee per year. and layer on mandates, such as the requirement that all dependent "children" up to age 25 may be covered under their parents' policies whether they're in school or not. Representative (D, Providence) Edith Ajello's mandate appears to be additional:
A state mandate already requires insurers to cover fertility treatment for women between the ages of 25 and 42 who are otherwise healthy but are unable to achieve or sustain pregnancy for a period of a year or more. But under current law, the mandate applies only to married women.Arguing that that the stipulation is discriminatory and would not be permissible in other areas of state law, Representative Ajello has submitted legislation (2008-H 7239) to eliminate the word "married" from the mandate and extend coverage to all 25- to 42-year-old women, regardless of their marital status.
So the state is seeking to attract insurers to Rhode Island, and it may force employees to finance the policies, and it's going to require everybody over four times poverty to have a plan, while layering on regulations that will drive the price up — all under the increasingly pervasive watch of the nation's most corrupt and (arguably) incompetent government. Shouldn't health-conscious politicians be attempting to lower citizens' stress levels?
February 1, 2008
Well, Maybe if the Doctor's Office Was in the Mall....
I gotta say, even I was surprised to learn that somehow RIPTA depended on Medicaid money to keep running.
A federal clampdown on the state’s Medicaid program will cost as many as 18,000 needy Rhode Islanders their free bus passes and will force the state to make up for millions of dollars in lost transit money to avert wreaking havoc on the state’s bus system, state officials say.Only a bureaucrat and/or the most committed government=mommy proponent could possibly think that a blanket ride-the-bus-for-free pass (versus a certain allotment per year, for instance) was a legit use of Medicaid funds.The state is also expecting an attempt by the federal government to demand repayment of millions of dollars in past Medicaid money that was spent on transit. Those payments, reaching back to 1995, total more than $60 million, according to figures from the Rhode Island Public Transit Authority, although state officials say they expect the amount sought by the federal government in “recoupment” to be much smaller, between $4 million and $5 million.
The development means that the state, which paid an increasing amount of the cost of running the state bus system with Medicaid money, will now have to pick up that expense or face a major disruption, probably including bus service cuts and perhaps layoffs, at RIPTA.
DHS Director Gary Alexander said the change will affect about 18,000 of the 27,000 RIte Care members who now get bus passes, worth $45 a month. He said the other 9,000 will continue to get passes through the Family Independence Program, formerly the welfare program.Hey, I can understand the need to pay for transportation to the doctor or hospital and how there is some justification for Medicaid dollars to be used to subsidize such transport. But how did they ever think that Medicaid could be legitimately used to pay for unlimited trips to the mall, too? I guess so long as they could get away with it, it was OK, right? And now 18,000 people will be ticked off because their "right" to free transportation will be yanked. Thus does the enablement of the entitlement mindset end up hurting those who are supposed to benefit from the "helping hand." At least until the money (about $10 million) disappears.The reason for the change is that Medicaid doesn’t pay for general transportation, only for transportation related to medical treatment, according to the Centers for Medicare & Medicaid Services, which runs the Medicare, Medicaid and related programs.
January 25, 2008
Redefining Corporate Welfare
Ian Donnis points to a "strong post" (alluded to earlier) which illustrates how approximately $11.2 million of taxpayer dollars are going to government supplied health care for workers who don't get health care through their jobs.
Where is that money going, you might ask….First, a correction. The numbers above are taken from the Public Health Access Beneficiary Report and are equal to the combined total of employees + dependents covered by RIte Care / Rite Share / Medicaid, not just the employees as was claimed. In reality, the numbers of employees of Bank of America, Citizens Bank, CVS and Wal Mart that qualify for the aforementioned programs are, respectively, 112, 179, 86 and 140 (not 382, 610, 310 and 500).It is going to Bank of America, and their 382 employees on RIte Care / Rite Share/ or Medicaid. It is going to the 610 employees of Citizens Bank that are getting our taxes. It is only 310 folks at CVS (plastic bag, anyone) but 500 Wal Mart employees are paid for by the State. In total more than 4,000 workers for these corporations get us to pay for the health insurance. That, my dear reader, is corporate welfare.
Regardless of all that, underlying the charge is the false premise that companies should be obligated to provide all employees (including part time and temporary workers) health care. Last time I checked, there is no such law or rule. So companies aren't shirking their responsibilities--and taking "corporate welfare" from the government--if they never made the promise in the first place.
Additionally, as the Health Insurance Commissioner Christopher F. Koller explained in his overview of the 2005 Rhode Island Employer Survey Report (both referenced in the Public Health Access Beneficiary Report):
Faced with annual double digit premium increases, small employers are being forced to decide between increasing cost sharing with employees, dropping health benefits altogether, or taking a hit to core business performance. Employees are forced to decide between the risks of going uninsured or sharing in the rising costs.Thus, even if employers had offered generous health care benefits in the past, the economics have changed and adjustments had to be made so that companies could remain competitive. (Something the public sector seems to have a hard time grasping, incidentally). This includes reducing their ability to subsidize employee health care plans (or offer defined benefit pension plans for that matter). So long as we continue to rely on an employer-centered health care system, that is the way it will continue to be. Such reductions don't mean employers are shirking their responsibilities. Often times it's just the opposite: they're trying to remain competitive and continue to employ people.
January 15, 2008
Willful Naivete on Healthcare
Although I'm fully sympathetic with the inclination to ignore complications, I find it hard to believe that syndicated columnist Froma Harrop hasn't heard the basic argument against the following assumption, spoken this time with reference to health insurance (emphasis added):
You see, health care has become just another racket by which clever operators can scoop up fortunes. There's a ton of money to be made nickel-and-diming doctors and hospitals while making sure you don't sell insurance to sick people — and that's the legal part. Once government offers coverage, it's Game Over for the manipulators — and more of our health-care dollars go for health care.
She can't really believe such a bromide as "once government offers coverage, it's Game Over for the manipulators," can she? The manipulators just shift gears, becoming part of the government, pulling its levers, and pushing for laws favorable to them. It's a peculiarity of the liberal mind that identical problems transported to government somehow obtain a sheen of good intentions. Companies are evil because they cut corners and pressure providers in order to make a profit to sustain themselves; government is simply doing the best it can when it shaves corners through legislation and rations services to fit budgets.
From my experience, those greed-inspired businessmen are at least more likely to cut corners internally than the government, with its unionized and well-entrenched interests. The reason Harrop doesn't "hear Medicare beneficiaries clamoring for a return to private coverage" is that government services — financed systematically by somebody else's money — are more generous and less risky. They can only be so, however, at the expense of the rest of the industry and must, therefore, remain a relatively small percentage of the market.
January 10, 2008
Alzheimer's Research Breakthrough and the RI Economy
Take this with a grain of salt--it's early research after all--but there may have been a substantial breakthrough in Alzheimer's research:
A drug used for arthritis can reverse the symptoms of Alzheimer's "in minutes".For any who have been effected by Alzheimer's, this could be great news. What does this have to do with Rhode Island? The manufacturer of Enbrel--the drug used in the study--is Amgen and the drug is made right in her in its West Greenwich plant. The same facility has experienced a rough patch lately as Amgen attempted to make up for losses other areas by implementing cost-cutting measures (read: job cuts) here in Rhode Island (it appears to have worked). This new use for an established drug could mean an economic boon to the company and perhaps--eventually--more jobs here in Rhode Island.It appears to tackle one of the main features of the disease - inflammation in the brain.
The drug, called Enbrel, is injected into the spine where it blocks a chemical responsible for damaging the brain and other organs.
A pilot study carried out by U.S. researchers found one patient had his symptoms reversed "in minutes".
Other patients have shown some improvements in symptoms such as forgetfulness and confusion after weekly injections over six months.
The study of 15 patients with moderate to severe Alzheimer's has just been published in the Journal of Neuroinflammation by online publishers Biomed Central.
The experiment showed that Enbrel can deactivate TNF (tumour necrosis factor) - a chemical in the fluid surrounding the brain that is found in Alzheimer's sufferers.
When used by arthritis sufferers, the drug is self-administered by injection and researchers had to develop a way of injecting it into the spine to affect the brain cells.
Sue Griffin, a researcher at the University of Arkansas for Medical Sciences, said: 'It is unprecedented to see cognitive and behavioural improvement in a patient with established dementia within minutes of therapeutic intervention.
'This gives all of us in Alzheimer research a tremendous new clue
about new avenues of research.' Enbrel is not approved for treating Alzheimer's in the U.S. or the UK and is regarded as highly experimental, said Dr Griffin.
'Even though this report predominantly discusses a single patient it is of significant scientific interest because of the potential insight it may give into the processes involved in the brain dysfunction of Alzheimer's,' she added.
Lead author of the study Edward Tobinick, of the University of California and Director of the Institute for Neurological Research, said the drug had 'a very rapid effect that's never been reported in a human being before'.
He added: 'It makes practical changes that are significant and perceptible, making a difference to his daily living.
'Some patients have been able to start driving again. They don't come back to normal but the change is good enough for patients to want to continue treatment.'
November 30, 2007
RE: Rhode Island's Literal Depressed Status
There may be a reason the state as a whole is so depressed: not enough Republicans!
Republicans are significantly more likely than Democrats or independents to rate their mental health as excellent, according to data from the last four November Gallup Health and Healthcare polls. Fifty-eight percent of Republicans report having excellent mental health, compared to 43% of independents and 38% of Democrats. This relationship between party identification and reports of excellent mental health persists even within categories of income, age, gender, church attendance, and education.OK, I can hear the wisecracks coming. But I'll see your "blissfully ignorant" and raise you an "optimistic about the future." Regardless, I think the path to a happier state is clear, don't you?***
What are the implications of these findings?
Correlation is no proof of causation, of course. The reason the relationship exists between being a Republican and more positive mental health is unknown, and one cannot say whether something about being a Republican causes a person to be more mentally healthy, or whether something about being mentally healthy causes a person to choose to become a Republican (or whether some third variable is responsible for causing both to be parallel).
Previous analysis...shows that a number of variables are related to self-reported mental health -- including, in particular, income. Because Republicans have on average higher incomes than independents or Democrats, part of the explanation for the relationship between being a Republican and having better mental health is a result of this underlying factor. The same is true for several other variables.
But the key finding of the analyses presented here is that being a Republican appears to have an independent relationship on positive mental health above and beyond what can be explained by these types of demographic and lifestyle variables. The exact explanation for this persistent relationship -- as noted -- is unclear.
Rhode Island's Literal Depressed Status
The number and kinds of lists that Rhode Island is placing near the bottom of is starting to get just plain ridiculous. Here is yet another one from an organization called Mental Health America…
Using data from nationally representative surveys conducted by the United States government, Mental Health America created two different rankings of the states: one showing the state rankings of depression and one showing the state rank in terms of suicide rates.Four different measures of depression and mental health status were used to develop one composite measure of the level of depression in a given state. The four measures were: (1) the percentage of the adult population experiencing at least one major depressive episode in the past year, (2) the percentage of the adolescent population (ages 12 to 17) experiencing at least one major depressive episode in the past year, (3) the percentage of the adult population experiencing serious psychological distress, and (4) the average number of days in the past 30 days in which the population reported that their mental health was not good….
- (12) Vermont
- (16) Massachusetts
- (20) New Hampshire
- (38) Connecticut
- (41) Maine
- (48) Rhode Island
November 4, 2007
A Note for Our Dialogue
Well, if we're all going to sit around the table and resolve the healthcare crisis in Rhode Island, as Lt. Gov. Elizabeth Roberts wishes, I'd like to make sure that this sort of testimony doesn't slip out of sight onto the floor:
Unfortunately Sicko is a dishonest film. That is not only my opinion. It is the opinion of Professor Lord Robert Winston, the consultant and advocate of the NHS. When asked on BBC Radio 4 whether he recognised the NHS as portrayed in this film, Winston replied: "No, I didn't. Most of it was filmed at my hospital [the Hammersmith in west London], which is a very good hospital but doesn't represent what the NHS is like."I didn't recognise it either, from years of visiting NHS hospitals. Moore painted a rose-tinted vision of spotless wards, impeccable treatment, happy patients who laugh away any suggestion of waiting in casualty, and a glamorous young GP who combines his devotion to his patients with a salary of £100,000, a house worth £1m and two cars. All this, and for free.
This, along with an even rosier portrait of the French welfare system, is what Moore says the state can and should provide. You would never guess from Sicko that the NHS is in deep trouble, mired in scandal and incompetence, despite the injection of billions of pounds of taxpayers' money.
October 29, 2007
Making It Your Job to Stay Healthy
The economics of changing insurance rates based on demonstration of a healthy lifestyle are simply to understand. Still, do we really wish to make it the responsibility of employers to enforce those lifestyles?
[State Health Insurance Commissioner Christopher F.] Koller explained that HEALTHpact was created, at the direction of Governor Carcieri and the General Assembly, as an alternative to high-premium, high-deductible, reduced-coverage health insurance that small-business owners have shunned.It requires managers and workers to be more engaged in the process of buying health insurance.
To qualify for the least-costly policy under HEALTHpact, a worker must complete a “health risk assessment” that includes a pledge to lower body weight, stop smoking and participate in disease/case management. After that, there are regular assessments, and if the employee does not comply with the requirements, the deductible goes up — significantly.
It seems far more rational, to me, to make health insurance an individual thing and then to offer discounts — adjust premiums — to those who live healthily. Lowering my blood pressure and cholesterol shouldn't be a concern of my employer, at least inasmuch as it doesn't affect my performance.
October 25, 2007
Roland Benjamin: The Problems with Medicare-for-All
Hyperbole aside, Robert Whitcomb’s Projo op-ed from October 19 can be summarized by his one statement:
In short, extend Medicare to everyone.He proceeds to use exaggerated estimations of private insurance overhead costs and completes his argument by saying:
Then we would not have to hang our heads in shame that Americans are the most unhealthy people of any developed nation.The administrative assumptions of Whitcomb’s argument are suspect at best, and fatally flawed at worst. A white paper from the Manhattan Institute, published a few weeks ago, analyzes the holes in the Medicare-for-All debate. To support his claim of efficiency, Whitcomb estimates that non-benefit expenses in the private insurance market are near 25%, while the same expenses are only 2% for Medicare administration.
The Manhattan paper cites all the usual sources from both sides of the debate like Krugman, Council on Affordable Health Insurance, Rand, Commonwealth, Kaiser Family Foundation, etc. and points out a few interesting analyses. Notably, administrative costs of Medicare are nowhere near the 2% Whitcomb describes in his piece (nor are private costs anywhere near the 25% number). The paper uses conservative estimates of 14% private (while citing estimates as low as 11%) and 6% Medicare to make the claim that the theorized savings by transition are impossible to realize. Private carrier rates are confirmed locally by a study from the Rhode Island Office of the Health Insurance Commissioner citing total benefit payouts by carriers at 85.2% of premiums (or 14.8% non-benefit spending, including some percentage for taxes). The Medicare rate shifts dramatically, for example, when fraud expenses are classified as non-benefit expense instead of actual benefit spending. An apples to apples comparison using consistent accounting methods shows the true cost of Medicare between 6% and 8%.
The Manhattan study then goes on to describe the evolving nature of spending by those who would be newly insured under the policy and underscores the deficit that will be realized based on static assumptions. Finally, the white paper describes the response to tax policy that will inevitably result. Migrating the funding system to a Medicare style payroll tax will increase explicit labor cost in the US.
Currently, payroll taxes cover Medicare, private insurance premiums cover the health care of active employees and dependents and some income taxes cover another portion of health care spending. In the three buckets (or more), the costs tied to labor are less explicit and more dispersed. Take all of those costs and apply them in one bucket that is explicitly tied to labor and there will be a problem. Like it or not, corporate behavior responds to tax policy with amazing agility and immediacy. Increase the cost to employ directly, and work will move to regions where labor costs less. Or in the best case, capital investments facing a lower ROI bar will be exploited where labor can be replaced with automation. Reduce the workforce, or the value of a skilled workforce, and the tax base drops, perpetuating the spending deficit in an otherwise well intentioned policy.
The economic argument of Medicare for All has the underpinning that the cost of the uninsured is at the root of the health care inflationary problem. Yet I have not seen convincing data that this is true. No studies that I have seen refute either of these two facts:
- Uncompensated care to the uninsured is not a top tier cost driver. Kaiser shows uncompensated care around 2.05% of all health care spending, while others show the impact at less than one percent. Defensive medicine accounts for anywhere from 3 to 10 times that amount depending on the definition. Rx sales of the top 15 drugs alone exceed the total amount of uncompensated care. And so on and so on…
- Uncompensated care to the uninsured has not inflated at the same pace as overall spending. In fact, the inflation rate of spending by the uninsured has kept pace or lagged behind normal inflation since 2000 (this comes right from the Medical Expenditure Panel Survey MEPS). Meanwhile, the spending by the insured has increased at alarming rates. The economic problem lies with those currently insured. Bringing more individuals into that system, and providing the same or more insulation from real prices will only aggravate the situation.
The only argument to be made for insuring all via Medicare type arrangement then is a moral one. While well intentioned, the demographics of the uninsured suggest that the moral argument may be shaky as well. With 93% either opting out of available insurance for non-affordability reasons, without insurance for less than 4 months, or without citizenship status, there may be as few as 4 million people who would truly benefit from the coverage. These are the people that are at or beyond their ability to afford or access coverage today. This would also be the population most likely impacted when the inevitable labor shifts occur in response to changing tax policy. To use the same hyperbole that Whitcomb employs, would it be moral to give someone insurance, only to have their job become prematurely obsolete or permanently displaced?
October 22, 2007
Behold the People's Glorious Five Year Plan
I wonder, when Lieutenant Governor Elizabeth Roberts proposes a five-year plan for healthcare reform, followed by Projo columnist Charles Bakst writing approvingly of it…
It was a pleasure to hear Lt. Gov. Elizabeth Roberts deliver a thoughtful speech Tuesday calling for a program of compulsory, affordable health insurance for Rhode Islanders....…is it the result of a lack any sense of historical irony, or of a sincere belief that government-created five-year plans are unquestionably the best way to do things, but have never properly been tried?"Where is the vision? Rather than whittling away at our safety net and trimming at the edges of the personnel budget, we should be thinking about the long-term role of government", [asked Lt. Governor Roberts]....
She pledged to work to bring interested parties together to devise a five-year plan;
Behold the People's Glorious Five Year Plan
I wonder, when Lieutenant Governor Elizabeth Roberts proposes a five-year plan for healthcare reform, followed by Projo columnist Charles Bakst writing approvingly of it…
It was a pleasure to hear Lt. Gov. Elizabeth Roberts deliver a thoughtful speech Tuesday calling for a program of compulsory, affordable health insurance for Rhode Islanders....…is it the result of a lack any sense of historical irony, or of a sincere belief that government-created five-year plans are unquestionably the best way to do things, but have never properly been tried?"Where is the vision? Rather than whittling away at our safety net and trimming at the edges of the personnel budget, we should be thinking about the long-term role of government", [asked Lt. Governor Roberts]....
She pledged to work to bring interested parties together to devise a five-year plan;
October 19, 2007
Just One Thing, Mr. Whitcomb
In a signed editorial that doesn't appear to be online, Providence Journal Editorial Pages Editor Robert Whitcomb suggests that the simple solution to America's healthcare problem is to expand Medicare to encompass everybody:
The Republicans will do anything but go to thye simplest, most cost-effective reform — putting everyone into Medicare. The latter's overhead: 2 percent; for-profit insurance companies': 25 percent. Why must everything in health care be done in such complicated and expensive ways? The reason is simple: Because rich and powerful people profit from the current arrangements. ...... Americans are hungry for such reform. As it is, America has the worst healthcare system in the developed world — it's unfair, unbelievably inefficient and complicated, and grossly expensive. The best way to reform it is to disconnect health insurance from the workplace and to make sure that everyone is in the same national pool — the healthy and the unhealthy. That's what makes insurance plans fair and efficient, not the current cherry-picking arrangements.
In short, extend Medicare to everyone. And for minor medical problems, people should pay out of their own pockets, which would act as an economic discipline. The invisibility of real costs to many people with insurance has driven up overall costs. Medicare, like all insurance, should be for serious problems.
Clearly, Mr. Whitcomb is not proposing just an extension of Medicare, as it exists, to everybody. He would limit insurance to "serious problems" (I agree). He would require people not to insulate themselves from the process that turns their money into the health services that they use (again, I agree). He would disconnect health insurance from employment. Ah, now there's the thing.
A quick refresher on how Medicare is funded:
The two parts of traditional Medicare are funded in very different ways. Part A, which covers in-patient hospital bills, is financed by a trust fund known as the Hospital Insurance Fund (HI Fund).The 1.45 percent that the government deducts from your paycheck -- and also from your employer -- is placed in the HI Fund to cover Part A services. This payroll tax provides the bulk of the money that flows into the HI Fund; that money is in turn used to cover Part A expenses.
Part B, which covers doctor appointments, is run by a separate trust fund, called the Supplemental Medical Insurance Trust Fund (SMI Fund). Enrollee premiums and funds from the general budget supply the SMI Fund, which then pays for Part B services.
So, for Part A, you currently pay 1.45% of your salary and your employer pays the same amount again on your behalf, as it were. The link between healthcare and employment remains as a function of Medicare's structure. Now consider that this money associated with your salary currently covers just over 25% of a senior's healthcare. By 2075, every two workers will be paying for a single retiree, so the percentage of salary will have to go up to roughly 6% (employee and employer contributions) to maintain the equivalent services.
Were everybody to dive into the Medicare pool, the ratio would become approximately 0.8 workers per recipient, making the percentage contribution a little under 13% of salary. Sharp readers will have noticed that I've forgotten an additional consideration that I haven't the time to work through, just now: If Medicare covered everybody, each worker would also be paying for those who are unemployed, whether they are adults or children. My guess is that the percentage of salary would increase to an amount at least as high as the combined contribution that my employer and I currently make to my healthcare. In other words, "including everybody in Medicare" isn't but so different from requiring all employers to offer healthcare to their employees' families, with an additional fund for unemployed and retired adults.
And nothing above addresses the increased cost of "enrollee premiums and funds from the general budget" that would have to be raised via taxes for Part B. I don't know from where Whitcomb took his overhead numbers, but it isn't at all clear to me that my cost — taking myself as an example of exactly the sort of head of struggling household whom healthcare costs could easily break — would improve, as an absolute matter or in relation to services.
Worse yet, the risk is surely tremendous that the system would change when it shifts from covering a minority to being the only game in town — and one run ultimately by politicians. Who will decide what are "minor medical problems"? Who will decide from whom it is proper to demand payment for non-emergencies? The answer cannot be other than "rich and powerful people," back again, but with a government-sanctioned monopoly.
October 3, 2007
S-CHIP Veto
The President vetoed the bill that sought to expand the S-CHIP program and our usual suspects piped up with the same old hyperbole:
“Playing politics with the health care coverage of 10 million children is unacceptable, but that is exactly what President Bush did today when he vetoed H.R. 976, the reauthorization of the State Children’s Health Insurance Program, better known as RIte Care in Rhode Island,” Rep. Jim Langevin said.The fact is, the President would support a reauthorization, just not at the level Congress wants. And they knew it, so this is being played for political points, nothing else. Sure, there are some Republican Senators who are playing along, but I think it's because they like the idea of expanding government health-care into the middle-class for, shall we say, electoral reasons...Here's the President's explanation:Langevin called it a "bipartisan plan" that would help more than 30,000 low-income Rhode Island children while not changing eligibility rules.
"I look forward to the opportunity to cast my vote to override this unfortunate and misguided veto," Langevin said.
Sen. Sheldon Whitehouse said the veto “is a stunning rejection of one of America’s most deeply-held convictions: that every family, and every child, must have access to health care they can afford."
Rep. Patrick Kennedy said it is “unconscionable" that Bush would veto something "aimed at providing 10 million children the health care they deserve. The President’s veto of the State Children’s Health Insurance Program is a slap in the face to families all across America."
First of all, the intent of the S-CHIP legislation passed previous to my administration is to help poor children's families buy the children health care, or get them on health care. That's what it is intended to do. Poor children in America are covered by what's called Medicaid. We spend about -- this year -- about $35.5 billion on poor children's health insurance....The S-CHIP program was supposed to help those poor families, the children of poor families have the ability to get health insurance for their children. I strongly support the program. I like the idea of helping those who are poor be able to get health coverage for their children....As a matter of fact, my budget -- the budget request I put in said, let's increase the spending to make sure that the program does what it's supposed to do: sign up poor children for S-CHIP....Some have run the numbers and discovered the extent of the bloat:I want to tell you a startling statistic, that based on their own states' projections -- in other words, this isn't a federal projection, it's the states saying this is what's happening -- states like New Jersey, Michigan, Minnesota, Rhode Island, Illinois and New Mexico spend more money on adults in the S-CHIP program than they do on children. In other words, the initial intent of the program is not being recognized, is not being met.
It is estimated by -- here's the thing, just so you know, this program expands coverage, federal coverage up to families earning $83,000 a year. That doesn't sound poor to me. The intent of the program was to focus on poor children, not adults or families earning up to $83,000 a year....
This would involve expanding the program to cover 4 million more children and adding $35 Billion to its cost, over the next five years. Assuming the dollars are base year and uniformly phased, the Senate version of S-CHIP makes the annual cost of the program increase from $4 Billion to $11 Billion. This would increase program costs by 175% on the top line.Finally, one of the sponsors of the original S-CHIP legislation is against this new expansion:The unit cost per child insured also increases dramatically. The original program insured 6.9 million children, at a price of $4 Billion a year, for a unit price per child insured of approximately $580. The Senate program extension would insure roughly 11 Million children at approximately $11 Billion per year, for a cost of $1,000 per child. This is an increase of $420 per child, or a unit cost growth of 72%.
“I want to thank Majority Leader Henry Reid for recognizing that I cast the only correct vote about SCHIP in the state of Maryland,” said Congressman Roscoe Bartlett upon learning that the Senate Majority Leader mentioned today there was only one vote in Maryland to sustain the President’s veto of the SCHIP expansion.And so are some Republicans.Congressman Bartlett added, “I’m proud that I voted to create the SCHIP program in 1997. I want to help the working poor, but Democrats are demanding that SCHIP be expanded to have government-controlled, taxpayer-paid health care for millions of children who already have private health coverage.”
September 16, 2007
Poor Diagnoses, or Munchausen by Proxy?
Rhode Island Kids Count's Jill Beckwith is correct that Rhode Island is "heading in the wrong direction" when it comes to healthcare. According to Projo Medical Writer Felice Freyer, fewer Rhode Island workers have healthcare coverage, a higher percentage of children are without it, and yet:
Rhode Island spends a higher proportion of its economy and its state budget on health care than the rest of New England and the nation.
Why, then, do three of the four recommendations that Freyer reports from "a first-of-its-kind report" by the state's health insurance commissioner, Christopher Koller, call for increased public aid, with the fourth suggesting that the state "require employers to offer health insurance and individuals to buy it"? Either the problem is being misdiagnosed, or the care-for-you community in the public sphere has a social manifestation of Munchausen by proxy (the disease that led that mother in The Sixth Sense to spoon Pine-Sole into her daughter's soup).
Don't misunderstand: requiring people to buy their own health insurance is a key component of the solution that I've increasingly been favoring, but in typical Rhode Island fashion, it looks as if the powers that be are fixin' to get it all wrong. Expanding the number of people who can claim publicly funded insurance while leaning on companies and slightly wealthier individuals (such as those at three times the poverty level), and while taking no steps to decrease regulations or draw additional insurers to our local market, will only reinforce the trends that are killing the state.
If, for instance, RI Senate Majority Leader Teresa Paiva Weed should decide to act on her observation that (in Freyer's words) "it may be difficult to regulate large employers because many are self-insured," large employers will have one more incentive leave, even as disproportionate handouts continue to spur the needy to come.
September 6, 2007
Never Know Unless You Ask
There's an odd omission from Steve Peoples's article about the new medicine copays for impoverished recipients of state aid. We get the policy's numbers:
McCaffrey is among 14,000 impoverished Rhode Islanders on fee-for-service Medicaid who will be asked to shoulder a portion of their prescription drugs — $1 for generics and $3 for brand-name drugs — as of Oct. 1. The fees were enacted by the General Assembly in the state budget, part of a larger effort to close a massive budget deficit.State officials say the copays will save state taxpayers nearly $600,000.
McCaffrey, who is disabled and receives $680 each month, estimates her monthly drug costs will grow to about $16.
We get the sad story:
McCaffrey, 47, needs medicine to function. The disabled Providence woman takes eight medications each day for a list of ailments that include major depression, asthma, diabetes and posttraumatic stress disorder.
We get the incensed calls for the government to spend money advertising a loophole:
"It's outrageous, shameful really, that DHS made a deliberate decision ... not to tell people that, under federal and state law, the drugstore has to fill their prescription if they are unable to afford the copay," Mary Curtain, a paralegal with Rhode Island Legal Services, said at yesterday's hearing.
We even get the Rhode-Island-suffers-in-a-national-comparison factoid:
In charging copays for this program, Rhode Island is not unique. More than 40 states already do, according to the federal Center for Medicare and Medicaid Services.
But nobody in the story offers — nor does Mr. Peoples ask about — suggestions of familial or community charity. Apparently, nobody worth quoting for the story is able to come up with creative ideas for helping the most needy among us drum up sixteen bucks a month for medicine. How about a jar at the pharmacy counter? How about a community fundraiser? What if kids — under the heading of Civic Participation — volunteered for short bursts of work (either in pharmacies or elsewhere) and donated their pay to a copay fund?
Why, in this state, must it always be career advocates pushing the government to find ways of forcing one group of citizens to bankroll another? Sure, the extra government spending for this program, set apart from the rest, amounts to very little for the average taxpayer, but it is not set apart, and the very littles add up. As for the costs to the individual in dependency and to the community in apathy, those are incalculable.
August 28, 2007
United States Leads All Developed Countries -- Even Those With Universal Health Care -- In Cancer Survival
According to a study published in The Lancet Oncology medical journal, the United States has the best cancer survival rate in the developed world. The tables below are from an article on the study published in Britain's Daily Telegraph (h/t Andrew Stuttaford)…
| USA | 62.9% |
| Iceland | 61.8% |
| Sweden | 61.7% |
| Belgium | 61.6% |
| Finland | 61.1% |
| Switzerland | 61.1% |
| Italy | 59.7% |
| Spain | 59.0% |
| Germany | 58.8% |
| Norway | 58.4% |
| Netherlands | 58.3% |
| Austria | 58.0% |
| Malta | 54.6% |
| Wales | 54.1% |
| Slovenia | 52.9% |
| England | 52.7% |
| Ireland | 51.9% |
| N. Ireland | 51.0% |
| Czech Republic | 49.3% |
| Poland | 48.3% |
| Scotland | 48.0% |
| USA | 66.3% |
| Sweden | 60.3% |
| Iceland | 57.7% |
| Finland | 55.9% |
| Austria | 55.4% |
| Switzerland | 54.6% |
| Belgium | 53.2% |
| Norway | 52.0% |
| Germany | 50.0% |
| Italy | 49.8% |
| Spain | 49.5% |
| Ireland | 48.1% |
| Wales | 47.9% |
| Netherlands | 47.1% |
| England | 44.8% |
| Malta | 42.3% |
| N. Ireland | 42.0% |
| Scotland | 40.2% |
| Poland | 38.8% |
| Czech Republic | 37.7% |
| Slovenia | 36.6% |
"Survival rate" was defined as "the number of patients who are alive five years after diagnosis".
The Telegraph article, focused on Britain's poor showing in the study, contains a couple of notable observations…
For women, England was the fifth worst in a league of 22 countries. Scotland came bottom. Cancer experts blamed late diagnosis and long waiting lists.… Prof Richard Sullivan at Cancer Research UK said: "Cancer is still not being diagnosed early enough in all cases."
But wait – I thought this wasn't possible in a country with a "universal" health care system. Don't universal health care proponents promise that universality guarantees that everyone will have their illnesses diagnosed early?A second article, which looked at 2.7 million patients diagnosed between 1995 and 1999, found that countries that spent the most on health per capita per year had better survival rates.
Contrary to what the folk-Marxists out there argue, not every problem can be solved by increasing the resources controlled by government. How money gets spent matters. And big government bureaucracies are simply not the best option for making medical decisions that will have life or death impacts on individual people.Britain was the exception. Despite spending up to £1,500 on health per person per year, it recorded similar survival rates for Hodgkin's disease and lung cancer as Poland, which spends a third of that amount.
August 26, 2007
ProJo: Teacher Benny's "All over the board"
The ProJo reports that teacher benefits in RI are "all over the board" and gives some stats in the differences among plans by district and differences in buyback options. It's an old and familiar tune around here, but the central point is worth repeating:
Last year, after a decade in which health insurance emerged as a critical and contentious contract issue, 33 of the state’s 36 districts required some form of cost sharing. But teacher contribution still trails private sector workers in the state by a wide margin — although in some communities teachers are paying far more than other public employees.Hey, school boards and city councils are as at fault as the unions here, folks. In the world of collective-bargaining, they haven't been up to snuff (even granting their amateurish experience versus those employed by unions solely to bargain). But maybe going forward, they can take Rhode Island Federation of Teachers President Marcia Reback statement--that “to the people I represent, health insurance is as important — if not more important — than salaries"--as a way to prioritize negotiable line-items. But perhaps the biggest line-item that can be dispensed with is the asinine "buy back" options that are still included in nearly all state contracts--teacher and otherwise. It can't be that difficult to determine if an employee is covered by their public-employee spouses health insurance, can it?
July 24, 2007
The Wisconsin Universal Coverage Plan
Today’s OpinionJournal has an editorial describing a universal health care plan proposed for Wisconsin. To borrow a phrase from Ian Donnis, the budget numbers are eye-popping…
Democrats who run the Wisconsin Senate have dropped the Washington pretense of incremental health-care reform and moved directly to passing a plan to insure every resident under the age of 65 in the state. And, wow, is "free" health care expensive. The plan would cost an estimated $15.2 billion, or $3 billion more than the state currently collects in all income, sales and corporate income taxes. It represents an average of $510 a month in higher taxes for every Wisconsin worker.Pro-rating the total dollars spent by population (5.5 million in Wisconsin, versus about 1 million in Rhode Island), the cost of a similar plan for Rhode Island would carry an estimated price tag of about 2.7 billion dollars, or about 80% of existing general revenues.Employees and businesses would pay for the plan by sharing the cost of a new 14.5% employment tax on wages. Wisconsin businesses would have to compete with out-of-state businesses and foreign rivals while shouldering a 29.8% combined federal-state payroll tax, nearly double the 15.3% payroll tax paid by non-Wisconsin firms for Social Security and Medicare combined.
Basically we’re talking about making state governments into giant health insurance companies and making all other state government functions into side-operations of the super-insurers.
Wisconsin officials realize that many people aren’t going to be satisfied with their state-controlled coverage (especially if it’s run with the same competence that states have applied to say, public pension funds), so they’re moving immediately to block alternatives…
The plan is also openly hostile to market incentives that contain costs. Private companies are making modest progress in sweating out health-care inflation by making patients more cost-conscious through increased copayments, health savings accounts, and incentives for wellness. The Wisconsin program moves in the opposite direction: It reduces out-of-pocket copayments, bars money-saving HSA plans, and increases the number of mandated medical services covered under the plan.Wisconsin officials are conceding that that their plan will force many people to pay high prices for coverage that doesn’t make sense for them and therefore are denying access to plans that would give people better ability to tailor coverage to their individual needs. It’s a perfect example of the standard excess of big-government: If you don’t have the imagination or skill or desire to build a better mousetrap, then make building new styles of mousetrap illegal!So where will savings come from? Where they always do in any government plan: Rationing via price controls and, as costs rise, waiting periods and coverage restrictions.
July 19, 2007
Too Many Sperm Being Injected in Rhode Island
Anecdotal evidence of the unintended consequences of insurance mandates and bureaucratically-set healthcare pricing, courtesy of the Associated Press…
Fertility clinics are overusing a laboratory technique and costing infertile couples and some insurers hundreds of extra dollars, a new study suggests.Now, I know there are some critics of the current healthcare system will say this is clearly a result of the evils of for-profit medicine, but that argument doesn't fly here.At issue is a procedure that injects a single sperm into an egg. The method is considered the best option for couples in which the man has defective sperm or extremely low sperm counts.
But many clinics are using it for other infertile couples, even though it often doesn’t work as well as the standard lab dish method, according to a study in Thursday’s New England Journal of Medicine.
Sperm injection adds about $1,500 to the $12,400 average cost of an in vitro fertilization treatment cycle, the authors said.
“This paper is particularly troubling because we’ve got a major shift in practice that isn’t evidence driven. The paper suggests it may be driven by money,” said Arthur Caplan, director of the University of Pennsylvania’s Center for Bioethics and a contributing writer for MSNBC.com's Breaking Bioethics column....
The research team reviewed a decade of results that hundreds of fertility clinics reported to the federal government. In 2004, about 58 percent of treatment attempts included sperm injection — up from 11 percent in 1995.
But the proportion of couples who have trouble conceiving because of the man’s sperm has stayed constant, at around 34 percent. This suggests that the sperm-injection technique is being urged on many couples who do not need it and might be better off with traditional lab dish, or in vitro, fertilization, Caplan said.
Sperm injection does not increase overall success rates for healthy births. The researchers found that among infertility treatment attempts with successful egg retrievals in 2004, about 31 percent of those involving sperm injection resulted in a live birth. The percentage was higher — 33 percent — for those that did not use the sperm injection....
They also noted that sperm-injection rates were higher in three states — Illinois, Massachusetts and Rhode Island — that mandate coverage of the technique than in states without such a requirement.
Prices for medical procedures in America today are set by a mixture of private and public insurance bureaucracies. (And if you don't like the price specified by your insurer, too bad; you have little opportunity to go elsewhere, because of our employer-based healthcare system). Since insurance companies set the reimbursement rates, it’s doubtful that doctors can be blamed for conspiring to establish a bigger profit margin for the injection versus the lab dish procedure. And since the insurers don't provide the actual service, they can't be making more money by encouraging higher-priced treatments.
That leaves at least two explanations, in the absence of evidence of medical necessity, for the growing preference for injection treatments...
- There are different profit margins for the two procedures, resulting from the fact that bureaucratically established prices have not responded efficiently or rationally to the true costs of providing treatments, and some doctors are indeed getting greedy.
- Alternatively, note that the AP story states only that the price of the injection treatment is higher, not that the profit margin is higher. The increase in injections could also result from the fact that some patients figure the higher-cost treatment must be the better treatment, and since they're paying the same amount for either treatment (assuming the price of both treatments exceed their deductible), that's the treatment they choose.
June 29, 2007
Truth: An Antidote to Sicko
Having watched Michael Moore's latest bit of propaganda — Sicko, about the evil of American healthcare in comparison to saintly socialism — a bit more closely than is probably healthy, David Gratzer felt compelled to offer another view:
Consider, for instance, Mr. Moore's claim that ERs don't overcrowd in Canada. A Canadian government study recently found that only about half of patients are treated in a timely manner, as defined by local medical and hospital associations. "The research merely confirms anecdotal reports of interminable waits," reported a national newspaper. While people in rural areas seem to fare better, Toronto patients receive care in four hours on average; one in 10 patients waits more than a dozen hours.This problem hit close to home last year: A relative, living in Winnipeg, nearly died of a strangulated bowel while lying on a stretcher for five hours, writhing in pain. To get the needed ultrasound, he was sent by ambulance to another hospital.
In Britain, the Department of Health recently acknowledged that one in eight patients wait more than a year for surgery. Around the time Mr. Moore was putting the finishing touches on his documentary, a hospital in Sutton Coldfield announced its new money-saving linen policy: Housekeeping will no longer change the bed sheets between patients, just turn them over. France's system failed so spectacularly in the summer heat of 2003 that 13,000 people died, largely of dehydration. Hospitals stopped answering the phones and ambulance attendants told people to fend for themselves.
No wonder, Gratzer observes, single-payer systems worldwide are beginning to make way for private healthcare, even as Western dead-enders push for the only fair system — one in which the wealthy can travel great distances and pay high prices for rapid service while the average shmoe is forced into compliance with Darwin's prescription.
Sheesh! What do we plebs think "privilege" means?
June 1, 2007
Another Argument for In-Store Health Clinics
In an op-ed in today's Projo about CVS' proposed network of in-store health clinics, Joann Fitzpatrick (a retired editor for the Quincy Patriot Ledger) argues that much of what appears to be a healthcare "crisis" is really the result of an inflexible system that poorly aligns available resources with people's needs...
Our confusing, overpriced health-care system needs a lot of changes and high on the list is flexibility. That means flexibility in the attitude of health-care providers — including medical professionals and insurers — and in the delivery of health care. Too often patients must negotiate a labyrinth of rules and requirements just to see a doctor for a simple ailment....[CVS MinuteClinics] answer the needs of working families and of those who don’t necessarily have a primary-care physician, or insurance. For a parent, taking a child with a sore throat or cough to a clinic rather than a busy pediatrician’s office can mean the difference between being an hour late for work or missing half a day. For a twenty-something without a personal physician, having a rash looked at and treated for $59 is the cost of a few drinks at a downtown bar....
Consumers need to become their own advocates for good health care. We can’t expect everyone to navigate insurance rules and increasingly complex modern medicine with ease. But consumers should be seeking value for their health-care dollar as much as they do with grocery bills.
May 24, 2007
The Financial Times on Walk-in Health Clinics
Eventually, the big international business papers are able to catch up to Anchor Rising’s coverage of an issue. Here’s the Financial Times on the movement towards in-store health clinics by companies such as Wal-Mart and CVS…
Walk-in clinics represent one of the most advanced and aggressive attempts by US business and entrepreneurs to drive reform of the healthcare system.Here’s the anti-clinic arguments presented in the article, which I’ll admit, I don’t find very convincing…This year hundreds will be opened in some of the US’s largest drugstore and retail groups, and thousands of clinics could be running in the next decade.
Advocates say the clinics will improve access to healthcare and reduce costs; that they will reduce more expensive visits to hospital emergency rooms; and that they will catch some illnesses before they become serious and costly. As a result, physicians will have more time for complex cases….
More than anything, however, the retail clinics show that business is pushing for change on its own without waiting for government. And walk-in clinics could do for US healthcare what low-cost Southwest Airlines did for the airline industry, by making healthcare better, faster, and cheaper.
First, despite US business’s push to inject and increase consumer principles into healthcare, it is still unproven whether people understand how to shop for medical care like other products, or even whether they want to do so. Clinics also could be a controversial way for employers to push more health costs on to employees.Not to make too much of a direct comparison, but isn’t the philosophy that it’s OK to have a system that doesn’t really work as long as nobody makes money the philosophy that killed the old Communist bloc?Second, retail clinics claim they will increase doctors’ business by referring new patients or allowing them to spend more time on higher-value tasks. But experts agree that they could be sapping high-margin, easy tasks like vaccinations from doctors’ businesses, and that clinics do not yet generate significant referral business to doctors.
Third, the clinics are for-profit businesses. Dr Osborn, of Illinois, says: “They’re not at this to increase doctors’ business; they’re in it to make money. That’s a smokescreen.”
May 16, 2007
Re: Warwick City Council Rejects $1 Million in Budget Savings
Dan Yorke just had Warwick City Councilman Steve Merolla on to talk about why the City of Warwick has eschewed an additional $1 million in cost-savings by deciding to stay with Blue Cross/Blue Shield instead the cheaper United Healthcare as manager of the City's employee healthcare plan. (The "manager" distinction is important--Warwick pays its own claims, the healthcare provider only administers it. That means a claim rejected by the provider can be appealed to the City, which can decide to pay it anyway).
Merolla stated there were many city employee union members in attendance at the meeting and they made it clear they would be unhappy if United was chosen. Merolla himself was threatened by someone in the gallery at the meeting (he's filed a police report). It's Merolla's belief that this intimidation was a factor in why the majority of the City Council ignored the recommendation of it's own, appointed consultant and voted to stay with BC/BS and cost the City of Warwick nearly $1 million.
Finally, Yorke asserted that BC/BS is bought an paid for by unions. Currently, there are three union members on the BOD, including Chairman of the Board, Frank J. Montanaro, President of the Rhode Island AFL-CIO.
April 25, 2007
Wal-Mart to Open In-Store Health Clinics Nationwide
Blogger Mickey Kaus calls a news item directly impacting multiple blog-topics a "harmonic convergence" of issues. I think it’s fair to consider this news from Wal-Mart a harmonic convergence within the Rhode Island blogosphere…
Wal-Mart Stores, Inc., intends to contract with local hospitals and other organizations to open as many as 400 in-store health clinics over the next two to three years, and if current market forces continue, up to 2,000 clinics could be in Wal-Mart stores over the next five to seven years, Wal-Mart president and CEO Lee Scott will say in a speech later today at the World Health Care Congress in Washington, D.C. The clinic program's expansion is just the latest in a series of moves by Wal-Mart to help implement customer solutions to America's health care crisis, including the $4 generic drug prescription program, health information technology and participation in a major coalition supporting comprehensive healthcare reform by 2012.Wal-Mart puts appeals to all kinds of health policy wonks into their press release…
Scott notes that surveys in existing clinics revealed more than half of those who visited a clinic said they were uninsured. Nearly 15 percent of customers said they would have gone to a hospital emergency room for their care -- thus increasing the burden on already strained community health care institutions -- if they could not have gone to the clinic inside a Wal-Mart.(Note that this part of the Wal-Mart proposal is different from CVS's description of its in-store clinic plan, which mentions only nurse practitioners.)The providers running the clinics will determine what services to offer, which will generally include preventive and routine care for conditions such as allergies and sinus infections, as well as basic services such as cholesterol screenings and school physicals at affordable prices. They will be staffed by either certified nurse practitioners or physicians.
"We also think there is tremendous potential with local hospitals as partners for some or all of these clinics. Patients trust the role hospitals play in providing quality medical care. They have the medical experience and expertise -- and the larger network if more serious treatment is needed," Scott says.Related items:The clinics will post clear prices for services and procedures, helping to bring much-needed price transparency to the American health care system.
Scott highlights Wal-Mart's work on health information technology, pointing to Wal-Mart's partnership with other corporations to start Dossia, an independent, non-profit group that will provide safe and secure electronic medical records to their employees and retirees. Wal-Mart recently joined with the University of Arkansas and Blue Cross Blue Shield to create the Center for Innovation in Health Care Logistics, a new research center focused on improving health care delivery through information technology.
Wal-Mart is also working with leaders in business, government, labor and public policy on the "Better Health Care Together" coalition. The goal of the coalition is to assure that affordable, quality health care is accessible to all Americans by 2012
- Anchor Rising on in-store health clinics here.
- Anchor Rising trying to understand the emergency room crisis here.
- Anchor Rising on universal healthcare here and here.
- RI Future's disdain for all things Wal-Mart here and here.
Wal-Mart to Open In-Store Health Clinics Nationwide
Blogger Mickey Kaus calls a news item directly impacting multiple blog-topics a "harmonic convergence" of issues. I think it’s fair to consider this news from Wal-Mart a harmonic convergence within the Rhode Island blogosphere…
Wal-Mart Stores, Inc., intends to contract with local hospitals and other organizations to open as many as 400 in-store health clinics over the next two to three years, and if current market forces continue, up to 2,000 clinics could be in Wal-Mart stores over the next five to seven years, Wal-Mart president and CEO Lee Scott will say in a speech later today at the World Health Care Congress in Washington, D.C. The clinic program's expansion is just the latest in a series of moves by Wal-Mart to help implement customer solutions to America's health care crisis, including the $4 generic drug prescription program, health information technology and participation in a major coalition supporting comprehensive healthcare reform by 2012.Wal-Mart puts appeals to all kinds of health policy wonks into their press release…
Scott notes that surveys in existing clinics revealed more than half of those who visited a clinic said they were uninsured. Nearly 15 percent of customers said they would have gone to a hospital emergency room for their care -- thus increasing the burden on already strained community health care institutions -- if they could not have gone to the clinic inside a Wal-Mart.(Note that this part of the Wal-Mart proposal is different from CVS's description of its in-store clinic plan, which mentions only nurse practitioners.)The providers running the clinics will determine what services to offer, which will generally include preventive and routine care for conditions such as allergies and sinus infections, as well as basic services such as cholesterol screenings and school physicals at affordable prices. They will be staffed by either certified nurse practitioners or physicians.
"We also think there is tremendous potential with local hospitals as partners for some or all of these clinics. Patients trust the role hospitals play in providing quality medical care. They have the medical experience and expertise -- and the larger network if more serious treatment is needed," Scott says.Related items:The clinics will post clear prices for services and procedures, helping to bring much-needed price transparency to the American health care system.
Scott highlights Wal-Mart's work on health information technology, pointing to Wal-Mart's partnership with other corporations to start Dossia, an independent, non-profit group that will provide safe and secure electronic medical records to their employees and retirees. Wal-Mart recently joined with the University of Arkansas and Blue Cross Blue Shield to create the Center for Innovation in Health Care Logistics, a new research center focused on improving health care delivery through information technology.
Wal-Mart is also working with leaders in business, government, labor and public policy on the "Better Health Care Together" coalition. The goal of the coalition is to assure that affordable, quality health care is accessible to all Americans by 2012
- Anchor Rising on in-store health clinics here.
- Anchor Rising trying to understand the emergency room crisis here.
- Anchor Rising on universal healthcare here and here.
- RI Future's disdain for all things Wal-Mart here and here.
April 18, 2007
United Healthcare Versus St. Joseph's and Our Lady of Fatima
I’m not commenting on the veracity of either side’s claims, as reported by Karen Lee Ziner in today’s Projo. I’m just pointing out that if United Healthcare decides to drop St. Joseph’s and Our Lady of Fatima hospitals from its provider network, the average United customer has no recourse, because of the way that health insurance is tied to employment. In a more rational system, people who didn’t like United's decision could walk away from United and buy their insurance elsewhere. However, since employment-based health insurance places consumers in the position of taking the one choice that's offered or taking nothing at all, United is free to make this decision without considering what its customers want.
OK, I will comment on one claim mentioned in the news item. This ratio does seem a bit out of whack…
At a news conference at Our Lady of Fatima, [St. Joseph Health Services president and CEO John Keimig] , “[United Healthcare] is the same company that earned over $5 billion in profits nationally last year. It is the same company that paid its CEO the staggering total of $124 million in compensation last year — an amount that is approximately 150 percent of the total annual payroll for all of the 2,000 employees here at St. Joseph Health Services …”If one insurance CEO getting paid the same amount as 2,000 hospital employees is a problem, the solution is to allow every individual Rhode Islander to seek insurance from companies that can provide the same coverage with less corporate overhead. Under the existing system, insurance companies can increase the price of their services far above their costs because consumers are not free to take their healthcare dollars to insurers who run their businesses more efficiently, i.e. to insurers able to charge lower rates for the same or better service and still make a profit. Break the link between insurance and employment, and you'll see insurers suddenly become a lot more accomodating towards individual consumers.
It should be noted, however, that if hospitals want to be less subject to the whims of insurers, they too need to become more friendly towards the individual consumer.
United Healthcare Versus St. Joseph's and Our Lady of Fatima
I’m not commenting on the veracity of either side’s claims, as reported by Karen Lee Ziner in today’s Projo. I’m just pointing out that if United Healthcare decides to drop St. Joseph’s and Our Lady of Fatima hospitals from its provider network, the average United customer has no recourse, because of the way that health insurance is tied to employment. In a more rational system, people who didn’t like United's decision could walk away from United and buy their insurance elsewhere. However, since employment-based health insurance places consumers in the position of taking the one choice that's offered or taking nothing at all, United is free to make this decision without considering what its customers want.
OK, I will comment on one claim mentioned in the news item. This ratio does seem a bit out of whack…
At a news conference at Our Lady of Fatima, [St. Joseph Health Services president and CEO John Keimig] , “[United Healthcare] is the same company that earned over $5 billion in profits nationally last year. It is the same company that paid its CEO the staggering total of $124 million in compensation last year — an amount that is approximately 150 percent of the total annual payroll for all of the 2,000 employees here at St. Joseph Health Services …”If one insurance CEO getting paid the same amount as 2,000 hospital employees is a problem, the solution is to allow every individual Rhode Islander to seek insurance from companies that can provide the same coverage with less corporate overhead. Under the existing system, insurance companies can increase the price of their services far above their costs because consumers are not free to take their healthcare dollars to insurers who run their businesses more efficiently, i.e. to insurers able to charge lower rates for the same or better service and still make a profit. Break the link between insurance and employment, and you'll see insurers suddenly become a lot more accomodating towards individual consumers.
It should be noted, however, that if hospitals want to be less subject to the whims of insurers, they too need to become more friendly towards the individual consumer.
April 9, 2007
"Anchor Babies" and RIte Care
Froma Harrop calls attention to the problem that "Anchor Babies" (some consider the term to be a perjorative, incidentally) pose for immigration reform and enforcement.
Pregnant women routinely arrive in the United States in time to give birth and thereby obtain Social Security numbers for their babies — and with them, permanent entrée into American society and the socio-economic benefits it offers. Once the American-born child turns 21, he or she can sponsor his or her parents and other relatives for citizenship.Meanwhile, RIte Care is now in the process of implementing more stringent, federal guidelines that seek to prevent illegal aliens from using the system. And although even legal citizens are having a hard time proving their citizenship so that they may participate in RIteCare, the program does cover all children, whether their parents are illegal or not, so long as the kids are U.S. citizens. This is exactly the sort of thing Harrop is talking about. Finally, while the President is currently beginning a new push for "comprehensive immigration reform," there is no discussion about fundamentally changing the citizenship equation as outlined by Harrop.Many illegal aliens already in this country make a point of having “anchor babies” that they hope will secure them a permanent status in the United States. During the recent immigration raid at the Michael Bianco factory, in New Bedford, a number of the arrested women who had American-born children were allowed to return to the community, while the childless workers were kept in detention centers.
Changing the law will not be easy. The guarantee of citizenship to any child born on U.S. soil is in a 1952 immigration act and the 14th Amendment to the Constitution, ratified in 1868. When Rep. Brian Bilbray (R.-Calif.) first introduced legislation to change the law, in 1995, stopping the anchor-baby phenomenon was considered radical.
Since then, however, our broken immigration system has made the concept more mainstream. Very few countries offer this automatic citizenship. Even France has been tightening up.
Ending the citizenship birthright need not affect any future measures to grant amnesty to illegal immigrants. What it would do is end another lure to come here illegally.
April 5, 2007
All is Not Fine with the Emergency Room Fine
I have to examine the numbers more carefully before commenting on the overall plan, but this part of Rhode Island’s new small business healthcare plan, as described by Felice J. Freyer in yesterday’s Projo, seems troubling…
You pay through the nose — $200 per visit — if you go to a hospital emergency room with a problem that does not lead to being admitted.Obviously the state is trying to discourage people from using emergency rooms for non-emergency care -- which may or may not be contributing to rising healthcare costs.
Yet at the same time, the state is also blocking alternative treatment facilities designed specifically for dealing with immediate but non-emergency care from opening in Rhode Island. Taken together, the policies seem to be designed to discourage people from seeking non-emergency care at all. I know that’s not the intent, but it’s the kind of stupid dysfunction you get when you try to manage individual human decision making through government planning.
And would anyone like to take a stab at explaining how charging people what is in essence a fine for using the emergency room helps to reduce costs? At first glance, the $200 surcharge seems more like a backdoor way to subsidize indigent care (those without insurance get still get emergency room treatment for free, right?) by grabbing money from families teetering on the edge of the middle class than it does a plan for real cost control.
All is Not Fine with the Emergency Room Fine
I have to examine the numbers more carefully before commenting on the overall plan, but this part of Rhode Island’s new small business healthcare plan, as described by Felice J. Freyer in yesterday’s Projo, seems troubling…
You pay through the nose — $200 per visit — if you go to a hospital emergency room with a problem that does not lead to being admitted.Obviously the state is trying to discourage people from using emergency rooms for non-emergency care -- which may or may not be contributing to rising healthcare costs.
Yet at the same time, the state is also blocking alternative treatment facilities designed specifically for dealing with immediate but non-emergency care from opening in Rhode Island. Taken together, the policies seem to be designed to discourage people from seeking non-emergency care at all. I know that’s not the intent, but it’s the kind of stupid dysfunction you get when you try to manage individual human decision making through government planning.
And would anyone like to take a stab at explaining how charging people what is in essence a fine for using the emergency room helps to reduce costs? At first glance, the $200 surcharge seems more like a backdoor way to subsidize indigent care (those without insurance get still get emergency room treatment for free, right?) by grabbing money from families teetering on the edge of the middle class than it does a plan for real cost control.
April 4, 2007
Maybe the Worst Healthcare Op-ed Ever
Lawrence Purtill’s education aid op-ed isn’t the only recent Projo op-ed guilty of trying to convince people that a contradictory set of recommendations can be combined into sound public policy. In last Thursday’s Projo, Dr. Joseph Chazan presented this dud of a suggestion for containing healthcare costs in Rhode Island…
Government controls and regulators should recruit new insurance companies to enter and compete in the marketplace and mandate that everyone receives needed care regardless of ability to pay as part of the cost of doing business.I really don’t think that “Use your gains in other states to subsidize big operating losses in Rhode Island” can become the basis of a successful recruiting campaign. How exactly can you recruit companies to come to Rhode Island while demanding that they give their product away for free or below cost? What precisely are the “recruiters” supposed to pitch as the advantage of doing business here?
Dr. Chazan’s attitude towards individuals is even more frightening than his attitude towards business…
Recognize that individuals demand all the advances that have occurred in medical technology and prescription medications without concern for their costs. It is unlikely that health-care costs can be contained without some limitation or rationing of services. However, this will require a frank debate and the acceptance that to contain costs, not every patient can receive every available service.Translation: "People have a survival instinct and want to live, so government must teach them to manage and suppress that instinct". That's not a business that government should be getting into.
Before we start talking about giving government regulators, who have have a difficult time controlling costs without killing whatever economic sector they are trying to regulate, absolute power to decide who gets treatment and who doesn’t, shouldn’t we at least give an expansion of consumer-driven health plans a chance? After all, as another of Dr. Chazan's recommendations explains (quite inadvertently), consumer driven plans are the best fit for a pluralistic, democratic society like the US…
Finally, permit a robust, honest, forthright, uncensored debate to occur among parties: government, regulators, providers, insurers and consumers included.Dr. Chazan has the right principle in mind here, but what he and other advocates of a government takeover of healthcare never seem to grasp is that people need real choices if a robust, honest, forthright, uncensored debate is to matter. When individuals have a choice of healthcare options, they will talk to potential insurers and talk to their healthcare providers. That talk will have real ramifications, in terms of compromises on costs and on coverages and treatments offered. How can debate get any more robust than this?
Unfortunately, because of our employer-based system of health insurance, that debate is too restricted now because (save for a few forward-thinking companies like this one) employers have a big voice in the healthcare debate, but employees have almost none. And in strong-government schemes, the problem will become even worse, as government regulators, big-insurance companies, and well-organized special interests will become the only voices that matter, freezing ordinary people completely out of the debate.
Finally, Dr. Chazan reminds us that just because you think you're debating doesn't mean that you're making sense…
About 20 years ago, Rhode Island had one of the most regulated and controlled health-care systems in America. State laws required the Health Services Council and the head of the state Department of Health to approve the opening of virtually any new health-care facility (“certificate of need”). That sustained the status quo by delaying or preventing competitive facilities from operating but failed to control increasing costs.Er, why should anyone be surprised that heavy regulation in order to reduce supply led to increased costs?
Maybe the Worst Healthcare Op-ed Ever
Lawrence Purtill’s education aid op-ed isn’t the only recent Projo op-ed guilty of trying to convince people that a contradictory set of recommendations can be combined into sound public policy. In last Thursday’s Projo, Dr. Joseph Chazan presented this dud of a suggestion for containing healthcare costs in Rhode Island…
Government controls and regulators should recruit new insurance companies to enter and compete in the marketplace and mandate that everyone receives needed care regardless of ability to pay as part of the cost of doing business.I really don’t think that “Use your gains in other states to subsidize big operating losses in Rhode Island” can become the basis of a successful recruiting campaign. How exactly can you recruit companies to come to Rhode Island while demanding that they give their product away for free or below cost? What precisely are the “recruiters” supposed to pitch as the advantage of doing business here?
Dr. Chazan’s attitude towards individuals is even more frightening than his attitude towards business…
Recognize that individuals demand all the advances that have occurred in medical technology and prescription medications without concern for their costs. It is unlikely that health-care costs can be contained without some limitation or rationing of services. However, this will require a frank debate and the acceptance that to contain costs, not every patient can receive every available service.Translation: "People have a survival instinct and want to live, so government must teach them to manage and suppress that instinct". That's not a business that government should be getting into.
Before we start talking about giving government regulators, who have have a difficult time controlling costs without killing whatever economic sector they are trying to regulate, absolute power to decide who gets treatment and who doesn’t, shouldn’t we at least give an expansion of consumer-driven health plans a chance? After all, as another of Dr. Chazan's recommendations explains (quite inadvertently), consumer driven plans are the best fit for a pluralistic, democratic society like the US…
Finally, permit a robust, honest, forthright, uncensored debate to occur among parties: government, regulators, providers, insurers and consumers included.Dr. Chazan has the right principle in mind here, but what he and other advocates of a government takeover of healthcare never seem to grasp is that people need real choices if a robust, honest, forthright, uncensored debate is to matter. When individuals have a choice of healthcare options, they will talk to potential insurers and talk to their healthcare providers. That talk will have real ramifications, in terms of compromises on costs and on coverages and treatments offered. How can debate get any more robust than this?
Unfortunately, because of our employer-based system of health insurance, that debate is too restricted now because (save for a few forward-thinking companies like this one) employers have a big voice in the healthcare debate, but employees have almost none. And in strong-government schemes, the problem will become even worse, as government regulators, big-insurance companies, and well-organized special interests will become the only voices that matter, freezing ordinary people completely out of the debate.
Finally, Dr. Chazan reminds us that just because you think you're debating doesn't mean that you're making sense…
About 20 years ago, Rhode Island had one of the most regulated and controlled health-care systems in America. State laws required the Health Services Council and the head of the state Department of Health to approve the opening of virtually any new health-care facility (“certificate of need”). That sustained the status quo by delaying or preventing competitive facilities from operating but failed to control increasing costs.Er, why should anyone be surprised that heavy regulation in order to reduce supply led to increased costs?
March 29, 2007
Re: Senator Tom Coburn’s Healthcare Reform Plan
The inclusion of this item in Senator Tom Coburn’s national healthcare proposal…
Keeping Medicaid on mission: The bill liberates the poor from substandard government care and offers states the option to provide their Medicaid beneficiaries the kind of health care coverage that wealthier Americans enjoy. The bill creates incentives for states to achieve private universal coverage for their population. The bill offers states the freedom to design the programs that serve their beneficiaries with the best care instead of the current, one-size-fits-all straitjacket.…led commenter “mrh” to ask what “liberat[ing] the poor from substandard government care” meant.
John O’Shea of the Heritage Foundation provides the beginning of an answer…
In spite of Medicaid's hefty price tag, Medicaid patients find it difficult to access the health care system. Medicaid payment rates are considerably lower than physician payment rates under private insurance or even Medicare, in which physician payment is a recurrent problem. This has deterred physician participation in Medicaid. According to a 2003 Medicare Payment Advisory Commission (MEDPAC) study, only 69.5 percent of physicians surveyed were willing to accept new Medicaid patients, substantially fewer than the number willing to accept new privately insured patients (99.3 percent), Medicare patients (95.9 percent), and even the uninsured (92.8 percent)....Plenty of references available in the original memo.Once Medicaid beneficiaries gain access to the health care system, they receive inferior quality of care compared to patients with private insurance.
For example, patients with non-ST segment elevation acute coronary syndromes (NSTSE ACS), a form of heart attack, benefit significantly from innovative therapeutic approaches, including early invasive management strategies. These measures have now been incorporated into the guidelines of the American College of Cardiology and the American Heart Association. According to a study in the Annals of Internal Medicine, however, Medicaid patients with NSTSE ACS were less likely to receive evidence-based therapies and had worse outcomes (including increased mortality rates) than patients who had private insurance as the primary payer. This study found that these differences in care and outcomes persisted after adjusting for clinical characteristics (associated illness), socioeconomic factors (education and income), and the type of center where patients received treatment. In other words, the most important predictor of treatment and outcome in the study was whether the patient had Medicaid or private insurance.
March 27, 2007
Senator Tom Coburn’s Healthcare Reform Plan
Senator Tom Coburn of Oklahoma has introduced major healthcare reform legislation into the U.S. Senate. Kimberley Strassel had a short summary of the proposal in last week’s OpinionJournal…
[Senator Coburn's proposal] would remove the subsidy corporations get for health care, and instead give the money to individuals--putting them in charge of their health expenditures. It would expand HSAs, and allow consumers to buy insurance from any state, thereby avoiding costly regulations. It would modernize Medicare, allowing workers to invest their payroll taxes into a savings account and control their care in their retirement years. It would free up the states to inject Medicaid with new flexibility and competition.Senator Coburn’s website has a more detailed summary…
Promoting prevention: The legislation will reform our rudderless and wasteful federal prevention programs and demand results and accountability. Five preventable chronic diseases – heart disease, cancer, stroke, chronic obstructive pulmonary disease, and diabetes – cause two-thirds of American deaths. Seventy five percent of total health expenditures are spent to treat these largely preventable chronic diseases. A sound prevention strategy will save countless lives and billions of dollars.MediChoice tax rebates that will shift tax breaks away from businesses to individuals: Giving Americans a rebate check ($2,000 for individuals and $5,000 for families) to buy their own insurance will foster competition, improve quality and drive down prices. This provision will help put individuals back in charge of the health care, and help restore the doctor-patient relationship that has been severed by third-party government and health insurance bureaucrats.
Creation of a national market for health insurance: The bill would give Americans the right to shop for health insurance anywhere in America. Patients should not be forced to be pay for outrageously expensive health plans in states like New Jersey when they can save thousands by buying plans from companies in other states.
Creating transparency of health care costs and services: This Act requires hospitals and providers receiving reimbursements from Medicare to disclose their estimated and actual charges for all patients as well as the rates they are reimbursed through Medicare and Medicaid. This provision could allow patients to “Google” their doctor and comparison-shop for health care the way that they do for cars, computers, or other products and services.
Securing Medicare’s future by increasing choice and encouraging savings: The bill retains existing benefits but encourages true competition among private plans to hold down costs, a model already is working in Medicare’s prescription drug benefit. The plan would give Medicare recipients similar health care options available to Members of Congress and employees of Fortune 500 companies.
Keeping Medicaid on mission: The bill liberates the poor from substandard government care and offers states the option to provide their Medicaid beneficiaries the kind of health care coverage that wealthier Americans enjoy. The bill creates incentives for states to achieve private universal coverage for their population. The bill offers states the freedom to design the programs that serve their beneficiaries with the best care instead of the current, one-size-fits-all straitjacket.
March 23, 2007
If Emergency Room Overuse is Really a Problem, Why Aren't MinuteClinics Being Allowed?
For a while now, I have been hearing that the inefficient delivery of routine healthcare, especially through the over-use of emergency rooms, is a primary source of America's runaway healthcare costs. If this is true, CVS’ proposal to place “MinuteClinics”, staffed by a nurse practitioner, in a number of their stores, should at least an incrementally improve the existing healthcare system. Felice J. Freyer of the Projo described “MinuteClinics” in a Projo article from last year…
Say you've got a sore throat and you've heard that strep is going around. You're really busy at the office and want a quick answer on your health.Of course with this being Rhode Island and “MinuteClinics” being different from the established way of doing business in the state, there is an organized movement afoot to stop them from ever beginning operation here.Then imagine you could just stop at the drugstore, where within minutes a nurse practitioner could give you a strep test -- and, if it's positive, a prescription for antibiotics. Which you could then buy at the selfsame drugstore.
Such convenience has obvious appeal for consumers.
Allen Dennison, chairman of the Urgent Access Committee of Rhode Island Primary Care, had an op-ed in Sunday’s Projo arguing that Rhode Islanders already have access to all the urgent healthcare services they need. If they want improved access and convenience, well, they’re wrong to…
As to the issue of consumer convenience, the concept of the Urgent Care Center first arose in Rhode Island in 1975. According to the Web site of the Urgent Care Association of Rhode Island (urgentcareri.com) there are 20 Urgent Care Centers in Rhode Island, at most a 15-minute drive from anywhere in the state. Also, around the state, there are five Walk In Clinics that offer similar if simpler facilities with extended hours for the working sick who can’t get an appointment with their primary-care practice.Five clinics with “extended hours” for a state with a million people. How dare Rhode Islanders think they might need anything more!
The immediate question that arises from this is why anyone in any business should be allowed to shut down a competing practice because it might attract people through increased convenience and better access. The fact that CVS thinks there's a market for MinuteClinics in Rhode Island implies that people will choose a facility other than an emergency room for simple medical needs, when another choice is readily available. Maybe there are problems with opening a clinic inside of a drugstore (what's the plan, for instance, for dealing with someone who thinks they can get a prescription for OxyContin right away, and is disappointed to find out that they can't?), but if Dr. Dennison really wants to help doctors and patients, shouldn't he be looking for ways to improve access to existing non-ER facilities, rather than shutting down any new alternative facilities before they open?
Having said all this, in a precise economic sense, I'm still not sold on the idea that emergency room overuse is a true driver of rising healthcare costs. Dr. Dennison bolsters my skepticism, when he admits that Doctors over-charge for simple procedures in order to subsidize other parts of their practice...
To put it frankly, simple visits make us money. The work required by the time-consuming complex patient, on the other hand, is poorly reimbursed by Blue Cross, United Health Care and Medicare.I suspect, as Megan McArdle has suggested, that hospitals do the same thing: over-charge patients with simple problems and lots of insurance in order to subsidize uninsured patients and more complex cases. If so, then emergency room usage isn't really raising the cost of healthcare, it's only raising its price -- for those who are actually paying for it. A more rational insurance system than exists now, one that allows more people to participate by offering a range health savings accounts plus high deductible plans, is the needed beginning to more fairly allocating the costs of healthcare to patients who seek treatment.
Anyway, if Rhode Island politics plays out as usual, expect the lobbyists on Dr. Dennison's side to win, MinuteClinics to be stopped from entering RI, prices to continue to be inflated, urgent care access outside of emergency rooms to continue to be limited, and maybe the MinuteClinic system to eventually open branches in Attleboro and Seekonk.
March 21, 2007
Teaching Moment of the Week #1: United Healthcare’s Profit Transfer
According to Felice J. Freyer in today’s Projo, just about everyone in Rhode Island not on the United Healthcare payroll, including most of the state’s healthcare providers, Attorney General Patrick Lynch, and Governor Donald Carcieri, opposes United’s attempt to transfer $36.8 million from RI to their parent company in Minnesota...
United is seeking state permission to take out $36.8 million in “extraordinary dividends” — profits beyond the “ordinary” profits already taken. Although such permission has long been required, this year United’s request is being considered by the Office of the Health Insurance Commissioner and the Health Insurance Advisory Council, both created by a 2004 law....Consider this story carefully, because it is a perfect illustration of how the healthcare mess faced by our country is NOT the result of impersonal and unstoppable macroeconomic forces, but of a strange system of government regulation maintained in this country out of inertia and not because it serves any public good.An extraordinary dividend is defined as profits that exceed either 10 percent of the insurer’s surplus or the net income from the insurer’s operations in the previous year. Long-standing law requires insurers to win state permission for such dividends, but never before has the state sought public input on such a request.
Here’s what I mean. Current insurance laws, obviously, allow health insurers to conduct their business across state lines. Yet for individuals, similar activity is forbidden; individuals are restricted to their home states when spending money on health insurance. The restriction is not the result of any iron laws economic of necessity, but of political decisions made by the government.
If corporations have been given the freedom to pick and choose which states provide the best environment for the use of their resources, then why shouldn’t regular people be given the same freedom and be allowed to “transfer” a few thousand dollars to another state in order to buy a health insurance policy, if they can find a company in another state that better meets their needs? What legitimate purpose does the existing regulatory asymmetry between corporations and individuals serve?
March 16, 2007
Promoting New Healthcare Ideas in South Kingstown
Liz Boardman has a report in this week's South County Independent on a presentation given to the South Kingstown Republican Town Committee by Sean O’Donnell and Roland Benjamin on “Consumer Driven Health Plans”, i.e. health savings accounts combined with high-deductible insurance. Ms. Boardman provides a straightforward example of how CDHPs work…
Under CDHPs, employees put pre-tax dollars into a special savings account. Their employers match at least a portion of that amount. The employee uses the money to pay a relatively higher deductible, but any costs above that are fully covered by the plan.Among other benefits, South Kingstown Republican Town Chairman Dave Cote sees CHDPs as a possible way of relieving the fiscal crunch on Rhode Island’s cities and towns…For example, an employee with a $2,000 deductible would contribute $1,000, and his employer would add the other $1,000. If the employee has a chronic illness, such as asthma, he would likely spend his $2,000 on maintenance drugs and doctor’s visits, but he would cap out after $2,000 and not pay any additional costs…
Using a CDHP system, Benjamin told the group, LFI was able to hold the cost of health insurance steady after several years of near double-digit increases with traditional plans.
Coté said the GOP would be holding workshops about CDHPs around South Kingstown and statewide. “The end result, we hope, would be the students benefiting by infusing the savings back into school programs and extracurricular activities, like languages, sports and gifted programs,” he said.
February 22, 2007
Motivations for Employer Based Healthcare
I’ll admit to being surprised by the spirited defense of employment-based healthcare offered by commenters on this blog and in a few face-to-face discussions I’ve had. Mark Schmitt, writing just yesterday on the American Prospect’s weblog, adds an angle to this discussion not yet mentioned here, suggesting that many people prefer employer-based health insurance for the simple reason that they don't want the responsibility of choosing a health plan on their own…
On the other hand, an immediate transition to an individualized system seems unrealistic, and also politically dangerous. Not only do you have to give up the dollars that employers are putting in, but you also lose their role in helping to navigate the choices in the system (as Bruce Vladek, former head of HCFA, once pointed out, people may say they want choices but they really want somebody in HR to tell them what to do)…There is also a more extreme view, expressed by Lord Douglas Jay, a member of the British Parliament in the 1940s. Lord Jay’s sentiment is rarely expressed in direct fashion today, but almost certainly exists in the minds of some healthcare reformers…
Housewives on the whole cannot be trusted to buy all the right things where nutrition and health care are concerned. This is really no more an extension of the principle according to which the housewife herself would not trust a child of 4 to select the week’s purchases. For in the case of nutrition and health, just as in the case of education, the gentleman in Whitehall really does know better what is good for the people than the people know themselves.(Original quote taken from David Gratzer’s The Cure: How Capitalism Can Save American Health Care).{Note from the blogger: Americanizing the end of the last sentence would translate to something like “the Department of Health and Human Services really does know better what is good for the people than the people know themselves.”}
Whether it’s Mr. Schmitt’s soft view (people want someone else to make their insurance decisions for them), or Lord Jay’s harder one (people need someone else to make their insurance decisions for them), the implication is the same -- the debate about employer-based healthcare is more than a debate about economic factors, it is also a debate about government co-opting corporate bureaucracies in an attempt to engineer better lives for individuals.
Is Mark Schmitt right? Do people support the employer-based system because, at some level, they want someone to help them choose their coverage, and not just because they are afraid that the employer-based healthcare system is the only non-directly government run system that can provide them with affordable coverage?
People who believe there’s a better way to provide insurance than through the existing system need to know the answer to this question, so they will know if they need to make the case for a more open insurance market in terms broader than just fiscal and economic viability.
February 19, 2007
The Stop & Shop Strike: Important, Yet Just a Distraction
The issues in the looming Stop & Shop strike are all too familiar, centering on health benefits and retirement benefits. From Gregory Smith and Talia Buford in today’s Projo…
[Stop & Shop], based in Quincy, Mass., wants union workers to contribute to their health-care premiums and allow it to switch from an employer-paid pension fund to a 401(k) plan for new employees. [Union Official Jim Riley] said the employees would be willing to help pay the premiums if their health-care plan is improved.The big insurance companies must either sit back and laugh, or maybe just breathe a sigh of relief when they read a story like this, thankful that America’s employment based system of health insurance allows them to raise rates without improving the quality of their product, while deflecting all of the blame on to employers.
Stop & Shop is not responsible for rising healthcare costs. Insurer decisions beyond Stop & Shop (or any employer's) control, motivated by over-regulation state mandates, are responsible for that. Neither are Stop & Shop employees unreasonable in objecting to being charged more for the same coverage. When insurance companies want to charge higher prices for the same product, consumers should have the right to do what they would do with any other type of product -- to look for a better deal from a different supplier and to take their business there when they find one. Stop & Shop employees don’t have that option. Because of the way that insurance law is structured, most employees of Rhode Island businesses don’t. We’re all locked into a single, employer-provided option for health insurance and told “take it or get nothing at all”.
Stop & Shop’s management didn’t create the system that binds health insurance to employment, they are just trying to get along within it. That system, and not Stop & Shop's little corner of it, is what needs changing. State mandates should be relaxed, so that cheaper insurance policies are available. People should be given the option of high-deductible insurance plans and tax-free HSAs to cover their routine, recurring expenses. And individuals should be given the option of purchasing their health insurance from states where coverage is cheaper. These reforms could be combined in a way that would allow people to address their personal, medical needs without consulting with their employers.
If these options were available, many Stop & Shop employees would be able to find an affordable health plan that suited them. Some might even see an increase in their take-home pay. And, as an additional benefit, we would skip over a whole lot of labor strife that does very little to resolve the heart of the healthcare issue, by taking employers out of a role they don't want anyway as middlemen between individuals and insurers.
Will we ever see any interest from the left in the kinds of health insurance reforms that empower indivdual employees? Or are the forces in government and politics who should be labor’s allies more interested in managing the lives of employees, maybe even in just using them as a pathway to political power, than they are in giving those employees the tools they need to make their lives better?
February 14, 2007
A Prankster in the RI Senate?
 I truly want to know the motivation behind proposed legislation such as this:
I truly want to know the motivation behind proposed legislation such as this:
Sen. John C. Revens Jr. (D-Dist. 31, Warwick) has introduced legislation that would extend private health insurance coverage to dependents up to the age of 25.The legislation, (2007 - S0327), targets individuals between the ages of 19 and 25 who are financially dependent but who are not in school full time. Under current law, insurers are only required to continue coverage for this age group if they are enrolled full time in school or have chronic disabling conditions.
“Allowing insurers to stop providing coverage for individuals in this age group can be potentially devastating, medically and financially, for these people and their supporting parents,” said Senator Revens. “We all know the enormous price of supplemental health insurance coverage, which makes it impractical for most, and the other temporary catastrophic programs don’t pay for doctor visits or pharmaceuticals these 19- to 25-year-olds might need.”
Is it naive dogooderism? Is it cynical vote buying? Is it backroom backrubbing? Is it self-interest? Or is it merely a practical joke? Because it seems to me that Rhode Islanders' representatives should be personally embarrassed and politically frightened to offer such bills.
As is a recurring theme in Rhode Island government, there appears to be an assumption that the targeted parties — in this case, insurance companies — will simply eat the additional costs resulting from legislation. They won't. They'll pass the cost on to payers — whether that means the taxpayers who fund RI's lavish public sector benefits or the businesses that supply health insurance to their employees — probably by increasing family plans across the board.
Although this might be news to those who've lived on the public dime their whole lives, in the private sector, businesses often pass additional family-plan costs directly on to their employees. Those companies that do cover employees' family plans will either cease to do so or find other areas of payroll/benefits in which to make up for the increased expenses. Whatever the case — and as is, again, a recurring theme in Rhode Island government — the upshot is that families struggling to get by in the leech-filled Ocean State, without public-union-bullied benefits or In Crowd largesse — will be the ones who bear the burden of ensuring that indolent young adults needn't worry about paying full price for prescription fungicides.
In fact, the only rational basis that I can see for such a policy in Rhode Island is to create financial incentive for those young adults who are not indolent, but motivated and unable to support themselves in this state, from seeking opportunities elsewhere. But they'll leave eventually, Sen. Revens. Why don't we just pass legislation to encourage a healthier state economy?
ADDENDUM:
Here's a project for folks with more time to indulge in hypotheticals than I possess: What would be the cost to RI taxpayers if a married family with three 19–25 year old children all had public-sector jobs and piled their health insurance onto one plan, taking buyouts for the other four?
February 12, 2007
Ron Wyden Likes George W. Bush's Healthcare Proposal
Senator Ron Wyden (Democrat from Oregon), a Senator with a creative healthcare plan of his own, wants to compromise and combine his proposal with President Bush's healthcare proposal. Michael Barone of U.S. News and World Report has the details…
Bush's proposal in a nutshell is to end the preferential tax treatment for employer-provided health insurance....This decision has saddled us with a system in which health insurance has been tied to employment, with many perverse results. Healthcare is perceived as a free good, and consumers have no incentive to take costs into account....For conservatives and libertarians who may be turned off by the “universal coverage” part of the compromise, keep in mind that reasonable universal coverage schemes can be devised, if the goal is truly to provide insurance against major illnesses. It’s attempts by liberals, technocrats, and all-around demagogues to engineer a massive redistribution of wealth through the insurance system that creates problems, like big middle class tax increases that do nothing to improve the quality of care that taxpayers receive.The biggest beneficiaries of the current system are high earners with employer-provided insurance. The biggest losers in the current system are low earners without employer-provided insurance. Health insurance experts on the left, right, and center have long called for ending the tax code's preference for employer-provided health insurance. But employers haven't wanted to lose the deduction, and politicians have flinched at the prospect of taxing voters on something they have been getting tax free. Bush has found a way out, by equalizing the tax treatment of health insurance wherever it comes from....
[Senator Wyden] notes that we don't have employer-provided auto insurance; we buy that out of after-tax earnings. He argues that people should be able to buy health insurance as members of Congress and federal employees do, from an array of choices offered by private insurers. He's looking to make something of a political deal [with President Bush]. Republicans would get Bush's standard deduction and a private insurance market in which consumers would have incentives to hold down costs. In return, Democrats would get universal coverage, with subsidies for low earners to pay for coverage. As John Goodman of the free market National Center for Policy Analysis points out, additional revenues from those with policies worth more than $15,000 could be used to subsidize low earners.
It’s not clear from Barone’s article exactly what universal coverage scheme that Senator Wyden envisions as part of a compromise, but if its based on his original plan, it will lean more towards a mandate that individuals buy some kinds of insurance from the existing system than it will towards a single payer, total government takeover of healthcare.
One other note: John Edwards, who is especially relevant to this debate for reasons I won’t expound upon, has positioned himself as the leading advocate for preserving the employer-based healthcare system.
Details on the Bush plan available here.
Details on the Wyden plan available here.
How would you mix and match?
January 24, 2007
President Bush's Healthcare Plan
President Bush outlined a serious healthcare reform plan in last night's State of the Union. The President's plan is to replace the existing tax-exemption that applies only to money spent on employer-sponsored health insurance with a standard deduction that can be taken by any individual who purchases health insurance, regardless of employer or employment status.
1. Assuming the size of the deductions is reasonable, opposing this plan tantamount to saying "I oppose tax-breaks for individuals; tax-breaks should only be given to big corporations". And yet we will surely see this reaction from the usually anti-business left. In fact, we already do.
If libs can get past their knee-jerk "if Bush is for it, I'm against it" response to the entire universe, they will see that this plan addresses many of their complaints about Wal-Mart not providing insurance to enough of its employees. Under the Bush plan, for example, companies lose financial incentive to hire lots of part-time workers to avoid paying health benefits.
Arnold Kling of the Cato Institute systematically sums up and counters liberal reactions he has observed to the President's plan (h/t Instapundit)...
Since the President's plan was leaked, I have seen three complaints from the left.2. However, the biggest challenge to the President's proposal may not come from organized liberal shrieking, but from misunderstanding at America's apolitical center. Under the current system, employers do little more than choose the health plans that their employees will be allowed to spend their own salaries on. In spite of this, many individuals enrolled in employer-sponsored health plans are convinced that their employers are "giving" them something for nothing. When they hear about tax-code changes that will end the special status of employer based coverage, they will feel that the government is trying to take something away from them -- even though most will be able to to purchase same amount coverage with the same amount of money via an individual plan. Overcoming this perception will be one of the toughest challenges faced by Bush plan supporters.In my view (2) and (3) are positive developments....As for (1), I fail to see the cause for alarm. Consider the status quo. An economist on the faculty at Princeton who receives generous health benefits from the University is able to enjoy them tax-free. So can the professor's secretary. But, as with all tax breaks, there is a vertical inequity -- the professor derives more benefit from the tax break than does the secretary. But today there is a horizontal inequity as well. A self-employed economist and a self-employed secretary get no tax break for obtaining comprehensive health insurance.
- The tax break benefits the rich more than the poor.
- The tax break encourages people to leave employer-provided health plans and instead get health insurance on their own.
- The proposals encourage catastrophic health insurance rather than insulation.
Now, if the President's proposal is enacted, the self-employed economist and the self-employed secretary will get a tax break....
My sense is that the hard left is going to dig in against the President's proposals. Too bad for the millions of people for whom health insurance is more expensive simply because where they work falls outside the corporate umbrella.
3. To really make the Bush plan work, people must be allowed to buy insurance across state lines. Today's OpinionJournal article on the President's plan mentions that "the average employer-sponsored family plan runs about $11,500 annually". Even for someone in the top tax-bracket, a $15,000 deduction would pay for less than half of a $11,500 plan. But the $11,500 figure averages together nsurance costs in high-regulation, high-cost states (like Rhode Island) with insurance costs in low-regulation, low-cost states (like Idaho).
I poked around the "ehealthinsurance" website (as suggested by Anchor Rising commenter Emily Harding) and found that in some states, high-deductible insurance plans are available for a family of four in the range of $2,500 - $4,000. If people are given the freedom to escape from legislative mandates that drive the cost of insurance up, they should be able to find affordable coverage with the numbers the President is using.
4. Barack Obama was wrong in his post-SOTU interview with Charlie Gibson of ABC when he said there are no cost-controls in the President's plan (no link available). The cost-controls come from introducing transparency and choice into medical care, both of which are currently lacking in a system where an employer hands you a very complex health plan and tells you to "take it or leave it". Could Obama be confusing "cost controls" with "price controls"?
5. 'Tis not all praise I have for President Bush for proposing this plan. Here's my criticism: Why didn't he propose something like this when his party controlled both houses of Congress?
January 18, 2007
The Reform of the Veterans Administration Hospital System is Not the Great Example of Government-Controlled Healthcare That Liberals Think It Is
I've seen a few blogospheric comments touting the reform of the Veteran’s Administration hospital system as an example of how strong government involvement in healthcare, maybe as strong as single payer, works well. The example doesn’t work for a very simple reason, illustrated below.
An article from the July 17 issue of Business Week does provide several metrics proving pretty conclusively that (high) quality patient care is available from the VA hospital system…
According to a Rand Corp. study, the VA system provides two-thirds of the care recommended by such standards bodies as the Agency for Healthcare Research & Quality. Far from perfect, granted -- but the nation's private-sector hospitals provide only 50%. And while studies show that 3% to 8% of the nation's prescriptions are filled erroneously, the VA's prescription accuracy rate is greater than 99.997%, a level most hospitals only dream about. That's largely because the VA has by far the most advanced computerized medical-records system in the U.S. And for the past six years the VA has outranked private-sector hospitals on patient satisfaction in an annual consumer survey conducted by the National Quality Research Center at the University of Michigan. This keeps happening despite the fact that the VA spends an average of $5,000 per patient, vs. the national average of $6,300.Of course it wasn’t always this way. As Business Week reminds us…
To much of the public… the VA's image is hobbled by its inglorious past. For decades the VA was the health-care system of last resort. The movies Coming Home (1978), Born on the Fourth of July (1989), and Article 99 (1992) immortalized VA hospitals as festering sinkholes of substandard care. The filmmakers didn't exaggerate. In an infamous incident in 1992, the bodies of two patients were found on the grounds of a VA hospital in Virginia months after they had gone missing. The huge system had deteriorated so badly by the early '90s that Congress considered disbanding it.So how was the system turned around? In the mid-1990s, a VA administrator by the name of Kenneth Kizer (a Clinton appointee, for those keeping score) implemented a broad-based series of reforms...
The VA was reinvented in every way possible. In the mid-1990s, Dr. Kenneth W. Kizer, then the VA's Health Under Secretary, installed the most extensive electronic medical-records system in the U.S. Kizer also decentralized decision-making, closed underused hospitals, reallocated resources, and most critically, instituted a culture of accountability and quality measurements. "Our whole motivation was to make the system work for the patient," says Kizer, now director of the National Quality Forum, a nonprofit dedicated to improving health care. "We did a top-to-bottom makeover with that goal always in mind."And what is Dr. Kizer doing now, to continue make the system even better and build on his successes? The answer is nothing. After fixing the VA system, Dr. Kenneth Kizer was fired by Congress for not doling out enough pork projects to key legislators…
Kizer, the turnaround's architect, was forced out in 1999 when Congress refused to reconfirm him after he closed hospitals in key districts.Government Executive Online has more detail on Dr. Kizer's firing (technically, the Senate's decision not to renew his appointment; those who want to blame Republican Senators for opposing a Clinton nominee, get ready for a big disappointment)…
VHA also reflected another change in veteran demographics: the shift in population from North and East to South and West. Kizer's response was a resource redistribution plan called the Veteran's Equitable Resource Allocation (VERA) system. The system distributes operating funds among the agency's networks based on the number of veterans served. In its first year, VERA caused nine VISNs to lose some 1998 funding, while 13 gained. For example, VISN 3, in New York, lost $124 million, while VISN 18, in Phoenix, gained nearly $60 million.There wasn’t anything magical about “single-payer” that made the VA system work. Dr Kizer's reforms could be implemented in the existing hospital/insurance system (with an important exception or two, one of which is noted below), if there was a will to do so. The magic was that, for a little while, the top-priority -- the only priority -- in allocating resources in the VA system was quality of care. Unfortunately, as the VA is a government system, a systemic focus on regular people couldn't last. In fact, a focus on reform of patient care, instead of on the politically motivated redistribution of resources, could cost a successful administrator his job.VHA's shifts in focus and resources brought results. Staffing fell 11 percent between December 1994 and September 1998, while the number of patients treated per year rose 18 percent. Surgeries performed on an outpatient basis - increasing productivity and reducing deaths - rose from 35 percent of all surgeries to 75 percent from September 1995 to March 1998....
So Kizer is a hero, and VHA has been rewarded, right? Not in Washington.
In fact, after failing to win renomination in September 1998, at the end of his four-year term, and again in June 1999, at the end of a nine-month extension granted by Congress, Kizer withdrew from contention. By June, Kizer's VHA reforms had so angered legislators that they were lining up to threaten to place holds on his nomination if it ever escaped from committee.
Many legislators apparently couldn't stomach the process Kizer used to transform VHA into a patient-centered, effective and efficient health care system. Sen. Ben Nighthorse Campbell, R-Colo., repeatedly took Kizer to task for considering closure of the nursing home and outpatient clinic at Fort Lyon, Colo., a location so remote that the VA facilities there must run their own sewer system and fire department....
Meanwhile, Sen. John Kerry, D-Mass., threatened to hold up Kizer's nomination because of hospital cutbacks in his state, which has seen reductions in veterans, and consequently in VA hospital beds and funding.
To be successful, hospitals need to be run by people who want to build successful hospitals, not by politicians who view the world as a giant jobs program and whose concern for the quality of care is secondary to their concern that some fat budget numbers exist that can be pointed to on election day, whether or not the money is being spent on quality healthcare. Healthcare in America will only become economical, rational, and just when people are free to choose the best doctors and hospitals available to them, free from undue interference from either the government, or from private insurance industry bureaucrats who have figured out how to manipulate the government.
One other note. The Business Week article also notes that one factor in the VA turnaround an immunity from some lawsuits tied to the VA's status as a government agency…
[VA] doctors don't have to worry as much about malpractice lawsuits, since government agencies are somewhat protected. That made it easier for the VA to go out on a limb in 2005 and institute a systemwide policy of apologizing to patients for medical errors -- an act of contrition rarely done in the private sector.Are those who look towards the VA as model of healthcare reform willing to explore extending the tort immunity enjoyed by the VA to non-government hospitals?
Healthcare: Appeals Court Agrees That “Fair Share” Plans are Not Legal Under Existing Law
It’s been a few months since I've written about it…
Yet it’s back in the news…
And it’s important, with impact on a major policy debate…
So humor me, and pretend that it’s an exciting topic…
With this introduction…
Loyal Anchor Rising readers will know…
That it can only be…
[Dramatic pause]…
[Unorthodoxly long dramatic pause now bordering on campy]….
ERISA -- The Employee Retirement Income Security Act of 1974!!!!
The Fourth Circuit Court of Appeals has upheld a July lower court ruling striking down Maryland’s “fair share” health coverage law as illegal under the aforementioned Federal ERISA law. Fair share laws are state mandates requiring large companies either to provide health insurance to their employees or pay an additional payroll tax used to fund a state-managed healthcare plan. The courts agreed (as they always have) that the ERISA statute prevents states from regulating employer-provided benefits – any benefits, healthcare included -- any more stringently than the Federal government does.
The strikedown of the Maryland law may have immediate consequences beyond Maryland, potentially ripping the heart out of Governor Arnold Schwarzenegger’s universal healthcare proposal for California. Without the tax on employers, the additional tax-increases on doctors and hospitals proposed in the California plan probably won’t be enough to pay for it. (By the way, I haven’t yet seen a satisfactory explanation of why ERISA doesn’t also doom Mitt Romney’s universal coverage plan for Massachusetts.)
In its coverage of the ruling, the New York Times mentions an interesting alternative to “fair share” laws that may have some cross-ideological appeal, because (at least in theory) it helps separate health care choices from employment…
Maryland lawmakers may also choose to rewrite the law, using an approach upheld in several other states that requires companies with uninsured workers to pay them higher wages that can be used for health care premiums, said Paul Sonn, deputy director of the Brennan Center for Justice at New York University School of Law and an expert on fair share health care legislation.I’d be interested to know if the law in these other states requires employers to pay their employees only what would have been spent on health insurance, of if it requires the pay increase to be enough to pay for an individual health insurance policy, which would be substantially larger. If the second case is true, then this is less a reform proposal than it is a backdoor attempt to force everyone into (and thus continue) America’s strange system of employment based health coverage. That would be a bad thing, as it would retard the building momentum for decoupling health insurance from the workplace.
January 3, 2007
Some Questions (Answered) About the Wyden Healthcare Plan
Kari Chisholm of “Stand Tall for America”, a web-based effort founded to promote Oregon Senator Ron Wyden’s universal healthcare plan, answers a few questions about the Wyden plan put forth by me in the comments section of the Virginia Progressive blog. (The Wyden Plan is a federal proposal different from the Rhode Island small business health insurance plan, a state-level proposal also introduced last month). My original questions are in bold. Mr. Chisholm's answers are in italics.
The Wyden Plan begins from the radically simple notion of decoupling health insurance from employment. For the first two years, Senator Wyden is proposing that employers increase the wages and salaries of their employees using monies originally allocated for the purchase of group health plans. Employees would use their pay increases to purchase individual health insurance policies. Changes in the tax code and insurance regulation would be enacted to make individual insurance purchases feasible. That's all good. However, after year two, Senator Wyden wants to begin paying for his system through a payroll-style tax. That's not so good. The post-year two payroll tax was the subject of my first question…
1. The plan, as I understand it from the Los Angeles Times summary, has people directly buying their own insurance in years 1 and 2. Why not keep with this system after year 2 and let people spend their own healthcare dollars (perhaps through a HSA) into the future? After taking employers mostly out of the mix for two years, what’s the motivation for shoehorning them back in?
People will buy their own insurance long after years 1 and 2. That’s the crux of the plan. Employers will be out - forever. After year 2, employers will pay a per-person contribution to the health care system - that roughly approximates to 25% of the cost of health care. This cuts the cost of health care for those responsible folks who have been paying for it until now; while getting a contribution from the cheapskates (Wal-Mart and friends.)
(Me again: But employers aren’t out if they are required to pay a new tax. This new tax means that after year two, most individuals will experience a sudden drop in the amount of healthcare they can afford per-hour of work. In years one and two, people will spend a certain percentage of their incomes on healthcare. After year two, across-the-board pay-cuts will be needed to pay for the new tax, even though healthcare costs will likely remain about the same. Workers won’t get as much healthcare per dollar collected by the government as they were getting per dollar paid to them directly because much of the new tax-stream will be going to subsidize healthcare for the poor. For most folks, a better solution than a payroll tax would be to allow tax-breaks for individuals and employers for monies paid into HSAs, and to allow individuals to take tax-breaks for purchasing high-deductible insurance.
Now, if you want to argue that we need a better subsidized healthcare system for the poor in this country, that is a perfectly legitimate argument, but it is a separate argument from how to provide health insurance to people that could afford it already, if not for the strange system of health insurance regulation that currently exists in America.
Continue reading "Some Questions (Answered) About the Wyden Healthcare Plan"December 19, 2006
The Rhode Island Small Business Healthcare Plan
In today’s Projo, Felice J. Freyer describes a new small business/individual health insurance blueprint unveiled yesterday by the Rhode Island Office of the Health Insurance Commissioner…
Blue Cross & Blue Shield of Rhode Island and UnitedHealthcare of New England are required, starting in May, to offer a “wellness health benefit plan” to individuals and businesses with 50 or fewer employees. The plan has to meet the state’s criteria and the average premium can’t exceed 10 percent of the average Rhode Island wage....The program's concepts are stunningly unoriginal, consisting of nothing more than…The new plan’s deductible will be about $500, with out-of-pocket costs capped at $3,000 — provided the enrollee signs a pledge promising to choose a primary-care physician, undergo a health-risk appraisal, either maintain a healthy weight or participate in weight-management programs, either remain smoke-free or participate in smoking cessation programs, and participate in disease-management programs if applicable. In the first year, subscribers will be asked just to promise these things; in the second year, they will have to prove participation.
Someone who didn’t want to sign such a pledge could still buy the plan but he or she would face a $3,000 deductible and out-of-pocket costs up to $6,000 a year.
- Price controls on the amount insurance companies can charge employees of small businesses, and
- Government regulation of individual behavior that will hopefully lead to individuals consuming less insurance.
Seriously, there are at least 3 problems with the plan…
- A fixed-price formula divorced from actual costs of providing healthcare could eventually drive health insurers out of the state. There is recent precedent for this. An irrational regulatory structure forced most workers’ compensation insurers to pull out of Rhode Island in the early 1990s because they were required to pay out more money than pricing regulations allowed them to collect. There is no reason that the same thing couldn't eventually happen to health insurance.
- The partcular mechanism for implementing the “wellness” program sets a dangerous precedent. It is wrong for government to use its power to demand that interaction between individuals occur only on the government's terms. It is not hard to imagine a future where, for example, attendance at the sex-education program of the government's choice, chosen with as much political input as medical input, is made a pre-requisite of getting lower insurance rates on a family plan. (I chose the sex-education example because liberals, conservatives and everyone in-between should be able to envision a potential problem here.)
- Finally, it will never make sense to pay for “wellness” programs through an insurance-type system. Insurance assumes that many people pay into a pool of money, while only a few take monies out to pay for unexpected emergencies. But usage of "wellness" care will not be occurring on an infrequent, emergency basis. Ideally, the wellness program will be utilized by many people at regular intervals. This means that paying for wellness care through an insurance program will be always be less cost-effective than paying doctors for wellness care directly, sans any middleman. (Of course, if people start paying their doctors directly, they will never develop a sense that their visits to a doctor are a government-provided entitlement, making the government seem a little less powerful, creating an impression that strong-government advocates would prefer to avoid.)
- Implementing some sort of community rating system, ala the Wyden plan, so people can buy insurance independent of their employer,
- Modifying the community rating system so that insurers can modify their rates based on certain types of behavior (participating in a wellness program, not smoking, etc.), and
- Creating health-savings accounts that people can use to pay for their routine and “wellness” care.
December 14, 2006
Senator Ron Wyden's Universal Health Coverage Plan
Senator Ron Wyden of Oregon has announced a universal health coverage plan that he intends to introduce in Congress next year. Here’s how the Los Angeles Times describes it…
Wyden's plan would require employers to continue contributing toward the cost of health coverage, but it would get them out the business of directly providing insurance and limit their exposure to double-digit annual inflation in healthcare costs.It sounds like free marketers and libertarians might actually be able to rally around the Wyden plan in years one and two. However, for some reason, after year two, Senator Wyden wants to stick employers back in between individuals and their health insurance…In the first two years of the plan, employers who now provide coverage would be required to directly pay workers what they were spending on insurance.
Thereafter, most companies would pay the government a healthcare contribution that resembles a payroll tax.If you can successfully decouple insurance from the workplace for two years, then why does it need to be recoupled at a later date? The payroll-tax provision sounds more like something intended to make the government’s tax collection job easier, or to increase government influence over the healthcare choices that individuals make or, if you really want to be cynical, to make people believe that government is giving them something for free, when they are really buying it with their own hard-earned money, more than it does something intended to improve the delivery of healthcare.
Regardless of that concern, the idea of giving people the resources they need to choose their own health insurance, rather than having employers choose their insurance for them, is a solid starting point. Here's the rest of the outline of Senator Wyden's plan, according to the Times…
Using the money from their employers, individuals would be required to purchase private insurance policies through state purchasing pools. Benefits would be keyed to the Blue Cross Blue Shield Standard Plan available to federal workers. Workers would not have to pay higher income taxes because of the employer contribution.A fuller description of the plan is available from Senator Wyden’s official website.The uninsured would also have to buy coverage, but premiums for the poor would be fully subsidized by the government, and middle-class families with incomes up to $80,000 for a family of four would be eligible for help on a sliding scale.
Premiums from individuals and contributions from employers would be collected by the government through the tax system and distributed to insurers. Once enrolled, individuals would be covered until retirement. Seniors in the Medicare program would not have to make any changes.
In short, the concept of the Wyden plan is really quite simple (as are most health insurance plans, contrary to what you may have been told. As Ronald Reagan once said, "There are no easy answers, but there are simple answers.")…
- Change the insurance system so that people within a state are pooled together and can buy health insurance, regardless of who their employer is,
- Require individuals to purchase a mandatory minimum level of health insurance, while allowing insurance companies to sell more coverage to people who are willing to spend more, and
- Create a new healthcare entitlement for people below a certain income level.
Oh, and where is the money for that new entitlement going to come from?
November 30, 2006
If Medicare Part "D" Ain't Broke, Will Sen. Whitehouse Still Try to Fix it?
I remember during the recent RI Senate race that Senator-elect Whitehouse made much of Healthcare, and, in particular, the "broken" Medicare Part "D" program (prescription drugs). In fact, it was number one on his Health Care reform To-Do list. While he was holding "the hands of seniors who are desperately afraid that they’ll wake up one day to find that the medicines they need the most are beyond their reach,” Whitehouse proposed that the Medicare Part "D" plan be "scrapped" and cited the Washington Post, which reported "only 1.4 million people – a fraction of the 8 million eligible – have signed up for the new benefit, despite a $400 million campaign by the Bush administration."
Well, now the Washington Post (via Barone) has reported this:
It sounded simple enough on the campaign trail: Free the government to negotiate lower drug prices and use the savings to plug a big gap in Medicare's new prescription-drug benefit. But as Democrats prepare to take control of Congress, they are struggling to keep that promise without wrecking a program that has proven cheaper and more popular than anyone imagined...Oooh, I know, I know! An election year issue to scare senior citizens!Polls indicate that more than 80 percent of enrollees are satisfied, even though nearly half chose plans with no coverage in the doughnut hole, a gap that opens when a senior's drug costs reach $2,250 and closes when out-of-pocket expenses reach $3,600. By the latest estimates, 3 million to 4 million seniors will hit the doughnut hole this year and pay full price for drugs while also paying drug-plan premiums.
The cost of the program has been lower than expected, about $26 billion in 2006, according to the nonpartisan Congressional Budget Office. The cost was projected to rise to $45 billion next year, but Medicare has received new bids indicating that its average per-person subsidy could drop by 15 percent in 2007, to $79.90 a month.
Urban Institute President Robert D. Reischauer, a former director of the Congressional Budget Office, called that a remarkable record for a new federal program.
Initially, he said, people were worried no private plans would participate. "Then too many plans came forward," Reischauer said. "Then people said it's going to cost a fortune. And the price came in lower than anybody thought. Then people like me said they're low-balling the prices the first year and they'll jack up the rates down the line. And, lo and behold, the prices fell again. And the reaction was, 'We've got to have the government negotiate lower prices.' At some point you have to ask: What are we looking for here?"
November 16, 2006
Emergency Room Usage is Sort of the Problem, But a Part that Could be Fixed
Commenter “Andy” (no relation, as far as I know) tries to provide a signature example of how emergency room overuse contributes to rising healthcare costs...
If an uninsured person has no primary care provider, they are less likely to seek help if they have (to take a silly example) a chronic stomach ache. Let's say, for the sake of argument, the stomach ache is the result of an ulcer. If the uninsured goes to a clinic early on, it seems to me that it is a relatively quick and inexpensive fix. If, however, the uninsured does nothing until the ulcer burns a hole in the stomach (or whatever it is that ulcers do - I am not a doctor) and then goes to the ER, then the uninsured will need surgery, which is a significant cost that can be recovered by driving up premiums/costs for the insured population.It is true that Andy’s example describes a situation, if frequent enough, that would drive up insurance rates for everyone. The longer people wait before seeking care, the more intensive care they are likely to need. More intensive care for more people means (assuming a traditional insurance model) that everyone’s insurance premiums go up.
Still, Andy’s example does not support the conjecture that the real cost of providing care at an ER is any greater than the real cost of providing care at a walk-in clinic or other type of facility. It�s the waiting that drives costs up, regardless of where care is finally delivered. However, for the rest of this posting at least, we can let this distinction pass, and focus on the issue that too many people waiting until they feel sick enough to go to a healthcare provider of last resort could be driving up healthcare costs for everyone.
Solving this problem takes us back to the paradox that universal care advocates generally want to avoid. Preventative care would catch some, maybe many, illnesses early, obviating the need for more expensive treatments. Yet there is no way, if we really want everyone to take advantage of preventative care programs, that it is rational to pay for them through an insurance-style system (full argument here). For preventative care, it makes much more sense to eliminate the middleman and pay doctors directly.
So what do we do?
The answer, in part, is to separate healthcare events into two categories, rare events (accidents, major illnesses) paid for through insurance, and routine events (regular check-up, initial examinations of aches and pains) paid for through direct reimbursement of doctors. Then, we give everyone the option of a health-savings-account plan for paying for the routine events. And then, knowing that regular check-ups and establishing a relationship with a general practitioner reduces the odds that someone will need intensive care, we sell health insurance at two different rates. Those who use some of their HSA money each year for a preventive care regimen get a slightly lower rate, because there are less likely to need major care in the future. Those who don’t pay a higher insurance rate for the same coverage.
Note that aspects of the over-regulation of health insurance, things like “community rating” systems, make this kind of common sense approach illegal in many places. It is deeply frustrating when government throws up regulatory barriers that prevent people from acting rationally and then says the only solution is a total-government takeover of the system that government mucked up in the first place.
November 14, 2006
Does Emergency Room Care Really Contribute to Rapid Healthcare Inflation?
Megan McArdle of Asymmetrical Information challenges emerging conventional wisdom that using emergency rooms for routine medical care is a significant contributor to rising healthcare costs (h/t Instapundit)...
It doesn't seem to me that emergency room care for routine ailments is actually more expensive to provide than clinical care; it's just that hospitals price it to cover the cost of dead, uninsured trauma patients and so forth. I don't see how a triage nurse, a doctor, and a waiting room are more expensive to provide because they're on the first floor than they would be on the fifth. But perhaps I'm missing something there.Agree or disagree?
November 3, 2006
The Fogarty Healthcare Plan Would be Blocked by the Courts
Should Lieutenant Governor Charles Fogarty have the opportunity to implement his universal healthcare proposal, he will find himself disappointed. A key section of his Hope Healthcare Plan would be disallowed by the courts, if challenged under Federal law.
The section that would not pass Federal muster is from Phase 2 of the Fogarty plan�
Employers will be required to provide health insurance coverage for their employees or pay a �fair share� fee. Employers with 10 or more employees will be required to pay an appropriate amount of money every year for each full-time-equivalent employee who is not covered through the employer or through another insurer. With the small business subsidy in place, providing insurance should not be an undue burden. Businesses that do the right thing and provide health insurance should not be placed at a competitive disadvantage with those that choose not to help insure their employees. These assessments will be collected in a state fund to support health insurance for uninsured Rhode Islanders who cannot afford coverage.A similarly structured plan, mandated by the government of Maryland, was struck down by a Federal District Court earlier this year (Retail Industry Leaders Association v. Felder [2006]). The District Court upheld the long-standing precedent that the Employee Retirement Income Security Act of 1974 (ERISA) prohibits states from regulating employee benefits any more stringently than the Federal government does. Ergo, a state government cannot require a company to provide health insurance to its employees because the Federal government does not require them to do so.
I�m not saying (for the purposes of this post) that this is a good thing or a bad thing, just that the courts have been consistent in interpreting the ERISA statute in this way.
ERISA is not a new law. It is disappointing that candidate for governor, especially one who is running TV commercials for universal healthcare, is completely unaware of ERISA's effects and limitations. That Lieutenant Governor Fogarty and his advisors and policy wonks are ignorant of the ERISA constraints on health insurance shows how closed-minded they are to the reality that part of America�s healthcare crisis has its origins in out-of-control regulation.
The Issue of Healthcare Reform, Brought to You by the Commenters of Anchor Rising
There's a good debate about healthcare going on in the comments section on last night's gubernatorial debate that's worth promoting into its own post...
October 18, 2006
Healthcare Forum, Part 2: Where Universal Coverage Can Never Work
To understand why universal coverage won't work for a certain segment of healthcare delivery, consider a fictional extension to your auto insurance policy. You are given the option of buying "gasoline insurance". Instead of paying for what you buy when you go to a gas station, you will pay a premium at the beginning of each week. In return for buying into the program, you can put up to $36 of gasoline into your car per week at any participating gas stations (after paying a $1 deductible).
The flaw in this system is obvious. If everybody puts their full allotment of gas into their cars each week, everyone will end up paying more than 35 dollars for 35 dollars' worth of gas; everyone will have to pay for the cost of their gas plus the administrative costs of running the gas insurance program. Savings under this program are only possible if a large number of people consistently use less than their allotment of gas, but people who consistently use less than their allotment are unlikely to stay in the program.
The point is that insurance doesn't work as a way for paying for something that is frequently used. I don't think that that is too controversial a starting point...
Now, move to an example closer to healthcare. Consider dental insurance. Do you believe that everyone should visit their dentist twice a year for a cleaning? If so, for the same reason that it makes no sense to pay for gasoline through insurance, it makes no sense to pay for routine dental care through insurance. If everybody goes for their twice-a-year cleanings, paying for those cleanings through insurance offers no advantage over paying the dentist directly. Everybody's dental premium could be dropped by the cost of two cleanings, people could use the premium savings to to pay for their cleanings, and everything would stay about the same (except of course for the insurance companies, who would lose out).
The dental example is very relevant; many current healthcare proposals involve using preventative medicine and regular check-ups to catch problems early when they are easier to correct. And if we are talking about regular, recurring care, just like with dental cleanings, it makes more sense to pay the provider directly (maybe with the help of a health-savings account) rather than through an insurance program. If preventative medicine is to be an important part of the public healthcare system, the design of that system must assume that everyone uses their full allotment for wellness care and check-ups and, therefore, that paying providers directly will be as effective and as efficient as paying them through insurance.
I still don't think I've said anything too controversial. However...
What about the person that can't afford the costs regular dental cleanings or wellness check-ups? Doesn't the government have a responsibility to provide for them somehow? Isn't that the real purpose of universal health coverage?
Certainly if you believe that preventative medicine is an important part of the healthcare system, providing for regular care for the poor is a concern, but it is not a question of how to offer universal healthcare insurance, but a question of how to offer healthcare subsidies. The difference, you ask? In an insurance system, everybody who is covered pays into the system. In a subsidized system, only some pay into the system based on their "ability to pay"; people towards the upper end of the of the ability-to-pay scale pay for both their own care and for the care of the people with less ability-to-pay, while people at lower end of the scale pay for only a fraction (down to 0%) of their own care. (Michael Kinsley discusses some of the differences between insurance and subsidies in this Slate magazine article).
But the fact that some people need subsidies to pay for regular, recurring careis not a reason to put everyone into a uniform, government-run universal system for delivering it. There is no medically justifiable reason to force people to spend their healthcare dollars in a certain way just because they are also the ones who are covering the costs of subsidies for others. If there are private insurance plans, or HSA's, or direct fee-for-service plans that are preferable to the government plan (and experience shows us that there almost certainly will be better plans than the government plan -- unless the government creates regulations to make them impossible) then why shouldn't people be free to choose those other options for themselves?
Some people will provide an ideological answer to this question. They believe that everyone should be in the same system to make everything fair, or to remove a stigma of receiving subsidized payments, or because they believe that government programs are inherently superior to private ones. These are all terrible rationales for using universal health insurance to provide subsidies for wellness care. Once the designers of the healthcare system make anything other than delivering the best possible care using existing resources their top priority, it is unlikely that the system will deliver the best possible care.
If people are serious about providing regular wellness and early-intervention medicine to as many people as possible, it cannot rationally be done through a "universal" insurance system. This is the realm where health-savings accounts will be most effective. The insurance system should be reserved for accidents and illnesses and major costs that are truly unforeseeable.
Healthcare Forum, Part 1
On Monday, I attended a candidate's forum sponsored by the Rhode Island Health Center Association. Federal candidates Lincoln Chafee, Jon Scott, Rod Driver, Sheldon Whitehouse, Patrick Kennedy and James Langevin; and state candidates Don Carcieri, Reginald Centracchio, Charles Fogarty and Elizabeth Roberts all gave answers to questions about health care asked by moderator Bill "Rap Man"(*) Rappleye of WJAR-TV.
Felice J. Freyer reported on the forum in the Projo. The tone of her article suggests that, taken as a whole, she wasn't exactly blown away by the answers to the questions that she heard...
Given impending cuts in Medicaid on the federal level, Channel 10 (WJAR) political reporter Bill Rappleye asked, would you use state money to fill the gaps, or would you prefer to increase fees or limit eligibility in a state-run health program for the poor and disabled....Mr. Freyer quotes Sheldon Whitehouse's call for universal coverage of some sort...Of the 10 candidates at the Rhode Island Health Center Association's annual meeting, only one or two (depending on how you take their answers) would go on record favoring either of these unpopular options.
Governor Carcieri, a Republican who is running for reelection, said he has appointed a team to look for ways to save money in Medicaid....Rodney Driver, an independent running for U.S. House in the second district, against U.S. Rep. James Langevin, favored having the state make up any federal losses in Medicaid funding. The state can do this by cutting back on waste, fraud and abuse within the budget, Driver said.
The other candidates did little more than decry the Medicaid situation. Medicaid, which is financed jointly by the state and federal governments, is a growing portion of state budgets as medical costs increase and the number of uninsured people grows.
There were few specific, direct answers to any of the three questions posed to each candidate....
It's a system that is screaming out for reform....We simply have to get universal coverage.Former Attorney General Whitehouse wasn't the only Democrat at the forum who supports a so-called universal solution. Congressman Langevin and Senator Roberts both mentioned the goal universal health care in their responses. Congressman Kennedy talked about healthcare as a moral problem. And Lieutenant Governor Fogarty has put forth a proposal for mandatory health coverage for all Rhode Islanders as part of his campaign.
The unanimity on universality may be the cause of the lack of specifics that Ms. Freyer decries, at least on the Democratic side. Democrats invoke "universal health care" like the words themselves are a magical incantation that will solve the problem. (To be fair, Congressman Langevin does have specific ideas about extending the health plan offered to Federal employees to all citizens, and Lieutenant Governor Fogarty has put forth a plan similar the Massachusetts mandatory-coverage plan that is detailed in its implementation, if not in how it will be funded). But when Sheldon Whitehouse, or Patrick Kennedy, or Elizabeth Roberts use the term "universal", we don't know quite what they mean, because universal coverage can mean many different things...
- At one extreme, universal coverage could mean a single-payer, government run system where government insurance is the only health insurance allowed and supplemental insurance is made illegal.
- At the other end, universal coverage could also mean a government run system as a base, with people allowed to purchase additional coverage from a private system. (I think, for example, this is what a country like Australia does).
The second idea, while blunting the effects of rationing in theory, would most likely lead to a system with some people being stuck in a poor-quality government program, others paying for better quality private coverage, and a never-ending political tension for new "funding formulas" to transfer more resources into the government program. In short, government would do to health care what it's done to public education over the past forty years.
The important thing to bear in mind is that the mixture of public and private in any healthcare reform is not a "detail that needs to be worked out", it is a choice that needs to be made up front. Politicians who favor universal care need to be honest with the public about exactly what they are proposing...
(*)I'm just reporting how the hosting organization referred to their esteemed moderator.
October 10, 2006
Question for the Projo Editorial Board: Is the Goal to Fix Healthcare, or is Fixing Healthcare the Excuse to Strengthen Government?
For the last several weeks (at least), the Providence Journal editorial board has been strongly advocating for implementation of a "universal health care" system. Here is an example from the October 3 Projo...
Until the United States puts everyone in the same risk pool (say, by extending Medicare to all), the situation will only worsen as the cost of increasingly high-tech medicine soars. That's especially so because those who have health insurance often ignore the cost of treatment; since they're not paying for most of it, they often overuse the medical system, injecting even more waste and expense.Here's another from September 30...The big question now is what percentage of middle-class voters who are losing health insurance will prove the critical mass that brings in a variant of the universal coverage and wide risk pool of other developed nations.
A national universal health plan is, of course, the logical solution to America's chaos of private insurance, state health plans, and federal programs. Every other large industrialized democracy has a national health system, as opposed to the rather barbaric U.S. "system."I am not a big fan of universal health care proposals. The health care crisis we face now is the result of excessive government regulation that separates people from having any influence on the form that their health insurance takes. Individuals are presented a very limited package of options through their employer once a year and are told to take-it-or-leave it. There are no serious alternatives allowing people to pay for better quality or seek lower costs, if they don't like the narrow range of choices they are given.
Imagine if we sold automobiles like we sold health care. Once a year, you would be given the choice to buy a car, but the only car you could buy would be a fully loaded BMW. If you couldn't afford it, too bad; buying a Ford Escort or a Chevy Cavalier would be illegal as per regulations set by the legislature. And if you didn't decide to buy your car at the beginning of the year, you couldn't buy one until next year. Under these circumstances, we would almost certainly face an "automobile ownership crisis", but it wouldn't be a market failure, it would be a regulatory failure.
However, there is one circumstance where I might be persuaded to support a statewide universal health care experiment, a proposal by economist Arnold Kling published in TCS Daily in response to Markos Moulitsas' argument that libertarians should vote Democrat...
What I propose is that Democrats promise to support one major libertarian experiment. In exchange for Democrats agreeing to support this experiment, libertarians would agree to vote for Democrats.I think most people can agree upon the basis of Professor Kling's challenge; our society is facing a number of crises rooted in the fact that certain of our systems, like the systems for delivering health insurance, or social security, or public education, were designed under assumptions that no longer hold true. They need to be changed and changing them will require a choice to move in either a more socialist or more libertarian direction.The experiment that I have in mind is school choice. If Democrats would instead prefer an experiment with voluntary investment accounts substituting for Social Security, that is an acceptable alternative. But for now, let us work with school choice...
Traditional Democrats may say, "If we are willing to give libertarians an experiment, what do we get in return? Do we get a chance to experiment with our policies?"
I would welcome experiments with socialist policies, provided that they are only experiments. That is, the policies must be evaluated, and if they are found to have failed, they must be abandoned.
For example, I would welcome an experiment in which four or five diverse states adopt single-payer health care. My guess is that if people were to experience single-payer health care for ten or fifteen years, that would provide powerful evidence that it is a bad idea for the United States.
Given all of this, here is my question to the Projo editorial board: will you consider the idea that it makes sense to try a number of different paths towards public policy reform and call for something like a voucher system in education or individual Social Security accounts to accompany your call for universal health care, or rather than fixing broken systems, is the top-priority of the reforms you seek pressing individuals into state-controlled collectives wherever possible?
July 25, 2006
Senator Tom Coburn on Healthcare Reform
At the Northeast Conservative Conference of the National Federation of Republican Assemblies held this past weekend at the Crowne Plaza in Warwick, I asked Senator Tom Coburn of Oklahoma what the Federal government's first step towards reforming health insurance in America should be�
Senator Tom Coburn: You can't tinker around the edges anymore. We have X-amount of resources to give to healthcare. The more of our total national income we put in healthcare, the less competitive we will be in the world. So how do we deliver healthcare best? We create a consumer driven, transparent healthcare market. The first thing we should do is pass John Shadegg and Jim DeMint's bill so you can buy your insurance anywhere you want.
I'll give you an example. In Oklahoma you can buy a family policy with a 500 dollar deductible for a year for 1200 bucks. That same policy costs 5900 dollars in New Jersey. Why should it cost 4 to 5 times as much? It's because they have 155 mandates that must be covered in New Jersey. What if I don't want to buy that?
We haven't allowed market forces to allocate resources. That requires some changes. That doesn't mean you give up state lines. The health industry is going to still have to report to the states, they will still have to pay into uncompensated funds in the states, but freedom should be given back to individual Americans. That will create innovation. That will get a lot of people insured who can't afford to buy insurance in New Jersey today -- they will have catastrophic coverage.
We're going to be introducing something in October and November that totally reforms healthcare across the country.
What you don't do is allow the Federal Government to try to design interoperable standards for healthcare IT, which they've been doing for two years to the tune of 160 million dollars and don't have anything yet. What you do is put 3 or 4 great software companies in the country in a room and say here's the money, go fix it and get it back to us. What they tell me is they could have something in 4 months, if we gave them 10 to 15 million dollars to do it, yet the government has already spent 2 years and 160 million dollars. Health IT is one of the places where we would save lives, cut costs, and increase innovation even further, but we've decided that government must design the system. Why?
July 21, 2006
"Fair Share" Healthcare Struck Down by the Courts
At the start of this legislative session, Representatives Amy Rice (D-Portsmouth/Middletown/Newport), Arthur Handy (D-Cranston), Raymond Sullivan (D-Coventry/West Greenwich), Joseph Faria (D-Central Falls), and Joseph Almeida (D-Providence) introduced a bill that would have required corporations with 1,000 or more people to either pay a fixed percentage of payroll for their employees health care, or pay into a state health insurance fund. The bill was passed by the Rhode Island House (H6917) but failed to pass the Senate (S2201).
Even had the bill been approved, it probably would have never taken effect. A Federal Court on Wednesday nullified a similar law passed by the Maryland legislature on the grounds that it conflicted with the section of the Employment Retirement Income Security Act of 1974 (ERISA) prohibiting states from regulating employer-sponsored benefit plans, including health insurance plans, any more stringently than the Federal government does. The decision will probably be appealed, but the courts have been very consistent in interpreting ERISA to mean that states cannot impose health coverage mandates on employers.
These so-called "Fair Share" plans (Maryland's, Rhode Island's, or any other state's versions) weren't good ones. They avoided any introspection about why problems with healthcare delivery have reached crisis proportions; they were typical of the big-government mentality that holds that if we can't be imaginative enough to facilitate something good for citizens, at least we can force everyone into something equally bad.
A better solution for improving healthcare delivery in America is to allow people more healthcare choices by 1) introducing health savings accounts 2) by decoupling health insurance from employment (by allowing individuals the same tax-breaks for buying health insurance that corporations get for offering it AND by eliminating the noxious provision of ERISA that protects insurance companies that provide employer-sponsored insurance from responsibility for the consequences of poor medical decisions they make and 3) by reducing the over-regulation of health insurance so companies can offer a range of coverages and deductibles tailored to meet individual needs.
May 16, 2006
The Healthcare Reform Being Filibustered in the Senate, Part 1 (What it is)
Last week, the Senate voted to continue a filibuster against the Health Insurance Marketplace Modernization and Affordability Act of 2005. Here's what the bill would do if passed.
Like all significant legislation relating to health insurance in America, this act relates to one of the most incomprehensible laws on the books -- the Employment Retirement Income Security Act of 1974 (ERISA). ERISA effectively divides health insurance into 3 regulatory classes...
- Employee sponsored plans, purchased through an insurance company,
- "Self-insured" plans, where a large company or labor union directly administers a health insurance plan, and
- Everything else.
A key provision of ERISA prohibits states from regulating ERISA-qualified plans (list items 1 and 2) any more strictly than the Federal government does. ERISA bars states from imposing any conditions on "self-insured" plans at all. However, ERISA also expressly reserves to the states certain powers to regulate insurance companies. Thus, although states cannot mandate the breadth of coverage provided by an employer, they are allowed to mandate the minimum coverage that must be provided by the insurance companies operating within their borders.
The final result is that big corporations and labor unions -- entities with enough people to support a go-it-alone self-insurance program -- can do whatever they want. Everyone else is strictly regulated by the government, via direct regulation of the insurance business.
What the Health Insurance Marketplace Modernization and Affordability Act would do is add a new class of plans to the ERISA regime. Trade associations and other commercially-oriented non-profits would be allowed to pool their employees for the purposes of purchasing "Small Business Health Plans" (SBHPs). SBHPs would be granted an exemption from state mandates similar to the exemption that self-insured plans already have (though the current version of the bill prohibits organizations qualified to offer SBHPs from self-insuring; I suspect this measure was added to the bill to placate the insurance industry, who would lose a great deal of business if trade associations were allowed to self-insure).
Since many trade associations have a national scope, this bill would give small businesses the opportunity to "cross state lines" to find a mixture of health insurance costs and coverage suiting their employees when available state-regulated insurance is too expensive. The law would not create a new category of "special rights" for SBHPs -- it would simply give SBHPs the special rights that big-entity self-insured plans already enjoy.
The Health Insurance Marketplace Modernization Act is a baby step in the right direction. But it's only baby step, because much of the healthcare "crisis" in America, and especially the crisis of healthcare "portability", is an artificial one, created by the unintended consequences of government regulation and ERISA in particular.
April 12, 2006
Ramesh Ponnuru on the Mass Healthcare Plan
At National Review Online, Ramesh Ponnuru offers his analysis of the Massachusetts healthcare plan, and offers a few suggestions to Massachusetts Governor Mitt Romney...
The governor has the ability to make modifications to this legislation through a line-item veto. He should use it to eliminate the mandates on coverage, strike the business taxes, and get rid of the individual mandate to buy insurance. (Or at least soften that mandate: His original proposal gave individuals more options in insuring themselves -- some of them pretty creative -- and did not rely on fines for enforcement.) Even if the overwhelmingly Democratic legislature rejects his changes, conservatives will appreciate his having made the effort.Ponnuru notes that Governor Romney's original preference included a wider range of catastrophic insurance plans...
Romney proposed eliminating laws that made it hard to sell cheap, no-frills, high-deductible catastrophic insurance policies. (Make insurance more attractive to healthy young people, and you might not need to force them to buy it.) But the legislature refused to eliminate mandates on coverage, and required zero deductibles for the new plans for low-income people.The legislature's refusal to create more insurance options should remind people that much of the source of our healthcare "crisis" is not implacable macroeconomic forces spiraling out of control, but bad government decisions that can be undone. We would face an "automobile ownership" crisis -- many people unable to buy cars -- if laws were passed making new BMW's the only type of car allowed to be sold. There's a place in the market for Ford Escorts as well as BMWs.
It's important for the citizens of Rhode Island to be aware of both this overriding principle and of the details of the Massachusetts plan, because Rhode Island may try to implement something similar in the near future. This is from a Felice J. Freyer article from Monday's Projo�
Rhode Island health-care leaders are watching with intense but wary interest as Massachusetts launches a landmark plan to provide health coverage for nearly everyone in the state...Unfortunately, if history is any guide, our state legislature is likely to Rhode Islandize the Massachusetts plan, implementing the features that maximize revenues collected by the government, whether or not they lead to an effective health insurance program."People have already approached me -- 'what would it take to do something like that here?' " said Christopher F. Koller, Rhode Island's health insurance commissioner. "There's an appetite for looking at this. There's a lot of potential applications for Rhode Island"...
Our goals are the same," said Lt. Gov. Charles J. Fogarty, a candidate for governor. "We want to see all our citizens have health insurance. . . . If we make it a priority in Rhode Island, I think we can do it. . . . We may not be able to do it in one giant step as they did in Massachusetts"...
[State Senator Elizabeth] Roberts, like others, said she wants every Rhode Islander to have health insurance and is eager to learn the details of the Massachusetts law. She pointed out that many Rhode Islanders work and obtain health insurance in Massachusetts, so there will be "a lot of transfer of information and experience."
April 6, 2006
David A. Mittell on the Mass Healthcare Plan
Projo columnist David A. Mittell likes the Massachusetts universal health care plan even less than I do.
Among other things, Mittell is concerned that using government regulation to force people to buy an inferior quality insurance product seems to be more of a giveaway to big insurance companies than it is good healthcare policy. Here is his complete list of objections...
Based on my speaking with legislators and health-care activists, who could, of course, only speculate, here is the scenario I think we ought to worry about:
- The bill is a sop to the powerful -- it protects big business and rewards big, profitable hospitals with big rate increases.
- It does not protect small business and small hospitals. It introduces an initially small $295 tax per worker per year on the labor of businesses not providing health insurance.
- It theoretically increases the number of insured, but has no way of assuring that the expanded coverage is reasonably comprehensive. It becomes, rather, a giveaway to insurance companies, and a bad deal for the newly insured.
- It doesn't appropriate enough money to provide good insurance. Its mandate for expanded coverage thus becomes what one legislator called "the camel's nose in the tent." When, in a year or two, the new plan is broke, without doing enough for the formerly uninsured, it will need a massive infusion of new cash, including a big increase in the $295-a-year tax on the labor of non-participating businesses.
- It creates a new bureaucracy with the impossible mandate of effecting top-down, bureaucratic "cost control." This entity doesn't control costs, but rather itself becomes a big cost.
April 5, 2006
The Massachusetts Univeral Health Care Plan
According to Pam Belluck in the New York Times...
Massachusetts is poised to become the first state to provide nearly universal health care coverage with a bill passed overwhelmingly by the legislature Tuesday that Gov. Mitt Romney says he will sign.The plan is a complex mixture of mandatory coverage requirements, tax incentives, and although Ms. Belluck tries desperately to avoid using the term, tax increases. Here's a few specifics culled from the news article...
The bill, the product of months of wrangling between legislators and the governor, requires all Massachusetts residents to obtain health coverage by July 1, 2007.Losing an exemption on state taxes is a tax increase. A penalty is a tax increase. Tax increases aren't inherently bad, but let's be honest on what this program is doing -- raising taxes on young people to pay for universal health insurance.Individuals who can afford private insurance will be penalized on their state income taxes if they do not purchase it. Government subsidies to private insurance plans will allow more of the working poor to buy insurance and will expand the number of children who are eligible for free coverage. Businesses with more than 10 workers that do not provide insurance will be assessed up to $295 per employee per year...
The Massachusetts bill creates a sliding scale of affordability ranging from people who can afford insurance outright to those who cannot afford it at all. About 215,000 people will be covered by allowing individuals and businesses with 50 or fewer employees to buy insurance with pretax dollars and by giving insurance companies incentives to offer stripped-down plans at lower cost. Lower-cost basic plans will be available to people ages 19 to 26.
Subsidies for other private plans will be available for people with incomes at or below 300 percent of the poverty level. Children in those families will be eligible for free coverage through Medicaid, an expansion of the current system...
Individuals who fail to get health insurance by July 2007 will first lose their personal exemption on their state taxes. In subsequent years, they would have to pay a penalty that could be as high as half of what an affordable health care premium would cost.
An aide to Governor Romney explains the focus on the young...
Eric Fehrnstrom, the governor's communications director, said that for those people with incomes above 300 percent of poverty, "our assumption was that these would be mostly single mothers who just did not have the wherewithal to get insurance. It turned out it was mostly young males. In some cases they are making very attractive salaries. These are people who just don't imagine themselves needing care, but of course when they break a leg when they're out bungee jumping they go to the hospital and we end up paying for their care anyway."This explanation should raise an immediate red-flag. Apparently, to initiate this program, the government needs to immediately grab a bunch of money from young people who don't use much healthcare and transfer it to others who do.
The problem is that the windfall of dollars added to the system is a one-time-only event that contributes nothing towards controlling costs. Once everyone is forced into the system (that has helped to create the problem by limiting the choices that people have), there's no one else left to tap, and measures like dropping treatments from coverage and even rationing become the only options as costs continue to rise. Ultimately, the Massachusetts plan does more to delay necessary reform of health insurance than it does to solve the problem.
Incidentally, today's OpinionJournal editorial mentions one of the simpler solution that would give people more control over their healthcare...
Congressman John Shadegg (R., Ariz.) has a bill to let Americans purchase affordable health insurance from any of the 50 states, thus bypassing state mandates that drive up insurance costs in New York and many other places.
March 23, 2006
Healthcare Assumptions
In Slate magazine, Michael Kinsley responds to a Paul Krugman/Robin Wells article in the New York Review of Books that argues that complete government control of healthcare -- where the government is the only insurance company, and maybe even all doctors work directly for the government -- is the only system of healthcare delivery that can work. (h/t Mickey Kaus).
Kinsley points out flaws in a number of Krugman's and Wells' assumptions. First, the argument for forcing everyone into a single government-run insurance pool is no more compelling for health insurance than it is for any other insurance sector...
Krugman and Wells note repeatedly that 20 percent of the population is responsible for 80 percent of health-care costs. But that doesn't explain why health insurance should be different from other kinds. The small fraction of people involved in auto accidents in any year is responsible for almost all the cost of auto insurance. You insure against the risk of being in that group.Second, Kinsley argues that advocates of government controlled healthcare too uncritically assert that centralizing bureaucracy is automatically a good thing...
Even the most competitive industry can seem wasteful and inefficient when described on paper. Dozens of computer companies making hundreds of different, incompatible models, millions spent on advertising: Wouldn't a single, government-run computer agency producing a few standard models be more efficient? No, it wouldn't.Third, Kinsley questions the argument that high-risk individuals will be left uncovered in any system not tightly controlled by the government. As he points out, this is based upon the assumption that there can be only one cost for health insurance...
Krugman and Wells say that private insurance is flawed by "adverse selection": Insurance companies will avoid riskier customers. Only a single payer (that is, an insurance monopoly) can insure everybody and spread the risk. But anyone is insurable at some price -- a price that reflects the cost they are likely to impose on the insurer. Adverse selection is only a problem to the extent that insurance is not really insurance, but rather a subsidy.
Unfortunately, Kinsley doesn't tell us exactly what a health coverage system based on his adjusted assumptions would look like (except to say it would be something more incremental than a complete government takeover of healthcare). So, after minutes of thinking about this particular article, I'll propose a system...
- Either government or mandatory catastrophic insurance for everyone from the moment they're born.
- Health-savings accounts (even with tax-breaks!) for preventative and routine measures.
- A robust, competitive private insurance market for stuff in-between.
March 7, 2006
Hospital Attitudes Towards Healthcare Delivery II
The Providence Business News article by Marion Davis on healthcare pricing also discusses legislation introduced at the behest of Governor Carcieri...
Gov. Donald L. Carcieri this year is pushing for legislation to require health plans to disclose to patients the negotiated amounts they pay to providers for services, procedures, tests, drugs or supplies that are subject to a deductible or coinsurance.The disclosure provisions are included as part of Senate bill 2614, introduced by Senator Leo Blais (R-Coventry/Foster/Scituate), scheduled for a hearing tomorrow.Prices for the most common items would have to be posted on the Internet, while the rest would have to be disclosed over the phone upon request.
Both hospitals and insurers seem to think that disclosing the price of hospital costs is a bad idea...
Stephen J. Farrell, CEO of UnitedHealthcare of New England, has already expressed concerns about the legislation (Blue Cross & Blue Shield of Rhode Island did not reply to a request for comment for this story). Hospital executives aren't keen on it, either.A concern about people making healthcare decisions based purely on costs is understandable. However, the executives quoted above seem to be taking this to an extreme.For starters, they say, the information is proprietary, part of their business dealings. Secondly, they say posting prices alone to guide consumers could be disastrous, because price is only one of many important factors they should consider.
"I happen to be a fan of consumer-driven health care," [Lifespan network senior vice president John] Gillespie said, but "it is utopia to say we're going to have a totally transparent system" with prices on the Internet.
[Women & Infants CEO Constance] Howes and [South County Hospital CEO Louis] Giancola noted that prices alone can be deceiving, too, because consumers won't know if a higher fee reflects higher-end equipment or expertise. Hospitals also have to keep their equipment available 24 hours a day, Howes said, and that increases their costs.
People are able to realize that price is not the only factor in decision making. An appropriate analogy here is higher education. The tuition at Brown University is very much higher than the tuition at Rhode Island College, yet the difference doesn't create a shortage of students wanting to attend Brown. People are willing to pay extra for the advantages -- that could accurately be described as advantages in "higher-end equipment and expertise" -- that Brown provides.
In an emergency situation, of course, you go to the nearest hospital available. But in non-emergency situations, is there really an argument against giving people information that can help them more easily match their needs with their means?
Hospital Attitudes Towards Healthcare Delivery
Marion Davis has an interesting article in this week's Providence Business News that discusses the maze of factors involved in healthcare pricing. One section of the article discusses how hospitals seem not to like the health-savings account/high deductible insurance combination because they don't want to deal with some basic record-keeping that would be involved...
Hospital officials tend to loathe high-deductible plans, because it forces their institutions to collect large amounts of money from their patients -- a task they neither like, nor are particularly successful with.I have a hard time seeing how this is a real issue and not mostly inertia on the part of hospitals. Why should keeping track of usage information and collecting under-deductible payments be any more difficult for health insurance than it is for something like auto insurance?There are complications, too: Constance A. Howes, president and CEO of Women & Infants Hospital, said it's common for the hospital not to be able to figure out how much a patient actually needs to pay, because there's no up-to-date information on how much of the deductible has already been met.
February 22, 2006
Discussing the Laffey Plan to Remedy High Drug Costs, Part 2
The next two problem/solution pairs proposed in Steve Laffey's plan to remedy high drug costs concern different aspects of the problem of regulation. (The first two problem/solution pairs are discussed here) .
1. The first issue is the relationship between the pharmaceutical industry and the Food and Drug Administration...
Today's Problem: FDA regulates drugs foremost on financial interest--not consumer safety (i.e. Vioxx)In 1992, the Federal Government implemented a "user fee" system where drug companies pay the government to help provide the resources needed for drug testing.
Laffey's Solution: Eliminate fees for FDA approval and ban experts with financial ties on drug advisory committees.
The problem with a user fee system is not conscious corruption. The problem is the nature of government bureaucracy and its incentive structure. In the private sector, success is measured in terms of a profit. In government, where there is no profit, we foolish humans still need some way to score our successes and failures. In public bureaucracy, management often measures its success in terms of its ability to increase its budget allocation. (An article in the Spring 2002 issue of the Cato Institute journal Regulation, mostly supportive of the user-fee system, agrees with this principle).
Once user-fees are built into the system, pressure inevitably builds on the government to push as many drugs through the testing process as possible in order to collect as much fee money as possible. It is certainly plausible that the 1.56% increase in drug recalls between 1993-1996 and the 5.35% increase in drug recalls between 1997-2001 reported by the Journal of the American Medical Association (via the Christian Science Monitor) is related, in part, to the bureaucracy's tendency to act, not evilly, but shortsightedly, thus warranting some re-examination of the practice of user-fees.
2. A second reform proposal focuses on the issue of patent law...
Today's Problem: Generic drugs are priced 20%-80% below brand names drugs, but comprise on 10% of total drug sales.A patent is supposed to be a deal that benefits both innovators and the public. An innovator gets rewarded for his work by having and exclusive period to market and/or license his product. In return for granting a period of exclusivity, the public learns the details of the innovation and, after the patent expires, is allowed to build upon those innovations.
Laffey's Solution: Increase generic drug distribution by closing drug loopholes, ending anti-competitive payoffs and adjusting effective patent life.
Unfortunately, patent law's current structure and enforcement is not consistent with its purpose. As soon as the generic drug maker notifies the Food and Drug administration that it is preparing to produce a generic version of drug about to enter the public domain, the brand name manufacturer can sue for a 30-month extension. In that period (and because of the sorry state of patent scrutiny in this country) they can attempt repatenting their original product, triggering other delays. Here's an example from reporting from PBS' Newshour with Jim Leherer showing how current law allows frivolous patents to stifle the purpose of the patent process...
What brand name manufacturers have done in some instances is go back and file new patents on those same drugs, some of them frivolous patents. In one instance, for example, a company suddenly went back and decided to patent the brown bottle that the cancer drug came in, because it said this brown bottle will preserve the potency of this drug. So it filed that patent anew. That triggered another 30-month stay.Other provisions in patent law encourage generic drug producers to sue brand-name producers in an attempt to shorten the lives of patents. A provision in the law allowing a generic drug producer an 180-day period of exclusivity after winning a patent-shortening suit caused an explosion in litigation starting in the 1980s. Robert Goldberg, Director of the Manhattan Institute Center for Medical Progress, explains the effect that this has had...
During the 1980s only two percent of generic drugs tried to cut patent life short as a way to approval. Today over 20 percent of all generic drugs now enter the market through legal attacks on patent life. And generic firms are attacking as soon as a drug hits the market -- with multiple challenges of the same patent in many cases. No wonder generic companies such as Barr Labs make most of their money not from selling medicines but from suing drug companies and settling cases.The Laffey plan would address these problems by simplifying patent law. Drug companies would not get an automatic 30-month extension on their patents. And to make sure that the get fully rewarded for their innovation, Mayor Laffey suggests reforming the law so that the clock on pharmaceutical patent doesn't start until the drug actually hits the market.
Clearer and simpler patent law would have a positive effect of creating a stable, non-litigious playing field for the production of both brand name and generic drugs.
Discussing the Laffey Plan to Remedy High Drug Costs, Part 1
The most difficult part of Steve Laffey's campaign platform for the traditional Republican base to swallow (so to speak) has been his promise to "fight the big drug companies". On Monday, Mayor Laffey laid out in detail his plan to remedy high drug costs. (Katherine Gregg and Jim Baron both provide good tastes of the overall flavor of the presentation in their reporting in the Projo and the Pawtucket Times, respectively).
Mayor Laffey summarizes his program in terms of six problems with six solutions. The first two problem/solution pairs are based on the assumption that pharmaceutical industry advertising creates an "artificial" demand that keeps drug prices high...
Today's Problem: Direct-to-Consumer advertising can inflate the need for brand name drugs and lead to inappropriate prescribing.Here are some general concerns about this set of solutions.
Laffey's Solution: Re-instate pre-1997 FDA disclosure requirements (for full-disclosure of ALL side effects).Today's Problem: Drug companies are spending more dollars on "Me-too" drugs that don't improve America's health.
Laffey's Solution: Require new brand name drugs to be superior than current drugs (or no patent!)
1. Certainly advertising is influential (after enough TV-ads, people will actually consider voting for Matt Brown for the Senate!) but prescription drugs, by being "prescription", are already supposed to involve a layer of protection between advertiser and consumer. They can only be sold after being prescribed by a doctor. In theory, doctors' judgements shouldn't be swayed by slick advertising campaigns.
If there is a problem with advertiser created demand, doesn't a large measure of the problem have to reside with the doctors who are writing the prescriptions? Also, if advertising is this powerful (and profitable), then why haven't generic drug makers developed their own advertising campaigns announcing that their drugs are just as good as brand name drugs to increase the demand for generic products?
2. The focus on "me-too" drugs -- drugs that have a different enough chemical composition to get their own patent, but serve the same function as a previous drug (the less perjorative term used to describe them is "follow-on" drugs) -- raises some specific concerns. The argument against follow-ons is that they inflate drug prices by discouraging people from purchasing cheaper generic drugs after the latest-greatest brand names hit the market.
Not everyone, however, agrees that follow-ons, because they have the same function as their parents, are all bad. The first argument for follow-ons is that they are necessary for providing treatment to patients who cannot use the orginal due to allergies or side-effects. (John Calfee of the American Enterprise Institute makes this argument). The second argument is good, solid economics. In theory, follow-ons ultimately drive prices down by making negotiation with drug companies possible by increasing the supply of drug options available for treating a particular problem. Too much regulation against follow-ons would restrict supply of available treatments, ultimately driving prices up. (Malcom Gladwell argues this position in the October 25, 2004 issue of the New Yorker).
Have all of the possible consequences of increasing the regulatory burden on developing follow-on drugs been given their due diligence?
Up Next: Some very sensible suggestions in the Laffey Plan on FDA & Patent Reform...
February 20, 2006
How the Most Boring Law Ever Determines the Shape of American Healthcare, Part 2
...Continued from the previous post.
Health insurers saw in the Employee Retirement Income Security Act of 1974 (ERISA) an incentive to sell as much insurance through employers as possible, because ERISA insulated them from any liability greater than the actual costs of treatments.
This aspect of the law was the key factor in making employer-based insurance the only health insurance product sold in America at reasonable prices. Under the protection of ERISA, insurers could include pre-care utilization review in employee sponsored health-plans as a way to control their costs. Pre-ERISA, pre-care utilization review was a risky proposition for an insurer. An insurer could be held responsible for complications (like death) following from a refusal to provide treatment.
ERISA changed this. Insurance companies working through employers could be held responsible for nothing more than the cost of a treatment denied. If an HMO improperly denied someone a $1,000 treatment, that individual could sue to obtain the $1,000, but not for consequences and complications caused by failure to have received treatment in a timely fashion. And because of the strict preemption rules, individual states could not pass laws that held insurers operating within their jurisdictions to any higher standard; this principle was most recently reaffirmed in the case of Aetna Health v. Davila (2004).
Given the risk-reducing advantages it provided to healthcare plans provided through an employer, ERISA motivated health insurance companies to get out of the business of selling insurance directly to individuals, and to sell health insurance only through employers.
ERISA may be the single most enervating factor in America's healthcare debate. More than any other single factor, through its removal of personal healthcare decisions to a remote court system, the weak remedies it mandates for major harm caused, and its general incomprehensibility, ERISA creates the perception that problems with healthcare delivery in this country are the result of intractable, impersonal forces that can only be solved with big-government solutions.
But ERISA is not an uncontrollable, unstoppable force of nature. It is just a badly written and poorly interpreted 30-year old law. The reasonable first step in fixing healthcare delivery in this country is not creating more bureaucracy and regulation to support the problems created by ERISA, but to remove health insurance from ERISA enitrely.
How the Most Boring Law Ever Determines the Shape of American Healthcare, Part 1
Rhode Island is one of several states where a bill pending in the state legislature would, if passed, impose penalties on large companies that do not spend a specified amount on employee health insurance (House bill 6917). In Maryland, such a requirement has already been passed into law, but is being challenged on the grounds that the Federal government prohibits any state regulation of employer-sponsored healthcare plans. OpinionJournal summarized the case last week...
The Maryland statute required employers with more than 10,000 employees to spend at least 8% of its payroll on health care. Only one company fit the bill: Wal-Mart....The legal term is that ERISA "preempts" any state regulation of employer-sponsored benefit plans. In the case of District of Columbia v. Greater Washington Board of Trade (1992), a case involving a law similar to the Maryland and Rhode Island laws (and cited in a letter prepared for the Maryland Chamber of Commerce explaining how ERISA limits the regulation options available to state legislatures), the United States Supreme Court explained how very broad the scope of ERISA preemption is...The good news is that the judiciary isn't likely to let such legal gerrymandering stand. The [Retail Industry Leaders Association] argues that both laws run afoul of the Employee Retirement Income Security Act of 1974, widely known as Erisa. One of Erisa's goals was to create a system in which nationwide employers could offer workers uniform benefits, free of conflicting state mandates...
ERISA sets out a comprehensive system for the federal regulation of private employee benefit plans, including both pension plans and welfare plans. A "welfare plan" is defined in �3 of ERISA to include, inter alia, any "plan, fund, or program" maintained for the purpose of providing medical or other health benefits for employees or their beneficiaries "through the purchase of insurance or otherwise."...The original focus of ERISA was not on health insurance, but on pension plans. The bankruptcy of the Studebaker automobile manufacturing company, which left thousands of employees unable to collect pension benefits they had earned, motivated legislative action on benefit regulation. The primary goal of ERISA was to apply strengthened reporting and funding rules to employer-sponsored benefit plans, reducing the likelihood that such plans would go bankrupt in the future.ERISA's pre-emption provision assures that federal regulation of covered plans will be exclusive. Section 514(a) provides that ERISA "shall supersede any and all State laws insofar as they may now or hereafter relate to any employee benefit plan" covered by ERISA.
To encourage businesses to continue to offer their employees benefit plans under the tougher regulations, ERISA gave employers two major breaks (in addition to tax-breaks) in the regulatory regime that it created. One was this idea of preempting any state laws. Large multi-state companies would not have to worry about operating under different regulations in different states. Secondly, ERISA reduced the risk involved in offering a benefit plan by limiting damages in benefit-related lawsuits to the exact amount of a benefit owed. If a company failed to pay out $1,000 it owed to an employee, the employee could sue for that $1,000, but not for any additional harm caused by the failure to recieve the $1,000 at the proper time.
Health insurers saw in ERISA a giant loophole that could be exploited to their advantage....
February 14, 2006
Froma Harrop on Health Savings Accounts
In a column in Sunday�s Projo, Froma Harrop expressed opposition to the idea of health savings accounts, at least as proposed by President Bush�.
Bush's new HSA is actually a rocket-powered tax shelter dressed up as a sweet little program to help the uninsured. It would also undermine the traditional health coverage now offered by employers. (More on that in a minute.) And in case anyone still cares about deficits, it would cost the Treasury $156 billion in lost tax revenues over 10 years -- more than wiping out any savings Bush hopes to achieve with his cuts in projected Medicare spending.1. The column�s emphasis illustrates why the country is not moving towards a national consensus on the issue of healthcare delivery. Liberal reformers focus almost exclusively on covering the uninsured. However, many people with health insurance have serious concerns of their own about the existing system, concerns like the fact that they have little control over what is and what is not covered, that changes in coverage are presented to employees in a take-the-whole-plan-or-leave-it fashion, that they may not be able to keep their current doctor if their employer changes insurance companies (which an employer might do without consulting their employees), etc.
To liberals (like Ms. Harrop) these concerns are secondary. Their overriding issue has become locking into law the power of remote collective entities -- either government or big corporations -- to regulate and control healthcare delivery decisions�
Like 401(k)s, the proposed HSAs could save money for employers while transferring the cost and risk of providing what was once an expected benefit onto the workers.In other words, because some people want to surrender their freedom to distant bureaucracies, everyone�s freedom to make decisions about their own healthcare delivery should be curtailed in order to reduce "risk".
2. Ms. Harrop seems to take the distressingly common liberal position that taxes are good things in-and-of themselves.�
Bush's HSA proposal is a wedding cake of tax credits piled on top of tax deductions. And unprecedented in the annals of tax breaks, this one would tax neither the earnings going into the accounts nor the withdrawals coming out. This is unlike 401(k) plans, in which people contribute pre-tax dollars into accounts but pay taxes on the money they withdraw.There is no mention of why this �unprecedented� tax cut is bad in terms of its impact on healthcare delivery, just the implication that a new way to cut taxes must be something undesirable.
Say you need medical services that cost $2,000, and you want to pay your healthcare provider directly. How much money do you need to pay for the medical services to be received? Under the "unprecedented" Bush plan, the answer is $2,000, if the money passes through an HSA. Ms. Harrop takes the position that to pay for $2,000 of medical services, you should pay the $2,000 to healthcare provider plus taxes to the government for the right to use your healthcare money where you need it.
3. The analysis of benefits that Ms. Harrop relies on borders on propagandistic. The Bush plan gives people both a tax-credit on the amount deposited into an HSA and tax-deduction from their gross adjusted income. Ms. Harrop, quoting a Center on Budget and Policy Priorities study, says�
The center figures that for a family making $180,000, a $1,000 contribution into an HSA would reap a $433 tax subsidy. If that family makes $15,000, the subsidy would total only $153 -- and that's assuming that a tax credit is made refundable. Otherwise, it would be zero.The $280 difference comes strictly from the deduction, not the credit. Everybody gets the same $153 tax-credit for $1,000 deposited into an HSA. The person making $15,000, however, gets no reduction in taxes paid on his adjusted gross income becasue he is in the 0% tax-bracket, i.e. he is paying no Federal income tax that can be reduced. The person making $180,000 gets to take $1,000 off of his gross adjusted income, resulting in $280 in savings in the 28% tax-bracket.
This kind of cheap-shot leads one to wonder if the rest of the analysis in the study is of the same dubious quality. It is obfuscating to favor a progressive income tax, then claim that any tax dedution is a �tax-cut for the rich� because it has a bigger impact on the people who are paying more under the progressive structure. Of course, CBPP and/or Froma Harrop could resolve this intellectual difficulty by coming out in favor of a flat-tax, where everyone pays the same percentage regardless of income.
December 23, 2005
Steve Laffey, Health Savings Accounts, and Conservatism, Part 1
The attention given to the vote on ANWR earlier this week stepped on bit of news relating to Steve Laffey in another significant policy area�
Laffey Introduces First HSA Plan in New England for Municipal Employees.HSA�s have potential to be the reform that fixes the healthcare mess in this country.Last night, Cranston�s City Council voted to ratify the tentative agreement negotiated between Mayor Laffey and Local 251, the Teamsters � comprised of 162 City employees. Most notable in the agreement is the introduction of Health Savings Accounts (HSA�s) as an option for the municipal employees.
Here�s how they work. An employer makes regular (tax-free) contributions to an HSA. The employee spends from the HSA�s for routine medical expenses, preventative check-ups, vaccinations, etc. The employee also purchases high-deductible catastrophic medical insurance (which is cheaper than comprehensive insurance) in case of a major medical emergency. The idea is to return insurance to being insurance -- many people pooling their money to help a few who need major assistance when an emergency strikes.
We�ll talk more about healthcare policy specifics in the coming year, but for now, I want to use this issue to emphasize Justin�s point from a few days ago � that the why of policymaking in many ways, is as important as the what and the how. The official announcement of HSA program from the Laffey campaign site is strong on the fiscal responsibility and the economic libertarian angles. These are both good arguments, but to fully understand the importance of HSA�s you need to go one step further�
Steve Laffey, Health Savings Accounts, and Conservatism, Part 2
Healthcare reform is necessary in this country not just because of the current system�s fiscal insanity. It's necessary because our present healthcare delivery system disrupts a fundamental connection in society � the relationship between healer and patient. While our leaders and the public in general weren�t paying nearly enough attention, laws were put into place that allowed insurance companies and government bureaucracies to insert themselves far too agressively between doctors and patients.
The bureaucratization of healthcare has consequences that reach beyond budgetary effects. The bureaucratization of healthcare contributes to a general feeling of insecurity in American society. Will I be able to go to my doctor tomorrow, if some bureaucrat decides to change the rules? Even if a doctor wants to treat me, will the insurance company allow him to? If some intermediary makes an improper decision, is there any chance of reversing it?
When individuals start feeling that too much of their lives have come under the control of distant, unaccountable actors -- and there's nothing more important to controlling your life than maintaining your health -- they despair about their ability to help themselves. And to help them where they feel they can't help themselves, people start demanding that government seize more power to try to fix things. But as government accumulates more power, it becomes inevitably less accountable, eventually becoming just another meddling intermediary.
HSA�s, which allow people to begin to seek medical treatment without obtaining permission from some remote third party partially motivated by something other than a desire to heal, help eliminate this insecurity. In doing so, they break the cycle driving society towards a mechanistic regime of government-controlled medical decision making.
By endorsing HSA�s Steve Laffey has presented a policy consistent with a humanistic conservatism that is cognizant of the fact that what good government does comes from building upon -- not replacing -- the relationships between and the innovation of individuals. Laffey's energy policy is based on the same idea. My hope is that we will to continue to see this theme as the Mayor presents his policy proposals in other areas and that Mayor Laffey himself, eventually, will spend some time directly explaining its importance.
December 19, 2005

Who Was Arguing for Importing Drugs from Canada?
From the December 19, 2005 issue of BioCentury, a biotechnology industry publication available only by subscription, comes a story entitled "FDA seizes imported drugs."
FDA said that in 1,700 parcels intercepted at three U.S. airports over a few days in August, only 15% of drugs that were promoted as "Canadian" actually originated in Canada. The agency said many of the drugs were not adequately labeled in English to assure safe and effective use, and that 32 of the pharmaceuticals sampled were determined to be counterfeit. The agency did not say how many drugs were sampled. FDA said the findings suggest that drugs ordered from Internet sites that consumers believe to be Canadian are not drugs of known safety and efficacy.
October 28, 2005
AIDS Drugs or a Japanese Garden: Which would You Choose?
Senator Lincoln Chafee took an anti-pork stand on a Senate floor vote on Thursday. According to Mark Tapscott of the Heritage Foundation,
President Bush had previously asked Congress to appropriate $30 million for construction upgrades at the Center for Disease Control facilities in Atlanta, including the Japanese gardens. There was already $240 million in previously authorized but not yet spent funds for the construction program.The amendment to transfer funds fromThe House approved the $30 million sought by Bush but when the bill came to the Senate, Coburn noted that it had increased the appropriation to $225 million, which meant there would be half a billion dollars available if the Senate version of the bill became law.
Coburn, who is a physician, offered the amendment to move $60 million from the CDC construction program to the AIDS effort. Doing so would mean "we will have enough funding to make sure everybody with HIV in this country has the medicine they need to stay alive," Coburn told the Senate, according to the Congressional Record for Oct. 26, 2005.
Coburn also told the Senate that the transfer was needed because "while people are dying from HIV, they cannot get medicines under the ADAP program because we cannot fund it significantly. We have multiple states with people on waiting lists. We have multiple states that cap the available benefits. It is a death sentence to those people with HIV today."
Senator Chafee was one of the 14 Senators who voted to provide AIDS drugs. Senator Jack Reed was one of the 85 Senators who voted to build the Japanese garden upgrade CDC headquarters instead. I would like to hear Sheldon Whitehouse's and Matt Brown�s position on this vote. So far, their Senate campaigns have been marked by unwavering adherence to national Democratic party positions. Would it be party discipline over doing the right and sensible thing on this issue too?
Finally, last week I posed the question of whether Senators and Congressmen are aware of what they are voting for when they pass these giant, pork-ladern approrpriations bills. Tapscott�s account of the Japanese garden amendment provides evidence that the answer is a thundering �No��
Coburn then noted that "the CDC has just completed a $62 million visitors center. I am asking for $60 million for people who have HIV, who are never going to get to the visitors center. I do not how we spent $62 million on a visitors center for the CDC but I believe that priority is wrong when people are dying from HIV and do not have the available medicines."Sen. Specter then responded to Coburn by first claiming there was not Japanese garden spending at the CDC facility in Atlanta, but then upon being corrected by a staffer, acknowledging that "maybe there could be a less expensive exotic garden than a Japanese garden."
UPDATE:
In an update to his original post, Tapscott wishes to clarify any confusion about the amounts involved...
Please note that the Japanese garden is part of a $60 million package of construction upgrades. The garden is NOT a $60 million garden. My apologies for the awkward wording when this post initially appeared earlier today. Being an editor, I should have caught that earlier.
October 26, 2005
Divided and Conquered by the Insurance Industry
From Tuesday's Pawtucket Times...
The tentative contract agreement, reached in private talks conducted well below the public radar, besides the 3 percent pay increase would change no other contract language, including the current lack of a health coverage co-pay.From Tuesday's Warwick Beacon...School Committee Chairman Alan Tenreiro confirmed those details Monday night.
Addressing the lack of a co-pay provision, Tenreiro cited city teachers' relatively low pay compared to other school districts around the state and likely union backlash, among other factors.
Mayor Scott Avedisian has advanced a proposal that would give teachers retroactive pay increases for the last two years without requiring the School Committee to seek a substantial additional appropriation and a supplemental tax increase....In his letter Avedisian says the City Personnel Department arrived at a $1.55 million cost for each year of the two-year deferral. He says if a co-payment for health care was also part of that package the deferred cost would drop to $728,654 for each of the years.
How is it that insurance companies successfully duck most of the ire centered on expensive and/or poor health care coverage? As is seen in the two examples above, insurance companies have convinced employers and employees to fight with one another over the ever-declining cost/quality ratio of the insurer's product. The insurer's choices to raise prices or to reduce or expand coverage are treated as immutable.
The ultimate solution to this problem is breaking the strange system of over-regulated corporate socialism that has evolved in this country for distributing health care. There is no law of nature that says health insurance can ONLY be purchased, at a reasonable rate, through an employer. Instead of being presented with one take-it-or-leave-plan through your employer, people should be able to shop from different insurance companies for the plan that suits them best.
September 15, 2005
Make-Believe Thinking About Drug Prices & Pharmaceutical Industry Economics
This posting responds to Steve Laffey's outlandish criticism last week of the pharmaceutical industry.
Originally part of an extended entry to this posting, the comments below - which represent counter-arguments to his suggestion that importing drugs from Canada would miraculously allow comparable patient care at radically reduced costs - were not sufficiently visible to readers. As a result, I am reposting a slightly modified version of my original comments here and deleting them from the original posting.
I have worked in the healthcare industry since 1983, spending most of my time since 1985 working in venture capital-financed startup companies. With that experience base, I found Laffey's words on drug prices - which you can read in the posting mentioned above - to be grossly misleading and grossly misinformed.
The Canadian Health System
The romantized - but fake - vision of simply importing inexpensive drugs from Canada in an effort to mimic their health system completely ignores the many grotesque failings of their socialist system discussed in an earlier posting entitled Canadian Supreme Court: "Access to a Waiting List is NOT Access to Health Care", including these highlights:
Canada is the only nation other than Cuba and North Korea that bans private health insurance..."Access to a waiting list is not access to health care," wrote Chief Justice Beverly McLachlin for the 4-3 Court last week. Canadians wait an average of 17.9 weeks for surgery and other therapeutic treatments, according the Vancouver-based Fraser Institute. The waits would be even longer if Canadians didn't have access to the U.S. as a medical-care safety valve. Or, in the case of fortunate elites such as Prime Minister Paul Martin, if they didn't have access to a small private market in some non-core medical services...
The larger lesson here is that health care isn't immune from the laws of economics. Politicians can't wave a wand and provide equal coverage for all merely by declaring medical care to be a "right," in the word that is currently popular on the American left.
There are only two ways to allocate any good or service: through prices, as is done in a market economy, or lines dictated by government, as in Canada's system. The socialist claim is that a single-payer system is more equal than one based on prices, but last week's court decision reveals that as an illusion. Or, to put it another way, Canadian health care is equal only in its shared scarcity...
...in Canada you wait for everything. North of the 49th parallel, we accept that if you get something mildly semi-serious it drags on while you wait to be seen, wait to be diagnosed, wait to be treated. Meanwhile, you're working under par, and I doubt any economic impact accrued thereby is factored into those global health-care-as-a-proportion-of-GDP tables. The default mode of any government system is to "control health-care costs" by providing less health care. Once it becomes natural to wait six months for an MRI, it's not difficult to persuade you that it's natural to wait ten months, or fifteen. Acceptance of the initial concept of "waiting" is what matters...
...[for single-payer health insurance systems] rationing by waiting is pervasive, governments overspend for the healthy and deny care for specialist and life-saving medical technologies to the sick, and leave health-care choices to bureaucrats rather than patients. Single-payer systems, in other words, often deny choice and access to the sick.
This denial and limited access also exists in market-driven systems...but at least sick patients in market-driven systems can explore options outside of rigid federal bureaucracies, as many Canadians do by coming to their neighbor to the south for care. The Canadian court decision debunks the myths that government systems offer equal access to care, that they offer a higher quality of care to all, and that a paternalistic government can take care of all of the people all of the time...
Preventing citizens from purchasing as much health care as they want and can afford under the pretext that it "wastes" resources needed to fund "free" health care presupposes that the state is the rightful owner of all wealth...
Further examples of the failings of the Canadian healthcare system can be found in a report entitled What goes into the cost of prescription drugs?...and other questions:
In British Columbia, some Canadians being treated with one effective medicine are switched to a substitute simply because the government health system mandates it. This can result in patient confusion, greater noncompliance, and a worsening of symptoms.Canadian patients are often denied easy access to certain medicines that, for them, would have minimal side effects, because the government requires that they must first endure therapy with the "cheaper," potentially less-effective medicines. Only when serious side effects appear - sometimes requiring hospitalization, for example - does the government allow the more efficacious drug to be prescribed.
Canadians wait, on average, seven months longer than Americans for new medicines to be approved by their government regulatory agency. Even after a medicine is approved, patients wait an average of five to 13 months longer before the medicine is put on and reimbursed by each province's formulary...
Canada ranks third-from-last in the developed world on the availability of medical technology, according to the OECD...
Is this the healthcare world we aspire to for all American citizens?
Adverse Macro Impact of Price Controls
In an article entitled The High Price of Cheap Drugs, John Calfee writes about the effect that price controls have had on innovative research, including the loss of jobs:
...Those price controls prevent innovative pharmaceutical firms from reaping free-market rewards anywhere but in the United States. That is one reason why the world pharmaceutical industry, which 20 years ago was mostly based in Europe, has largely relocated to the United States. American manufacturers now account for 7 of the top 10 worldwide best-selling medicines, and 15 of the top 20. This reflects a large and growing disparity in research and development expenditures. In 1990, European pharmaceutical firms outspent American firms on R&D by approximately 8billion euros to 5 billion euros ($7 billion to $4.3 billion). In 2000, U.S. firms outspent European firms by 24 billion euros to 17 billion euros ($20.9 billion to $14.8 billion). Even traditional European firms, notably GlaxoSmithKline and Novartis, have moved many of their most essential operations to the United States. After years of looking the other way, the European Commission is sufficiently alarmed by these trends to propose relaxing price controls in order to rejuvenate its pharmaceutical industry, especially the biotechnology sector...
Are we willing to pursue drug price controls in America and accept the resulting loss of jobs and innovation?
Drug Importation
As to the drug importation issue, David Frum frames the big-picture issue in this August 11, 2004 posting (no longer accessible on web) at his NRO blogsite:
...drug re-importation is a cheap and cynical non-solution to a real problem: the unfairness of asking Americans to pay the whole cost and more of new drugs while the rest of the world pays less. But it�s no kind of answer to cut prices in the US: In that case, innovation could disappear entirely. The answer is to share the cost more widely within the developed world � an answer that US trade negotiaters are beginning to press hard. So here�s the real question for [any politician] on drug prices: Will he stand up for American pharmaceutical-makers � and global pharmaceutical-users � by calling for a fair sharing through trade of the costs of innovation?...Or does he just want to score points now � at the price of denying Americans access to potential drugs of the future?
Are we going to hold our politicians accountable when they use cynical ploys to pander for votes? Are we willing to push for more equitable trade policies regarding drug pricing outside the United States?
Calfee adds his comments on drug importation from Canada:
...[Politicians] think this is competition and free trade at work. The fact that a group of Canadian or European bureaucrats would be setting drug prices for the entire U.S. economy seems to elude them. What would this law actually do? For one thing...might not get the low prices they want even if Congress passes their law. Prices won't drop in the United States unless foreign drugs really will be imported in large volumes. Importation from Canada alone won't do the trick because the Canadian market is tiny, about 5 percent of the U.S. market in terms of revenues. When Canadian pharmaceutical wholesalers ask Pfizer, Merck, and their competitors to ship them 10 times the usual volumes of Lipitor and Zocor and other blockbuster drugs, with the obvious intention of shipping them right back to the United States, any manufacturer with a decent regard for its shareholders will refuse. Why sacrifice billions of dollars in U.S. sales to maintain sales in a market one-twentieth the size? If that were the end of the story, events would follow a simple course. Canadian authorities, who understand the importation logic as well as anyone, would have to reassess their price ceilings or leave their citizens short of the best pharmaceuticals. At some point, it would become clear that Canadian drug importation would not bring the low U.S. prices its advocates want, although it might put a good number of patients at risk if importation--including importation of counterfeits--were to ramp up before prices adjusted. Prices in Canada, meanwhile, would rise...
Drug Safety
The second report referenced above includes these words:
...according to the Acting FDA Commissioner in July 2004, the FDA found evidence of a Canadian Web site advertising "Canadian generic" drugs, when in fact it was selling fake, contaminated and substandard versions of three commonly prescribed medicines. In addition, the FDA has identified drugs being imported into the U.S. arriving from unreliable sources in such places as the Bahamas and Pakistan. Media reports have found that some Canadian pharmacies are now shipping drugs from all over the world, including Belize, Israel, India, Chile, New Zealand, Ireland and Great Britian. So a drug that a consumer assumes is coming from Canada, may in fact originate anywhere in the world.According to Canadian Health Minister Ujjal Dosanjh: "Canada cannot be the drug store of the United States."...Additionally, Diane Gorman, Assistant Deputy Minister, Health Canada, said "the Government of Canada has never stated that it would be responsible for the safety and quality of prescription drugs exported from Canada into the United States..."
Calfee also discusses the risk of increased importation of counterfeit drugs:
...pass a law so that drugs shipped to Canada or Europe or South Africa can be imported into the United States for sale at foreign prices. The law would leave the Food and Drug Administration with almost no authority to check the safety of these imports. Wholesalers would have to do their own testing, but pharmacies and "qualifying individuals" (who could resell to others) would face no such requirement. This bothers the FDA...
Are we willing as a society to tolerate the greater human risk and higher economic costs resulting from use of counterfeit drugs by patients?
Long-Term Impacts
Calfee then notes how there are two eventual scenarios that arise from price controls and importation issues:
Two scenarios could play out, one bad and the other worse.In the first scenario, drug manufacturers would again simply refuse to ship huge volumes of drugs to small foreign countries in order for the drugs to be shipped back and cripple profits at home, where the drugs were invented. If that happened (and I think it would), our European friends would probably have a political fit. They would face the prospect of either going without American drugs or raising their own price ceilings--and with them the costs of their fiscally strapped socialist health care systems. From their point of view, the importation plan would be a clever way to force U.S. drug prices on Europeans. They would want very much to prevent that. An international demand for drug price controls in the United States (not just in Europe) would become a centerpiece of international diplomacy. And we might cave in, pushed by the same politicians who want importation.
In scenario two,...importation would rapidly escalate to massive volumes from Canada and Europe, maybe from South Africa and elsewhere. The process would resemble the "parallel trade" now engulfing European drug markets as products with Greek or Spanish labels flow to patients in Germany and Britain. Drug prices would drop here, limited only by fears of counterfeiting, dilution, or inadequate storage. Wholesalers, pharmacies, managed care organizations, and other large-volume dealers would feel intense price pressure from the imports, and the U.S. pricing structure would gradually collapse...
Either way, price controls would end up suppressing innovation here, just as they have done abroad. It is one thing for the Canadians and Europeans to free-ride on American R&D, but we can't free-ride on ourselves. The system that gave us the drugs the whole world wants would be hobbled...The market would understand with perfect clarity that the days of free-market rewards for high-risk-high-payoff research were over. The implications for future drug research are both obvious and depressing...
Are we willing to live with either of these outcomes in America?
Myths About Prescription Drugs
Robert Goldberg writes about Ten Myths about the Market for Prescriptions Drugs, including these excerpted thoughts:
Myth No. 1: American Spend Too Much on Prescription Drugs. Per dollar spent, drugs offer a better return on health care spending than virtually any other health care option. Using prescription drugs often reduces or eliminates the need for costlier health care services. One recent study found that every dollar spent on drugs is associated with a $4 decline in spending on hospitals...Myth No. 4: Drug Prices Are Higher in the United States than in Other Developed Countries. Drug prices in the United States are not very different from prices in other developed countries. Using accurate pricing information, health economist Patricia Danzon has found that drug prices in Canada, Germany, Switzerland and Sweden are higher on average than prices in the United States. When "purchasing power parity," a means by which economists attempt to compare the price of goods in different countries, is considered, the Organization for Economic Cooperation and Development has found that Americans spend less per capita per year on drugs than do people in Germany or France and only slightly more than those in Canada and Italy - yet the other countries have controls. (Go here for another verification of this point.)
Myth No. 5: Americans Could Reduce Their Drug Costs If They Paid the Same Prices as People in Less-Developed Countries. Critics of the U.S. system complain that consumers can buy drugs in Mexico for less than half their cost in the United States. Prices for the same drugs do differ in different countries, but Americans cannot get the newest drugs at Mexican prices for a simple reason. The research and development required to ready a drug for production can cost millions of dollars and take many years, but the cost of actually manufacturing a drug is usually small. Because manufacturers have discretion about pricing, the price may be close to production costs in poorer countries, which could not otherwise afford the drug, and higher in wealthier countries - more accurately reflecting the drug's value to patients. If all patients paid the lower price, there would be no money for research and development and no new drugs...Myth No. 7: Price Controls Can Reduce Drug Spending. Attempts to drive down drug costs through price controls have two unintended results: (1) they encourage increased consumption of drugs and (2) they lead to the consumption of inferior drugs. Many European health systems with price controls spend more on drugs per capita than the United States spends, but Americans use newer and more appropriate medications. That is one reason Americans spend less time in hospitals when they are sick and have a higher quality of life than do Europeans...
Myth No. 9: We Can Have Price Controls without Rationing Drugs. If federal price controls for pharmaceuticals were adopted, an increase in consumption of pharmaceuticals would be inevitable and the government would then try to control the increase. That is what happened with erythropoietin (EPO), which is used to reduce anemia in kidney dialysis patients. Medicare, which pays for drugs for kidney dialysis, put a price control on EPO in 1994, rationed the amount patients could get and refused to cover patients with healthy blood cells above a certain level...
Price controls represent not a mere extension of market pressure but a fundamental shift in values. Controls substitute a political process for the marketplace. For controls to work, individuals must be forced to adhere to governmental and bureaucratic decisions. This allows a few "experts" to decide what pharmaceuticals millions of physicians, pharmacists, medical researchers and patients "deserve" - and at what prices.
Finally, Did You Know?
That spending on drugs accounts for less than 11% of every healthcare dollar, of which branded drugs are about 7% and generic drugs are about 4%? That hospital care totals about 31% of every healthcare dollar, physician services about 22%, and nursing homes about 9%?
That studies show treating conditions with new medicines instead of older medicines increases drug costs but significantly lowers non-drug spending?
That developing a new drug takes 12-15 years and costs over $800 million?
That, on average, only five of every 10,000 compounds investigated are tested in clinical trials and, of those five, only one is ever approved for patient use?
That, on average, only three of every 10 prescription drugs available to treat Americans generate revenue that meet or exceed average R&D costs?
That pharmaceutical companies spend 20% of their revenue on research & development efforts for new drugs, equal to over $34 billion in 2003 alone and slightly over 10 times what they spent on direct-to-consumer advertising?
We need leaders who truly understand the economics of developing new drugs. If they stay ignorant, then we risk implementing policies which will lead to Americans losing access to innovative new drugs and losing the freedom we currently have to pursue the medical care we want.
And, if you needed any further evidence that the government is the last entity we want interfering with the marketplace, then reread this posting and share it with the next friend that whines about how the government should do something about the number of citizens lacking health insurance. Remind them that the government created the problem in the first place.
Our public debate and the ensuing public policies would improve if leaders did not go about promising economic benefits while simultaneously claiming the benefits can be realized without any costs.
Such suggestions are nothing less than a form of economic make-believe. In the end, if you won't deal with economic reality, then it will deal with you - on its own terms.
July 4, 2005
Employees are Paying an Ever-Increasing Portion of Health Insurance Costs
A Wall Street Journal article entitled Drug Co-Pays Hit $100 (available for a fee) notes the following:
Get ready for the $100 co-pay. That is how much state workers in Georgia will soon pay for certain brand-name drugs, in what may be the highest drug co-payment anywhere in the country.It is the starkest demonstration yet of employers' aggressive efforts to rein in the rising cost of prescription-drug benefits by driving employees to lower-cost medicines. Employer drug costs rose 83.4% over the past five years, an average of 16.7% each year, according to Mercer Human Resource Consulting, New York. And some estimates predict these costs will continue to rise at an 11% to 12% annual pace over the next several years.
As a result, consumers are seeing a variety of changes in their prescription-drug benefits. The most popular is tinkering with co-pays -- a set portion of the pharmacy bill that patients pay out of their own pockets -- to give patients a financial stake in what drugs they and their doctors choose. Just a few years ago, co-pays were rarely higher than $30, and most were much lower. Now, raising co-pays is a commonly used stick to discourage high-cost drug use. There also is a new carrot: making generic drugs free to patients by eliminating the co-pays altogether. Some plans divide drugs into two and three tiers, with less-expensive drugs requiring lower co-pays.
Also gaining steam is the use of "co-insurance," whereby the patient pays a percentage of the pharmacy bill rather than a flat amount. A few are experimenting with something called reference pricing, where patients typically pay extra if a prescription price exceeds a set "reference" level for the drug's category. And increasingly, plans are refusing to pay for a costly medicine unless patients first try less expensive alternatives or the doctors gets prior authorization from the health plan...
Employers and health plans say they have little choice but to find ways to reduce their ever-rising outlays for prescription drugs...
Co-pays have been rising steadily in recent years. According to Hewitt Associates, consultants to employers, nearly 40% of employers had co-pays of more than $30 this year, up from fewer than 10% 2001.
"Many employers have increased co-pays to the point where it actually equates to employees paying about 35% of the cost of drugs," says Debbie Martin, a consultant to major employers at Mercer. "That's about as high as they can go" and still have a competitive benefit that will attract employees...
Another increasingly popular approach to making patients more aware of drug costs has been to require "co-insurance," where a patient would pay 10% or 20%, even 50% of a drug's cost rather than a flat co-pay.
"We really want to impart to our employees that drugs cost a lot of money and you have to be aware of what you're taking and ask a lot of questions," said Nancy Tostanoski, senior vice president of global compensation and benefits at Starwood Hotels & Resorts Worldwide Inc. of White Plains, N.Y., which did away with flat co-pays for its employees in 2004. For most generic drugs, the co-insurance now is 25% and for brands 35%...
The article also contained this table:
CARROTS AND STICKSHow health plans are encouraging the use of cheaper drugs:
� Raising co-payments.
� Using co-insurance, where patients pay a percentage of cost, rather than a flat amount.
� Requiring doctors to get permission before prescribing an expensive drug.
� Refusing to pay for a costly drug until a less-expensive medicine is tried first.
� Cutting co-pays for generics.
� Offering discount coupons for over-the-counter medicines.
June 13, 2005
Canadian Supreme Court: "Access to a Waiting List is NOT Access to Health Care"
A Wall Street Journal editorial notes a landmark legal decision occurred last week in Canada:
...[T]he Supreme Court of Canada...issued an opinion last Thursday saying, in effect, that Canada's vaunted public health-care system produces intolerable inequality.Call it the hip that changed health-care history. When George Zeliotis of Quebec was told in 1997 that he would have to wait a year for a replacement for his painful, arthritic hip, he did what every Canadian who's been put on a waiting list does: He got mad. He got even madder when he learned it was against the law to pay for a replacement privately. But instead of heading south to a hospital in Boston or Cleveland, as many Canadians already do, he teamed up to file a lawsuit with Jacques Chaoulli, a Montreal doctor...
The court's decision strikes down a Quebec law banning private medical insurance and is bound to upend similar laws in other provinces. Canada is the only nation other than Cuba and North Korea that bans private health insurance...
"Access to a waiting list is not access to health care," wrote Chief Justice Beverly McLachlin for the 4-3 Court last week. Canadians wait an average of 17.9 weeks for surgery and other therapeutic treatments, according the Vancouver-based Fraser Institute. The waits would be even longer if Canadians didn't have access to the U.S. as a medical-care safety valve. Or, in the case of fortunate elites such as Prime Minister Paul Martin, if they didn't have access to a small private market in some non-core medical services. Mr. Martin's use of a private clinic for his annual checkup set off a political firestorm last year.
The ruling stops short of declaring the national health-care system unconstitutional; only three of the seven judges wanted to go all the way.
But it does say in effect: Deliver better care or permit the development of a private system. "The prohibition on obtaining private health insurance might be constitutional in circumstances where health-care services are reasonable as to both quality and timeliness," the ruling reads, but it "is not constitutional where the public system fails to deliver reasonable services."...The Canadian ruling ought to be an eye-opener for the U.S., where "single-payer," government-run health care is still a holy grail on the political left and even for some in business (such as the automakers)...
The larger lesson here is that health care isn't immune from the laws of economics. Politicians can't wave a wand and provide equal coverage for all merely by declaring medical care to be a "right," in the word that is currently popular on the American left.
There are only two ways to allocate any good or service: through prices, as is done in a market economy, or lines dictated by government, as in Canada's system. The socialist claim is that a single-payer system is more equal than one based on prices, but last week's court decision reveals that as an illusion. Or, to put it another way, Canadian health care is equal only in its shared scarcity.
...If the Canadian ruling can open American eyes to the limitations of government-run health care, Mr. Zeliotis's hip just might end up saving the U.S. system too...
Another Wall Street Journal news article (available for a fee) notes:
A ruling by Canada's top court is expected to open the door to broader private health-care services in the country, which often grapples with providing citizens with timely access to publicly funded health care.Canada's Supreme Court on Thursday ruled that the province of Quebec's prohibition on private insurance for services covered by the public system violates the province's bill of rights. Many policy experts believe the ruling will eventually spawn legal challenges to legislation in other provinces. It isn't clear, however, that such challenges would have the same success.
Some health-care professionals hailed the court's ruling as a recognition that Canadians should have the right to pay for privately insured medical services as a way to alleviate backlogs in the public system. "The Supreme Court is sending a warning shot to governments" in Canada that there is "no valid reason for stopping private health care" if the public system fails to provide timely access, said Normand Laberge, chief executive of the Canadian Association of Radiologists�
In practice, the demand for private services is likely to revolve around nonurgent care, Ms. Maioni said. In countries such as the U.K., which have a parallel private market, most of the urgent and expensive life-threatening cases still go back to the public system, she said.
Questions remain about how the ruling's effects will play out. The Quebec government indicated it will ask the Supreme Court to stay the ruling, possibly for six months to two years, so the province can make adjustments, which could involve altering the law or moving to reduce waiting times for public services.
And while the court ruled that Quebec's law violated the provincial bill of rights, the justices split 3-3 over whether it violated the federal charter of rights; and most provinces don't have their own bill of rights. What's more, since the case was heard, two justices have been added who are viewed as having relatively strong social democratic leanings, which could swing any future rulings against challenges to the public health systems.
More on the distortions caused by government meddling in the healthcare marketplace can be found in this previous posting.
Either you deal with economic reality or it will deal with you - on its own terms. That was something Hillary Clinton was too ignorant to grasp when she led an effort in the early 1990's to socialize medicine here in the USA. It is something others on the left still haven't learned.
Government cannot wave a wand and make the fundamental laws of economics go away. That is why socialism doesn't work. It is why socialized medicine will never work.
ADDITIONAL INFORMATION:
Mark Steyn adds his comments:
...On the other hand, to spot the drawbacks in your medical treatment, you first have to be getting some. And that's the design flaw in the Canadian system. As the chief justice, Beverley McLachlin, put it, "Access to a waiting list is not access to health care" � and in Canada you wait for everything. North of the 49th parallel, we accept that if you get something mildly semi-serious it drags on while you wait to be seen, wait to be diagnosed, wait to be treated. Meanwhile, you're working under par, and I doubt any economic impact accrued thereby is factored into those global health-care-as-a-proportion-of-GDP tables. The default mode of any government system is to "control health-care costs" by providing less health care. Once it becomes natural to wait six months for an MRI, it's not difficult to persuade you that it's natural to wait ten months, or fifteen. Acceptance of the initial concept of "waiting" is what matters...
Two recent letters to the editor of the Wall Street Journal (available for a fee) share their thoughts. The first letter includes these points:
...read Lives at Risk: Single-Payer National Health Insurance Around the World by John C. Goodman, Gerald L. Musgrave and Devon M. Herrick. The authors examine 20 such systems and conclude that rationing by waiting is pervasive, governments overspend for the healthy and deny care for specialist and life-saving medical technologies to the sick, and leave health-care choices to bureaucrats rather than patients. Single-payer systems, in other words, often deny choice and access to the sick.This denial and limited access also exists in market-driven systems, as Drs. Relman and Angell rightfully point out, but at least sick patients in market-driven systems can explore options outside of rigid federal bureaucracies, as many Canadians do by coming to their neighbor to the south for care. The Canadian court decision debunks the myths that government systems offer equal access to care, that they offer a higher quality of care to all, and that a paternalistic government can take care of all of the people all of the time.
The second letter adds these thoughts:
...how good intentions can justify any form of totalitarianism. Preventing citizens from purchasing as much health care as they want and can afford under the pretext that it "wastes" resources needed to fund "free" health care presupposes that the state is the rightful owner of all wealth...
June 6, 2005
Will Science Get Us OUT of a Moral Dilemma?
This would certainly be good news:
In recent months, a number of researchers have begun to assemble intriguing evidence that it is possible to generate embryonic stem cells without having to create or destroy new human embryos.The research is still young and largely unpublished, and in some cases it is limited to animal cells. Scientists doing the work also emphasize their desire to have continued access to human embryos for now. It is largely by analyzing how nature makes stem cells, deep inside days-old embryos, that these researchers are learning how to make the cells themselves.
Yet the gathering consensus among biologists is that embryonic stem cells are made, not born -- and that embryos are not an essential ingredient. That means that today's heated debates over embryo rights could fade in the aftermath of technical advances allowing scientists to convert ordinary cells into embryonic stem cells.
"That would really get around all the moral and ethical concerns," said James F. Battey, chief of the stem cell task force at the National Institutes of Health. The techniques under study qualify for federal grant support because embryos are not harmed, he noted. And eventually the work could boost the number of stem cell colonies, or lines, available for study by taxpayer-supported researchers.
May 18, 2005
Saving People's Lives: Why It's Exciting To Go To Work Every Day
I have had the privilege of working in the healthcare industry since 1983, joining my first biotechnology startup company in 1985. Just like physics had many of its heady years in the early part of the 20th century, the last 30 years have been similarly exciting times in biology. And there is no end in sight as we continue to learn more about the molecular basis of disease and how the human body works.
The annual American Society of Clinical Oncology (ASCO) meeting has just ended. One Wall Street Journal article (available for a fee) reports:
Drugs that specifically target cancer cells will be the focus of the American Society of Clinical Oncology's annual conference...Targeted therapies are considered the next generation of cancer drugs. Unlike chemotherapy, targeted cancer drugs avoid killing healthy cells, by choking off blood supply or signals that cancer cells need to grow.
Investors are awaiting data on several targeted therapies and their effects on a range of cancers. Presenting research will be companies such as Novartis AG, ImClone Systems Inc., GlaxoSmithKline PLC and Genentech Inc., which is partly owned by Swiss Roche Holding AG.
The annual ASCO conference is closely watched by Wall Street because of the sheer volume of clinical data presented. "It is the most important cancer conference of the year for doctors, patients and investors as well," said Le Anne Zhao, a Caris & Co. analyst...
The article then goes on to describe how various pharmaceutical companies would be reporting progress on their numerous clinical development efforts.
A second Wall Street Journal article (also available for a fee) tells the story of Genentech's recent run of drug development successes, as presented at the ASCO meeting:
...the spotlight will be on Genentech Inc., which is rapidly emerging as a dominant force in modern cancer treatment....researchers are expected to present details of several ground-breaking studies involving Genentech's new-style drugs, which precisely target the genetic weak points of tumors. Virtually alone among such similar targeted therapies, Genentech's drugs have proven surprisingly effective against some of cancer's biggest killers -- lung, colon and breast tumors, which together account for more than 250,000 deaths a year in the U.S.
For instance, Avastin, a new-style medicine that fights tumors by cutting off their blood supply, will be shown to extend the lives of lung-cancer patients and to improve the outlook for women with breast cancer. An older targeted drug against breast cancer, Herceptin, can cut in half the risk of cancer recurrence following surgery for a subset of women with particularly aggressive tumors.
Those results follow a year of other Genentech successes. Last year, researchers found that Genentech's drug Tarceva also improved the odds of survival for both lung -- and pancreatic -- cancer patients. And Avastin, which was approved last year for colon cancer, has piled up big sales numbers and proven effective at various stages of the disease as well.
Cancer drugs are notoriously hard to develop. Many seemingly promising drugs often fail outright when subjected to the most rigorous testing, and even among the new class of targeted therapies, disappointments vastly outnumber the rare successes. Over the past few years, however, Genentech's cancer drugs have bucked that historical trend in an unprecedented winning streak.
"I don't think anyone expected this," says Christopher Raymond, an analyst with R.W. Baird & Co. "These guys can't lose."
Genentech's drugs do not cure cancer, and as tested so far, rarely extend life by more than a few months on average. But cancer treatment, like football, is a game of inches, and cancer specialists generally welcome even incremental improvements over existing treatments. In addition, oncologists often point out that because new drugs are usually tested in the very sickest patients, many of them might be more effective at earlier stages of cancer....
Over the past two months, as news of the studies trickled out, its stock price has risen almost 70%. Measured by market capitalization, Genentech recently became the largest biotech in the world, edging out previous leader Amgen Inc. by a few billion dollars. It's also now bigger than drug-industry stalwarts like Merck & Co. and Eli Lilly & Co.
Genentech's success in this field is partly a matter of luck, since clinical trials of new cancer drugs remain an inexact science. But it also reflects the scientific rigor of the company's testing program. Unlike some competitors, Genentech routinely designs drug trials to prove that its therapies extend the lives of patients, an exacting standard that is arduous and time-consuming, but which tends to convince even skeptics when the results are positive...
Having lived nearly 20 years in the Bay Area, I remember watching Genentech grow from a small, young company. They have always been known for doing great research and not letting external pressures - which they certainly experienced a number of years ago - result in taking their eye off the prize. And, with their history of excellence, many of their alumni have gone on to be leaders in other successful biotechnology companies.
This interview with the Genentech CEO conveys the essence of their corporate culture. Another article about the company is here.
This article will educate you if you want to learn more about how breakthroughs in the biological sciences are changing the nature of drug discovery and development.
New drug development takes many years, has a very high rate of failure, and is extraordinarily expensive as this article notes. You can read more about the drug development process here. It is important to remember these facts when people with narrow political agendas focus on only 1-2 issues that alone do not tell a complete story. Successful innovations from companies like Genentech happen because they have the freedom to innovate and the ability to be rewarded for success after achieving the innovation.
Good research has led to valuable medicines, which are saving people's lives. It's why many of us in the industry are excited to get up and go to work every morning...knowing that we, too, have an opportunity to change the world in a wonderfully positive way.
April 28, 2005
Giuliani: Imported Pharma Drugs are Risky
A new report by Rudy Giuliani has found some flaws in importing drugs from other countries for use in the U.S. I note that the report was commissioned by the Pharmaceutical Research and Manufacturers Association, so that must be weighed. But I would also stress that Giuliani has certainly shown his integrity in the past. The key findings:
Unapproved drugs have already compromised the system. According to the report, nearly 90 percent of the suspected drug parcels randomly examined by airport mail facilities contained non-FDA approved medicines from Pakistan, Brazil, the Netherlands and Canada. Drugs are already coming from foreign sources. Several of the large Canadian Internet pharmacies have stated publicly that they are already filling prescriptions with drugs from other countries. Patients cannot assume these medications are identical to what they would get in the United States.
April 27, 2005
A Lifeguard for the Ocean
Providence Journal editor Don Sockol ends with a question a piece that laments his daughter's fear of losing healthcare if she returns to Rhode Island, loses whatever job allowed her to move back, and loses her health insurance:
There's been talk about school systems banding into larger purchasing groups to cut health-insurance costs. What if everybody joined one huge group, and wherever you went you belonged?
The short answer: because groups need administrators, and the bigger the group, the huger the administrator's power. There are very few people whom I'd entrust with my healthcare, and none whom I'd entrust with everybody's healthcare.
April 2, 2005
Reform All Around
I'd already added the Patients First Coalition to the list of links at left, but looking at their "Fast Facts on Why Rhode Island Needs Medical Liability Reform," I thought the following particularly noteworthy:
- 48% of physicians planning to leave Rhode Island within the next three years to practice elsewhere cite Rhode Island's high malpractice insurance costs.
- 71% of doctors have found it hard to recruit new doctors to Rhode Island.
- Rhode Island ranks last in the length of time it takes for malpractice cases to be resolved -- 6 years. The national average is less than 5 years and some states deliver justice in less than 3 years.
- Rhode Island has the 4th highest average malpractice award payment ($406,411) in the country.
- Rhode Island surgeons have experienced premium increases of 175% since 2002; general practitioners have experienced increases of 200% since 2002; and hospitals have experienced premium increases of 286% since 2002.
It's amazing how pervasive a state's problems can become after years of corruption and apathy.
January 13, 2005
Can Ohio's BestRX Drug Plan be Projected Nationally?
Heinz and Lewis accurately described the genesis and highlights of the Ohio plan.
Negotiations between the pharmaceutical industry (PhRMA) and a coalition of labor, church and consumer organizations (led by the Ohio AFL-CIO) resulted in "Ohio's Best Rx," a first-in-the-nation program that will slash drug prices for uninsured Ohio residents of any age who earn less than $22,450 per year, and uninsured Ohio families that bring home less than $44,000 per year.As to the last claim, the program will be initially funded by the Ohio taxpayers, but it is anticipated that the need for such support will disappear once the program is up and running. (Cue: Conservative skeptics, you may now raise your eyebrows). All and all, it would appear that Ohio's BestRX is an attractive bi-partisan solution to reigning in increasing drug prices. In fact, I could find none who argued against the program. One potential opponent, the Pharmaceutical Research and Manufacturers of America (PhRMA), as mentioned by Heinz and Lewis, was heavily involved in negotiating the plan. Kurt Malmgren of the PhRMA summarized his organization's view of Ohio's BestRX plan:
Ohio's Best Rx program, which begins this week, enables these Ohioans to buy drugs for the same average price paid by state employees and retirees, plus an additional $4 in fees ($3 to cover the pharmacy's professional services and a $1 transaction fee, to cover the program's administrative costs).
The potential benefit is enormous. Today, for example, a 30-day supply of the cholesterol-lowering drug Lipitor costs uninsured Ohioans up to $130. But if the state pays an average price of, say, $70, Ohio's Best Rx participants would pay just $74 -- a discount of more than 40 percent. A mail-order option will provide even greater saving.
What's more, these deep discounts are achieved without a big new bureaucracy. The program won't cost taxpayers a dime.
America's pharmaceutical makers understand that for some the cost of prescription medicine can be a challenge . . . We believe Ohio's Best Rx will provide a significant discount while preserving consumer choice, access and the ability of doctors and patients to determine the best treatments. Study after study show that patient health improves when they get the drugs they need. That is the mission and the goal of all pharmaceutical makers.With the PhRMA endorsing the plan, it would seem that the road is clear for other states to negotiate similar deals with the pharmaceutical companies. As such, I would have to say that perhaps there is room within the drug company profit margins for them to offer a bit of relief to their consumers. However, will lower prices result in smaller profit margins, thus affecting their R&D budgets and their concomitant incentive to produce newer and better, as well as less profitable, yet much-needed, drugs? What if similar programs are instituted nationwide? Perhaps such fears should be held in check. According to Heinz and Lewis
We realize that drug companies are not charities. But by making Ohio's Best Rx the model for a national plan, focused on the uninsured, the companies would not only generate goodwill; they might even eventually increase their profits. Whatever profits are initially sacrificed because of lower prices could well be made up or even exceeded through increased volume from millions of new customers suddenly able to afford needed medications.Maybe so. The willingness of the PhRMA to agree to the plan indicates to me that they hold a similar hope that this "Ohio model" will provide for sufficient profits to fund R&D, etc. I just wonder if they can be expected to support this model on a nationwide basis. If Ohio's plan proves successful, I suspect we will find out.
January 4, 2005
Health Care & Big Pharma IV: Some Solutions, No Single Answer
As Justin recently pointed out
There are a number of topics in which we find other countries getting away with practices that would have dire consequences were the United States to emulate them (the atrophied militaries of Europe come to mind). That, it seems to me, is the price that the U.S.A. pays for being the U.S.A. The question of the century may very well be whether we're a sufficiently mature people to acknowledge and accept it.Within this context, the question Americans face when it comes to drug prices is whether we are willing to continue to subsidize the rest of the world. It is becoming increasingly apparent, to those inside and outside of the U.S., that we are not. Unfortunately, this deeper issue has been masked by the prospect of a short term solution: the importation of cheaper drugs from foreign countries. What has not been discussed in this debate is that the short term savings accrued by purchasing cheaper drugs from other nations (who impose price controls) will eventually disappear as normal market forces gradually come into play.
But are drug prices really that high in the U.S.? A recent study concluded that, while the U.S. does pay more for drugs than other countries,
the differences are not nearly as large as they appear at first glance. The higher prices in the United States are concentrated among a subset of brand-name drugs and among those without insurance covering drugs. Some U.S. health plans obtain price concessions from manufacturers similar to those obtained by national governments. (1)While the particular point regarding specific drugs may be true, it is this �sub-set� of brand name drugs that are those most desired by Americans and are attractively priced overseas. Further, even if insurance companies do bargain with pharmaceutical companies for lower prices, the current focal point of controversy is concerning those whose drugs are not covered by insurance. Here in Rhode Island, the quick solution to the dilemma has been to approve the importation of cheaper drugs from Canada. Perhaps a better and longer-term solution would be to network the uninsured and those without prescription drug coverage so that their purchasing power would be greater, as proposed by RIPIRG.
It is important to explain that price controls in Europe has fostered a parallel trade market for pharmaceuticals within the European Union.
For many years the varying methods of price control of medicines by national governments in the European Community (and elsewhere) have resulted in wide variations in prices. Parallel traders buy products in low pricing Community countries and sell them, generally relabelled or repackaged, in high pricing Community countries. This practice diverts sales revenue and profits from the manufacturers to the traders, distributors, pharmacists and, in some measure, to the sickness funds and to some patients. While parallel trade appeals to those who gain financially, its basis is a market distortion that poses a significant threat to the future of the research-based pharmaceutical industry.(2)What many in the U.S. are pushing for is essentially an extension of the European parallel trade market into our country. Under this system, it appears that everyone but the pharmaceutical companies benefits. If it is assumed that �Big Pharma� can currently afford to take the hit, the question that should be asked is: for how long? How long before R&D is insufficiently funded? How long before drug companies determine that broad-based price increases are the only method by which they can continue to finance R&D and maintain a profit motive? The answer is that we are fast approaching this point. Drug companies are aware of parallel markets and have countered with drug price �convergence,� whereby one price is set and charged to all nations. This so-called �euro price� has a negative affect on those who can least afford it.
The primary losers from 'euro' pricing will be consumers in low income countries who will face higher prices or loss of access to new drugs. In the long run, even higher income countries are likely to be worse off with uniform prices, because fewer drugs will be developed.(3)In Europe, they have come to realize that parallel trade itself is not enough to keep drug prices low. For the first time, these countries are instituting cost-sharing plans (what we would call co-payments) for their drugs. Such was proposed as early as 1997, in a study that
policy should aim to contain growth in pharmaceutical expenses by means specific to reimbursement rather than direct price controls. By encouraging doctors to prescribe and customers to use generics, competition is enhanced to bring down drug prices. More emphasis is being laid by government in educating customers to cost-awareness and cost-benefit ratios with regard to pharmaceuticals.(4)Key to this program is making consumers and doctors aware of cheaper generic drugs. However, unless co-payments are indexed to actual drug costs, and not just a simple flat-fee, there is no consumer incentive to select a cheaper generic version over an established drug.(5) In Germany,
Starting in 1989, a maximum reimbursement for a given medicine replaced a flat prescription fee. This change in reimbursement exposes the patient to the price of a prescribed product. Using a product-level panel data set covering several therapeutic categories before and after the policy change, I find that producers significantly decrease prices after the change in potential patient out-of-pocket expenses. Price declines are most pronounced for brand-name products. Moreover, branded products that face more generic competitors reduce prices more.(6)The availability of generic drugs is dependent on patent expiration. Some seek to shorten the length of drug patents in hopes of quickening competition within a given drug class. Others have offered more innovative solutions.
To restore competition to all parts of the pharmaceutical industry, we propose a new institute at the National Institutes of Health that would compete with the private sector for pharmaceutical intellectual property by establishing competition for research and development contracts open to public and private institutions; retain the resulting patents; and grant cost-free, nonexclusive licenses to all qualified producers.(7)This seems an attractive option that sets up the government as a competitor, not a sole developer, in drug R&D and provides for some measure of free-market development competition. Taking it a step further, some believe that entirely publicly supported research, even if �considerably less efficient on a dollar-per-dollar basis than patent-supported research� would be beneficial.
The main reason for this conclusion is that patent monopolies lead to enormous economic distortions, including expensive sales promotion efforts, research into "copycat drugs," incentives to conceal unfavorable research findings, and other inefficiencies that economic theory predicts would result from a government-created monopoly. The gains from publicly supported research, coupled with a free market in the production of drugs, could reach into several hundred billion dollars annually within a decade.(8)Thus, government inefficiency, manifested as more tax-dollar expenditure, is deemed an acceptable loss on the way to reducing overall drug costs. The only problem it is rare indeed when a government program becomes more efficient over time. It could be reasonably expected that there will come a point where the government inefficiency would eventually approximate the �losses� from higher drug prices that had been projected and that the sole-source government program was intended to deflect.
It seems, then, that we have a few reasonable, long-term solutions available to us. Yet, these must be weighed against how they conflict with true "free-market" economics, especially business incentives. For we must not forget that pharmaceutical companies are businesses, albeit ones that traffic in goods that are deemed beneficial to mankind. This makes them unique. As the rhetoric has risen, so has the basic assumption that health care, and drugs, are a "right." In such an environment, profit motives and the bottom-line get lost or are deemed inhumane aspects of the conversation. However, profit motive is the most important aspect of the entire debate. Without incentive, why make a product? Without adequate R&D funding generated from drug sale profits, companies will be unable to develop newer and better drugs. However, how do we ensure that the profits are not beyond reasonable? The answer is: We can't, only competition can. As such, the ideal way to tamp down prices would be to encourage competition through true free-market principles. Unfortunately, this probably won't happen so long as other countries, large insurers and the U.S. government continue to negotiate prices with Big Pharma.
With no real prospect for real reform, it seems there are four reasonable options available to attempt to bring prices down. The first is for individuals and small groups to unite and negotiate side deals of their own with the pharmaceutical companies to try to solve their acute drug cost problem. The second would be to encourage competition by limiting patent exclusivity, though not to such an extent as to adversely affect product return-on-investment for the drug companies. Third, and following from the second, with increased competition a concerted effort to make patients and doctors aware of cheaper alternatives to "first in the market" drugs combined with variable co-payments will reduce demand and foster competition. Fourth, and last, the viability of a plan to turn the NIH into a drug developer within a competitive environment, and not just a research funding device, should be investigated.
Obviously, there are other ideas out there that I have not touched on. My goal in writing these posts was to clear up in my own head what the "Big Pharma" debate was about. The fundamental point I have taken away from my research is that the average citizens of the United States are not operating on a level playing field with the rest of the world. Unfortunately for us, the rest of the world isn't going to suddenly decide to pay higher prices, and thus share the burden of R&D, on their own. Given this, all we can really attempt to do is implement small reforms, some of which I have outlined above. Hopefully, these can lessen our burden as we await market forces to impact the rest of the world and tilt the playing field back to equilibrium. Absent that, we are left to accept that so long as we are the world's dominant power we will be held to a higher standard...and higher prices.
FOOTNOTES:
(1) J.L. Wagner and E. McCarthy, �International Differences in Drug Prices,� Annu Rev Public Health. 2004;25:475-95.
(2) I Senior, �Is parallel trade in medicines compatible with the single European market?,� Pharmacoeconomics. 1992;1(Suppl 1):70-6.
(3) P.M. Danzon, �The economics of parallel trade ,� Pharmacoeconomics. 1998 Jul;14(1):135-7.
(4) G. Emilien, �Future European health care: cost containment, health care reform and scientific progress in drug research,� Int J Health Plann Manage. 1997 Apr-Jun;12(2):81-101.
(5) S.M. Ess, S. Scheeweiss, and T.D. Szucs, �European healthcare policies for controlling drug expenditure,� Pharmacoeconomics. 2003;21(2):89-103.
(6) N. Pavenik, �Do pharmaceutical prices respond to potential patient out-of-pocket expenses?� Rand J Econ. 2002 Autumn;33(3):469-87.
(7) P. Stein and E. Valery, �Competition: an antidote to the high price of prescription drugs,� Health Aff (Millwood). 2004 Jul-Aug;23(4):151-8.
(8) D. Baker, �A free market solution for prescription drug crises,� Int J Health Serv. 2004;34(3):517-26.
December 30, 2004
Imports and Price Controls for a Mature Nation
The idea, which Marc noted in the previous post, that "Europeans and Canadians are able to get quality drugs at lower prices only because Americans pay free-market prices that fuel research and development" is one that I've touched on before. Michelle Malkin had made the point that the price negotiation practices of the Veterans Administration would be catastrophic if transported to a program as huge as Medicare. (She also offers this bit of corrective to the Harrop line: "the [Medicare drug] law will create a number of regional health plans, each of which will be free to use committed-use contracting on its own.")
As I wrote at the time, the benefits of collective bargaining and unified administration only outweigh the costs as long as the group is reasonably small compared with the total market. This goes for various groups within the U.S. market, and it goes for various countries on the global market.
There are a number of topics in which we find other countries getting away with practices that would have dire consequences were the United States to emulate them (the atrophied militaries of Europe come to mind). That, it seems to me, is the price that the U.S.A. pays for being the U.S.A. The question of the century may very well be whether we're a sufficiently mature people to acknowledge and accept it.
Health Care & Big Pharma III: Imports and Price Controls
According to a study by the Rhode Island Public Interest Research Group (RIPIRG), uninsured Rhode Islanders pay 79% more for prescription drugs than do insured individuals. RIPIRG puts the blame squarely on drug companies. The first charge is that drug companies inflate R&D costs to justify their high prices. The second charge is that drug companies have agreed to charge lower prices for drugs sold to both foreign countries and the U.S. Government because they agreed to institute price controls. RIPIRG recommends that, in the short term, U.S. citizens should be allowed to purchase Canadian or other foreign drugs. A longer term solution would be to create a statewide buying pool in which smaller entities could combine to negotiate lower-priced drugs. For now, at least according to the Providence Journal, it is the short-term recommendation, Canadian drug importation, that is generating the most noise.
However, I find I do agree with one thing Froma Harrop stated in her aforementioned and most recent column, "forget about importing drugs from Canada. All this talk is a sideshow..." Harrop believes the answer lay in negotiated price controls. Using the recent negotiations over the new prescription drug provision in Medicare, Harrop points out
Americans had a golden opportunity to extend this practice to the new Medicare prescription-drug benefit. But the bill that passed forbids any haggling on price. As a result, a fabulously expensive entitlement will cost taxpayers tons more money than it had to.While I agree with Harrop in the acute example she has given, and I also think that Tauzin's actions do appear unseemly and Thompson's as disingenuous, I'm not sure how price controls negotiated for this specific program could translate into more "universal" drug price reductions, as Harrop seems to imply.
This shameful piece of legislation was the handiwork of Billy Tauzin, Republican of Louisiana. Tauzin is leaving Congress for a $2-million-a-year job heading the Pharmaceutical Research and Manufacturers of America, the drug-industry trade group. Given what Tauzin has done for drug makers, he would have been cheap at twice the price.
Tommy Thompson, meanwhile, is on his way out as secretary of health and human services. As a parting shot, Thompson said that the Medicare drug bill should have let the government negotiate prices on behalf of the beneficiaries. How nice of him to speak up, now that it no longer matters.
There are two problems with implementing price controls on a widespread basis. The first was illustrated by Don's recent post, "Government Meddling Creates Marketplace Distortions, Increasing Long-Term Costs." The second is that price controls remove incentive. These two usually go hand-in-hand as was illustrated by the recent shortage of flu vaccine. According to Dr. Gilbert Ross, Medical/Executive Director of the American Council on Science and Health
when the government gets involved in pharmaceutical pricing, consumers should expect disastrous consequences. Recent shortages in children's vaccines can be traced directly to the government's power, as sole purchaser, to dictate below-market prices. This "negative subsidy" has a chilling effect on manufacturers' incentive to produce and market vaccines, which explains why so few continue to make these vaccines. (Unfounded but attention-getting lawsuits against vaccine makers have similar effects.)According to a May 2001 Wired Magazine article, Dr. J. Leighton Read, former CEO and founder of Aviron and Edward Penhoet, (who was recently named as Vice-Chairman of California's Stem Cell Research Board by California Governor Arnold Schwarzenegger), agreed that
drug companies will be less willing to take the substantial risks involved in developing drugs for diseases such as AIDS that are rampant in the Third World, if they are eventually required to give their product away for free.Even though I applaud Read for his candor, I don't believe the general public will be amenable to this line of thought. Within the same article, Dr. Alan Garber, a professor of medicine and director of the Center for Health Policy at Stanford University, stated, "I think we have been too timid about looking at models other than controlled pricing." He believe that one possible solution "would be fixed prices for insurance companies to purchase an unlimited amount of drugs." Finally, while I previously linked to his piece, Robert Goldberg's observation bears repeating (in shortened form)
It costs about $500 million to bring a drug to market -- about the same amount it takes to build a power plant.
Read, who also founded Affymax, suggested that consumers rethink "anything assumed to be an entitlement."
"We need to feel some of the pain," he said.
there is only a limited amount of drugs that can be supplied at price-controlled levels worldwide. . . Europeans and Canadians are able to get quality drugs at lower prices only because Americans pay free-market prices that fuel research and development. . . the high level of pharmaceutical R&D ultimately depends on revenues: Cut drug-company revenues, and you necessarily cut R&D. . . applying relatively moderate price limits just to purchases under the new Medicare drug benefit . . . would reduce new drug investment by over $300 billion over the next two decades. This drop would consequently deprive many millions of ailing people of potential cures. . . Gvernment price controls are already shortchanging Europeans and Canadians. They have led to a decline in investment, with venture capitalists investing 15 times more in biotech companies in America than they do in the same number of European firms. Health systems and consumers must also spend more to treat chronic illness there because they don�t get new medicines as quickly or as widely as we do. German and British patients, for example, are less likely to receive new cancer drugs than Americans. . . If we import price-controlled drugs, we will import these shortage-created side effects too.If drug importation is only a stop--gap and price controls and greater government intervention haven't worked elsewhere, what will work in the United States?
I will attempt to come up with some solutions in my next post.
December 29, 2004
Would this be Legal?
Here�s a question I need answered to fully understand the failure of the American health insurance system:
General Motors announces it will be selling automobiles in a new way. It will no longer sell cars to just any individual. Instead, GM will sign contracts with employers. If you work for a company that has signed a contract with GM, you can buy the car at regular price. If not, it will cost three times as much. Would this program be legal under existing commercial law?
Let me add a corollary: Is it even illegal for a private seller to charge different prices for a product based on age, or race?
Health Care & Big Pharma II: In Defense of Drug Companies
In my last post I laid out the case against big pharmaceutical companies as portrayed by Marcia Angell, former editor of the New England Journal of Medicine and author of a recent book that has garnered some acclaim for taking on "Big Pharma." Angell has put forth many arguments against pharmaceutical companies, but some of her most strident accusations are that:
1) Not enough money is put into research and development (R&D).
2) Drug companies lack innovation and create too many "Me-Too" drugs.
3) Drug companies rely too much on tax-payer dollars to generate revenue.
4) The pharmaceutical industry is not an example of American "free enterprise" and is protected by the FDA and the U.S. Patent Office.
While I didn't include some of Angell's secondary claims (or solutions) in the above list, they can be briefly summarized as follows: drug companies should spend less on advertising and either pass the savings on to consumers or invest in more R&D, drugs should be imported from other countries, drug price controls should be implemented, and finally that drug companies are greedy and not philanthropic enough.
There are those who believe Angell's portrayal of the pharmaceutical industry is misleading and that her solutions are wrongheaded. Dr. Elizabeth M. Whelan, president of the American Council on Science and Health (it has a blog, too) has offered a concise refutation of Angell's work. For instance, Whelan has countered Angell's charges that the drug companies "lack innovation," produce unneeded "copycat" drugs and have produced no "new" drugs.
Over the past decade, pharmaceutical companies have conducted hugely sophisticated research at the molecular and cellular levels to uncover many new treatments for disease. In the past ten years, over 300 new drugs have been approved by FDA � including vaccines, medicines to treat AIDS, modest steps toward treating Alzheimer's, a spectrum of antidepressants, and of course miraculous cholesterol-lowering drugs. [Angell's assertion that] [t]he copycat or "me-too" drugs offer no benefits over existing drugs. . . is false as well: It is in the consumer's interest to have a variety of drugs to choose from when looking to treat a condition. Some will work better than others for various individuals and afflictions; some will be tolerated more, with fewer side effects. Can you imagine if only one statin (cholesterol-lowering) drug were available for your physician to prescribe for you � and you were allergic to it?To further illustrate that new drugs, and not just "me-too" drugs, are being developed, The Pharmaceutical Research and Manufacturers of America (PhRMA), an advocacy group for pharmaceutical research and biotechnology companies, just reported that there are currently 109 separate drugs for mental illness now being developed, all of which "are either in human clinical testing or awaiting approval by the Food and Drug Administration." (Additionally, their FAQ "The Real Truth About Drug Companies" offers an informative counterpoint to many of the common charges made against them).
Angell make's much of tax-payer money funding research that in turn benefits private companies. To this, the PhRMA counters
The research-based pharmaceutical industry spends more ($32 billion in 2002) on biomedical R&D than the NIH, whose total 2002 budget was $24 billion. . . . the U.S. Government funding contributes substantially to general advances in the health sciences, including basic research, but there is still a distinction to be made between basic research and start-to-finish development of a new drug therapy.Additionally, according to Whelan,
In a report issued to Congress in 2001, the National Institutes of Health dismissed the contention that government pays for most of the research for the best-selling drugs. Indeed, statistics indicate that the research-based drug companies spend more on research and development than NIH does, develop the vast majority of U.S. medicines, and are responsible for over 90 percent of the entire world's new drugs each year.This would seem to counter Angell's claim that pharmaceutical companies don't spend enough of their own money on R&D. As to her contention that they spend more on marketing and advertising than R&D, the PhMRA's most recent publication (PDF), which includes complete sources, details the misconceptions surrounding the marketing of drugs.
Along these lines, Angell challenges the widely regarded estimate that the cost of developing one new drug is approximately $802 million (this number comes from a peer-reviewed scientific journal). Instead she quotes a non-peer-reviewed study by Ralph Nader's Public Citizen organization, which claims that the real number is only $l00 million (an odd and shaky citation for the former editor of a prestigious, peer-reviewed medical journal).
In 2003, PhRMA member companies alone spent much more on R&D�an estimated $33 billion�than the entire industry spent on all combined drug promotional activities, $25.3 billion. Of this amount, pharmaceutical companies distributed over $16 billion worth of free samples to office-based physicians. . . The entire industry�s direct-to-consumer (DTC) advertising accounts for just $3.3 billion of total promotion, or 10 percent of R&D spending by PhRMA members alone�a percentage consistent with the spending levels of other major industries. The remaining $5.7 billion the pharmaceutical industry expended on marketing and promotion in 2003 was spent on office promotion, hospital promotion, and journal advertising. ["Pharmaceutical Marketing & Promotion," p.5]Further, according to the aforementioned PhMRA FAQ,
Industry critics often mistakenly cite a category from Securities and Exchange Commission (SEC) filings as the amount spent on marketing, but this category includes many expenses other than traditional marketing expenses.Additionally, many who defend the drug companies contend that advertising is an important informational tool that enlightens potential health care consumers. For instance, Whelan contends that
This category includes, for example, free medicines provided to medically indigent patients under companies� patient assistance programs; systems and IT support; distribution and shipping expenses; and corporate functions, including legal, communications, dues, procurement, plus utilities and property taxes.
most observers familiar with "direct to consumer" advertising say it plays an essential role in consumer education. Many people who have serious diseases or risk factors like hypertension, elevated cholesterol, asthma, and depression are not being treated. These ads can prompt consumers to discuss medication with their physicians.Angell believes some relief for American drug consumers can be found in importation of drugs from other countries. These drugs are cheaper because other countries, such as Canada, impress price controls on drug companies. However, with price controls come limited quantities. According to Robert Goldberg
The fact is, there is only a limited amount of drugs that can be supplied at price-controlled levels worldwide. No degree of safety and surveillance can change the laws of supply and demand. Europeans and Canadians are able to get quality drugs at lower prices only because Americans pay free-market prices that fuel research and development.Further, again according to Goldberg and others, price controls take away the drug companies' incentive to conduct research or to provide basic medications. This was illustrated with the recent flu vaccine shortage. Because of price controls, few companies found it profitable to produce the vaccines. As such, when one company's batch of vaccines was found contaminated, there weren't sufficient vaccine producers to step in and immediately fill in the gap. Similarly, if drug companies are required to give away drugs for free, they will lack the incentive, and resources, to embark on the innovative research so desired by Angell and others. Most importantly, as Don Hawthorne recently posted right here at Anchor Rising, any time government gets involved in health care, disaster ensues.
The task force notes that the high level of pharmaceutical R&D ultimately depends on revenues: Cut drug-company revenues, and you necessarily cut R&D. Its report goes on to estimate that �importation could result in between four to eighteen fewer new drugs being introduced per decade.�This estimate is supported by a recent Manhattan Institute study which found that applying relatively moderate price limits just to purchases under the new Medicare drug benefit � so not to all drugs � would reduce new drug investment by over $300 billion over the next two decades. This drop would consequently deprive many millions of ailing people of potential cures.
Government price controls are already shortchanging Europeans and Canadians. They have led to a decline in investment, with venture capitalists investing 15 times more in biotech companies in America than they do in the same number of European firms. Health systems and consumers must also spend more to treat chronic illness there because they don�t get new medicines as quickly or as widely as we do. German and British patients, for example, are less likely to receive new cancer drugs than Americans. Indeed, British cancer patients are still waiting to use Gleevec for leukemia. If we import price-controlled drugs, we will import these shortage-created side effects too.
As it is, the accusations made by Angell and others that the pharmaceutical companies are greedy should be tempered. Deroy Murdock writes, citing a report by the Hudson Institute ["A Review of Pharmaceutical Company Contributions: HIV/AIDS, Tuberculosis, Malaria and Other Infectious Diseases," Carol Adelman and Jeremiah Norris], that "nine major drug companies donated $2.135 billion worth of products and services to combat HIV/AIDS, TB, malaria, and other tropical ailments." Additionally,
Despite the alleged avarice of the "mean, nasty" drug companies, this $2.135 billion in medical charity far outpaced the financial commitment of "caring, loving" government agencies that reputedly "put people, before profits." Compare Big Pharma's foreign aid with that of public-sector donors in 2003:Hence, an industry accused of profiteering has contributed generously to those in need, far outstripping so-called charitable institutions.
The U.S. Agency for International Development's Global Health Budget stood at $1.374 billion.
The World Health Organization's budget was $1.37 billion.
European Commission spending on HIV/AIDS, TB, and malaria totaled $451 million.
Finally, and quickly, drug companies do face a threat to their bottom line: trial lawyers are seeking to generate their own revenue from lawsuits against Big Pharma, much as they did against Big Tobacco. As an example, the recent Vioxx controversy has placed Merck directly in the line of fire of Big Trial Lawyers.
Next up is a more acute presentation regarding the "solutions" of foreign drug importation and price controls.
December 28, 2004
Government Meddling Creates Marketplace Distortions, Increasing Long-Term Costs
Two big issues frustrate and anger all of us about health insurance:
First, our personal insurance is not portable. In other words, the insurance is �owned� by our employer and we, the covered individuals, lose our coverage when we leave our jobs.
Second, the spiraling costs of health care products and services.
We can all thank the government for both outcomes. They meddled in the marketplace and all we got for it was less personal freedom and higher costs.
In the aftermath of World War II, the government meddled in the marketplace when they implemented wage-and-price controls. There have been many unfortunate consequences since then. Subsequently, because it was impossible to give salary increases when labor contracts were being re-negotiated, the companies instead offered health insurance as a separate benefit or form of compensation. This created the unnecessary marketplace distortion that tied our health insurance to our employer. The government then meddled further in the marketplace when the IRS deemed such benefits to be non-taxable income. This created yet another unnecessary marketplace distortion where the consumer is sheltered from the true costs of health care services, which are paid for by third party payors.
The list of further costly marketplace distortions created by government meddling has only continued to grow, with potentially ominous long-term consequences. A 4-part series (I, II, III, IV) of postings by the blog site, Houston�s Clear Thinkers, mixes some of their own commentary with highlights from articles by Holman W. Jenkins, Jr. of the Wall Street Journal:
Politicians, being adaptable sorts, have come to embrace the third party payor system as a means for political handouts and cost shifting�To take an example�Connecticut legislators recently voted to mandate that health insurers cover at least $350 a year in wigs for chemotherapy patients. Who wouldn't want chemotherapy patients to have wigs? But now everybody in Connecticut who wants health insurance has to pay for wig coverage.No serious person doubts that our overreliance on third-party payment is the problem that will be solved -- or will lead to a government-run, single-payer system that controls costs by denying care. In our information-rich economy, the medical industry doesn't even publish price lists. Is this not downright weird and a sign change is desperately needed?
Duke University's Clark Havighurst�has noted that "the systematic hiding of health-care costs from those who pay them" gives rise to the ultimate "moral hazard," allowing politicians to spend the public's money on health care in ways the public would never choose for itself either in the marketplace or the voting booth.
He also notes the seldom-emphasized regressive nature of the transfer: "The United States has structured things so that lower and middle-income premium payers bear heavy burdens so that the elite classes can continue to enjoy the style of health care to which they are accustomed." [This occurs when the higher-paid worker, because of their higher marginal tax bracket, can shelter more of their health care costs than the lower-paid worker.]
Treating cost as a factor in medical choices is considered somehow illiberal, though it's the poor who've been priced out of the health-insurance market. But, say it again, in the final analysis there's nobody to "shift" costs to. The health-care bill always comes home to working Americans in the form of higher taxes, lower take-home pay or unaffordable health care.
[The standard answer is to] throw yet more tax money at health spending while avowing disingenuously that "the rich" will pay for it. But our indictment here is of the conditioned cowardice of the health-care policy community at large. How can you expect better�when the arbiters of good policy�judge candidate health plans by a single criterion: Which would commit the most resources to health care?
There not being unlimited funds to spend on health care, [these] plan[s] would only speed the day when politicians, no longer able to write blank checks with the private sector's money, would face directly the choice of whether to curb consumption or raise taxes to pay for it. That's the job description of Europe's national health systems, which are not exercises in beautiful egalitarianism but exercises in rationing for those not rich enough to jet off to a private clinic and get the treatment they seek.
A study by the National Center for Policy Analysis looks at some of the macro trends that have resulted from all these distortions created by government meddling:
[I]n 1960, out of total health care spending�55.5% was paid out of pocket,�22.9% by private third-party payers,�12.7% by state and local government, and only�8.9% by the federal government�This changed dramatically after the creation of Medicare and Medicaid. By 1980,�only 27.8% [was paid] out-of-pocket. Private third party payers picked up 32.1% and the federal government paid 29.2%...
In 1998,�the federal government was paying for�33.7%...Out-of-pocket spending diminished to 19.6% of the total, and third party payments grew to 36.8%...
Not surprisingly, the flood of new federal money and the decrease in out-of-pocket spending resulted in health care inflation and an increasing share of national income going to health care after 1965�[5.2% in 1960, 7.2% in 1970, 9.1% in 1980, 12.7% in 1990, and over 14% in last 5 years, per another study.]
In response to this alarming growth, the federal government imposed a series of new laws and regulations intended to slow health care inflation�
Despite all these efforts, health care costs continued to rise. Every year from 1965 through 1982, the nation endured increases in health care spending in excess of 10%...
Employers instituted a number of cost-containing efforts, including benefit redesign emphasizing outpatient care over inpatient treatment and programs such as second surgical opinions and preadmission certification�These programs had remarkable, if temporary, success�
But soon enough, health care inflation was back�Employers had succeeded in holding down costs for a time, but now they needed another strategy. They switched to managed care in massive numbers. From 1984 to 1990, HMOs and PPOs increased their share of the private benefits market from 7% to 34%, and they continued to grow through the 1990s, capturing 65% of the market in 1995. More recent estimates place managed care's market share at 85%.
The hope for managed care was that it would provide first-rate health care while restraining utilization and cost. Managed care was supposed to provide incentives to keep people healthy so they would consume fewer health care services. It was supposed to help patients bond with their primary care provider who would direct them to the most cost-effective services. It was supposed to educate patients to take better care of themselves and avoid expensive professional care for ordinary ailments. It was supposed to bring a new businesslike attitude to health care services.
...managed care organizations...had [some] success in holding down cost increases, but at a high price in employee morale and community relations�
All of us will continue to pay quite a price as long as the government meddles in the marketplace and creates costly distortion after distortion.
Projo Schizophrenic on Healthcare & Employment
As I noted at the time on Dust in the Light, the Providence Journal's editorial page recently made an astonishingly forward-looking suggestion:
The problem of job quality is complex, involving trade, education and other issues. But we hope that political leaders will take an especially close look at the health-care factor. Our employment-based health-insurance system is collapsing. Any policy that frees employers from the burden of insuring their workers -- and controls health-care costs -- would also free them to hire more people.
Today, however, it's the unacknowledged turnabout that's astonishing:
Meanwhile, employer mandates are not an untested idea. For three decades, Hawaii has required companies to cover their workers who put in at least 20 hours a week. The Hawaiian economy is doing all right.It's become the fashion in America to portray every corporate mandate as anti-business and bad for the economy. But that's not necessarily true. When you let some companies shift their workers' health-care costs onto more responsible companies, you are in effect imposing a tax on your most desirable businesses. And when the uninsured end up on Medicaid or in hospital emergency rooms, the public pays more.
We urge Massachusetts leaders and citizens to clear the cobwebs of old thinking and try a bold approach to health care. The richest and most progressive states are doing it, and Massachusetts should be among them.
I don't know anything about Hawaii, but here in a New England border town, living in Rhode Island and working part-time from home for a company in Massachusetts, I'm finally about to enter that month when the infamous Northern specter of heating the home will break my already slipping grip on solvency. The wherefore is simple: I can't find full-time work in the range that I incurred so much debt (and lost so many years) to reach.
My family is fortunate to have healthcare (at a cost) through the employer that I do have, and as I managed in December, there is at least the chance to find non-career jobs to meet necessities. Considering my family's circumstances, I'd say I'm particularly justified in asking this question of fellow citizens who are desirous of a place among the "most progressive states": If healthcare costs do discourage hiring — and I don't doubt that they do — what bizarre calculus leads one to conclude that we'd be better off forcing the less "responsible" companies, those offering jobs that don't generally supply healthcare, to supply it?
From where I sit, on the decidedly non-academic side of the theoretical divide, it seems plausible, if not probable, that the end result of an employer-based mandate for universal healthcare will be a worst-of-all-worlds situation. In the first editorial here noted, the Projo lamented that the jobs that are available are increasingly of the low-paying variety. In the second editorial, it laments that people without health insurance become a significant burden on the taxpayers. Who's going to pay for healthcare when even low-salary jobs become scarce?
Health Care & Big Pharma I: The Case Against "BP"
Angell's argument is best summarized by this paragraph contained within the aforementioned article:
Over the past two decades the pharmaceutical industry has moved very far from its original high purpose of discovering and producing useful new drugs. Now primarily a marketing machine to sell drugs of dubious benefit, this industry uses its wealth and power to co-opt every institution that might stand in its way, including the US Congress, the FDA, academic medical centers, and the medical profession itself.To my mind, she finds four central faults with the current situation.
1) Not enough money is put into research and development (R&D): Big drug companies spend more on marketing and administration and reap more in profits than they spend in R&D. Finally, the prices they charge for drugs are vastly disproportionate to the amount spent on their developing, to the advantage of the drug companies' bottom line.
According to Angell, "For the top ten companies, [R&D expenditures] amounted to only 11 percent of sales in 1990, rising slightly to 14 percent in 2000. The biggest single item in the budget is neither R&D nor even profits but something usually called 'marketing and administration'�a name that varies slightly from company to company. . . .These figures are drawn from the industry's own annual reports to the Securities and Exchange Commission (SEC) and to stockholders, but what actually goes into these categories is not at all clear, because drug companies hold that information very close to their chests. It is likely, for instance, that R&D includes many activities most people would consider marketing, but no one can know for sure. For its part, "marketing and administration" is a gigantic black box that probably includes what the industry calls "education," as well as advertising and promotion, legal costs, and executive salaries�which are whopping."
2) Drug companies lack innovation - Too Many "Me-Too" Drugs: Only a few truly innovative drugs have been developed in recent years. Most are so-called "me-too" drugs, which are drugs that are not substantially different than those already on the market. There are two reason for creating these drugs, both related to market share. First, they are those created by competing drug companies in hopes of cutting into the market share of an existing drug that was developed by a competitor. Second, they are created by a company to replace an existing drug that the same company had created but whose patent, and thus monopoly, is ending soon. (As and example, Angell offers drug-maker Schering-Plough's attempt to market and replace Claritin with an "improved" version called Clarinex).
3) Drug companies lack innovation - Tax Payers Generate Their Revenue: Most of the few innovative drugs were brought to market as a result of either tax-funded research at academic institutions or the National Institutes of Health (NIH) or from small biotechnology companies. These organizations then licensed their findings to the larger companies and received royalties based on this research. This has resulted in a sort of biotech incubator, mostly centered around universities, where a symbiotic relationship between Big Pharma, academic institutions, small biotech companies and the NIH uses tax dollars to generate revenue. Further, the barriers between "pure" research for knowledge and research for profit have been broken down and a "pro-industry" bias has crept into academic institutions.
4) The pharmaceutical industry is not an example of American "free enterprise.": Big Pharma is excessively reliant on a "government granted monopoly," via patent rights and Food and Drug Administration (FDA) approval of their drugs, to maintain profitability. Through the FDA and the U.S. Patent office, as well as legislations such as the Hatch-Waxman Act, the effective life of a patent has been extended from eight to fourteen years since 1980. To maintain this situation, pharmaceutical companies have become particularly good at political lobbying and have retained an army of lawyers to press their case. Finally, many "American" drug companies are really just components of foreign-majority owned international corporations.
However, Angell believes that not all is rosy for Big Pharma and that though they still have vase reservoirs of wealth, there is potential trouble on the horizon. Drug companies became increasingly reliant on prescription co-pay provisions in company health care plans. In the '90's, as tax revenue increase, these provisions were particularly increased in government worker health programs. With the decline in revenues brought about by the recent recessions, various government entities have taken steps to reduce the burden of drug prices on their plans. Thus, the profits of drug companies have taken a hit.
There are additional problems. American consumers are increasingly looking "offshore," to Canada and Europe, for cheaper drugs via reimportation. Many successful drugs will be coming off their patents in the next few years with no similar inovative drugs to replace them. The pharmaceutical companies are putting too much faith in the human genome mapping project to generate genetic-based "miracle" drugs to cure ills. Finally, the industry is under a slew of investigations, "overcharging Medicaid and Medicare, paying kickbacks to doctors, engag-ing in anticompetitive practices, colluding with generic companies to keep generic drugs off the market, illegally promoting drugs for unapproved uses, engaging in misleading direct-to-consumer advertising, and, of course, covering up evidence."
In her article, Angell outlined two suggestions (there are more in her book). First, she suggests the FDA become more stringent in approving new drugs. Simply put, if they offer nothing new, then they shouldn't be approved. This would eliminate the "me-too" drugs and encourage innovation. It would also decrease the necessity of marketing one's version of the same drug to consumers, making more money available for R&D. Her second suggestion amounts to drug companies being required open their books so that what exactly such designations as "marketing and administration" cover can be discovered. Besides these two, she also alludes to breaking the dependency that academic researchers and medical professionals have on Big Pharma and to lessening the "inappropriate control drug companies have over the evaluation of their own products."
Next up will be the case for Big Pharma (or perhaps more appropriately, against Angell).
December 27, 2004
Health Care and "Big Pharma": Laying the Groundwork for Debate
It seems the latest "must-have" book for those who have cast the drug companies in the role of antagonist in this battle is The Truth About the Drug Companies: How They Deceive Us and What to Do About It by Marcia Angell. (Angell has presented this work in a shorter format here). To this, Elizabeth M. Whelan has responded. Additionally, the role of lawyers cannot be dismissed, as some see lawsuits against pharmaceutical companies as a lucrative proposition. Finally, the drug companies have provided their own reasons for high drug costs (such as too much consumer consumption [though it was only a joke, MAC]), and have their own organizations countering the claims of their opponents.
As a latecomer to the issue, I fully recognize that the depth of the debate is such that a pithy comment is not sufficient. The amount that has been written on this topic is voluminous and difficult to wade through and the rhetoric thrown up by both sides also makes it difficult to decide whom to trust. While I have my own predispostions as to who I tend to believe, I am also mindful of the importance of setting inherent biases aside when analyzing the debate objectively. Given all that, I have a lot to read and digest before I believe I can offer any sort of substantive, much less unique, commentary. As such, consider this post the first tentative step into the health care forest. I have yet to sharpen my axe, but I have whetstone in hand.
November 22, 2004
From the Outside In
The Projo editorial board's comments on recent healthcare happenings in the state mention a strategy — perhaps a necessity — with much broader application:
We are unmoved by Blue Cross's complaint that United is "an out-of-state for-profit company." In all-too-cozy Rhode Island, being out-of-state can be an advantage, avoiding as it does the local cronyism that has characterized such creatures as Blue Cross & Blue Shield of Rhode Island.And calling Blue Cross a "not-for-profit" merely elicits a bitter chuckle. We immediately think of the conflicts of interest -- the most glaring being that Blue Cross Board Chairman Frank Montanaro also heads the state AFL-CIO.
As a conservative advocate (of sorts) in this state, I can confirm that outside help is just about the only hope for real change at a pace measurable in years rather than decades. Fortunately, just as the size of the state helped its problems to develop, it lessens the degree of attention required from wider-world groups. (Of course, for them to care at all, we've got to be laboring from within.)
November 17, 2004
Fixing Something Broken on Purpose
I've admitted before that I find healthcare to be an eye-glazing issue — especially in Rhode Island. Sometimes it seems reasonable to wonder whether that's an effect that the industry actively encourages. As William Gamble's analysis suggests (to my mind, anyway), Blue Cross of Rhode Island could hardly have been better designed for corruption if that had been the intention all along:
Both the law and the market provide six methods to stop agents from taking anything that is not nailed down. They are: 1) business failure, 2) the market for corporate control, 3) managerial duties required by law, 4) direct managerial financial incentives, 5) corporate-governance oversight, and 6) shareholder empowerment. None of these applies to Blue Cross.
His solution?
Try selling it. It must be worth something. Why does Rhode Island, a small state with a small insurance pool, need a separate Blue Cross? Why not merge it with Massachusetts Blue Cross? Why not a New England Blue Cross -- a company large enough to negotiate with all providers?
I've noticed, here and there around my life, that smaller groups — a school system, a town government, a small office in a limited market — are often infested with backstabbing and advantage-taking out of proportion to their actual significance. The temptation of becoming a small pond big fish seems apt to drive people mad. (Perhaps because a certain sort of person can become such a creature although he wouldn't survive in a broader pool.) But as anybody who becomes addicted to the Flash game Fishy! will learn, ambition quickly becomes its own undoing in an enclosed ecosystem, and unfortunately, the individual isn't likely to be the only one undone.
November 9, 2004
Politics... Bad for Your Health
Writing in the Providence Journal, Emily Harding of the Rhode Island Association of Health Underwriters lays out the general argument for some suggestions for improving the healthcare near-crisis in the state:
What made [national health insurance carriers] leave the state had nothing to do with the inability to compete with Blue Cross (which they had done for so many years, or else they wouldn't have stayed as long as they did), but it had everything to do with Rhode Island's unfriendly legislative atmosphere, which got worse and worse until it was so bad that they all left.National carriers have been on record for two years saying what changes are needed if Rhode Island wants to see competition return to its health-insurance market.
The suggestions seem reasonable, and just pushing those who run Rhode Island to do something about the problem — other than reaching out for more centralized control — is absolutely critical. But here's the catch:
Can we count on our legislature to get the job done next session, so we might see some additional carriers back in Rhode Island, perhaps by next summer, along with much lower health-care costs and more choices? It remains to be seen whether our legislators will get the job done.
Well, that's the question of the decade. Interested citizens might find themselves wondering why it is so difficult in this state to make straightforward changes to address obvious problems. For starters, consider this little biographical summary from a recent Edward Achorn piece:
In many ways, Representative [Frank A. Montanaro (D.-Cranston)], 43, is the poster child of special-interest control of the General Assembly. It is their money -- especially the money of public-employee union groups allied to his father, who is head of the state AFL-CIO and State Association of Fire Firefighters -- that put young Frank in office at 25 and has kept him there for 18 years.Soon after his election, he obtained his state job, as assistant director of facilities at Rhode Island College, which pays him about $53,600 a year. Combined with his state representative's salary, he makes $65,880 a year directly from the taxpayers. ...
Immense political power seems to be concentrated in Montanaro's family. His father, of course, is the unelected governor, running Blue Cross & Blue Shield of Rhode Island, controlling the state Labor Relations Board and often chairing the state Economic Development Corporation. Young Frank's wife, Joy, a dental hygienist, is chair of the Cranston Zoning Board of Review. His uncle, Richard Crudele, ran the city's Building and Maintenance Department until Mayor Laffey took over. His cousin, former state Rep. Coleen Crudele, is chairman of Cranston's Board of Contracts and Purchasing.
How many Rhode Island legislators have similar reason to be disinclined to invite competition into the state? Higher healthcare costs to the RI taxpayer are a meager price to pay, considering the rewards of complicity.

 About Community Crier
About Community Crier

{kind=link}
{kind=link}